Variation in blood test monitoring practices for patients treated with conventional and biologic DMARDs
Joanne Ablewhite, Amy Fuller, Abdullah Almayahi, Abhishek Abhishek

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
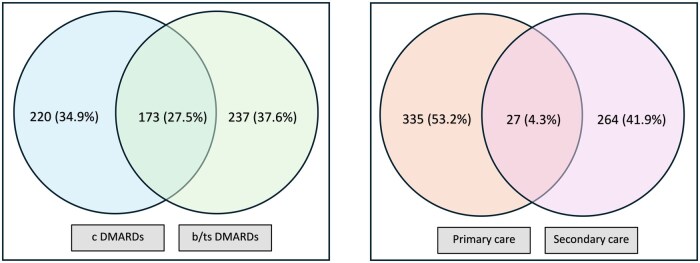 Figure 1
Figure 1- —National Institute for Health and Care Research—Health Technology Assessment Programme
- —NIHR10.13039/100006662
- —Department of Health and Social Care10.13039/501100000276
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSystemic Sclerosis and Related Diseases · Systemic Lupus Erythematosus Research · Celiac Disease Research and Management
Dear Editor, Between 11% and 35% of people prescribed DMARDs did not adhere to monitoring recommendations according to previous surveys conducted in the UK >20 years ago [1, 2]. Similar findings were reported from The Netherlands [3], while a study from Sweden reported 80% of patients with psoriasis with or without arthritis are not receiving recommended blood test monitoring while prescribed immunosuppressive treatments [4]. In recent years, the British Society for Rheumatology and other specialist societies have issued recommendations on the intervals between monitoring blood tests for the early detection of hepatic, haematological and renal adverse reactions to DMARDs [5, 6]. Whether this has standardized clinical practice in recent years has not been evaluated. We surveyed people with inflammatory conditions about the frequency of monitoring blood tests recommended to them by their clinical care team and their adherence with such recommendations.
We undertook a cross-sectional survey that was approved by the West Midlands Black Country Research Ethics Committee (Ref: 21/WM/0285). We recruited participants from rheumatology, dermatology, and gastroenterology clinics in National Health Service hospitals in Sheffield, Norwich and Nottingham and via advertisements promoted by the National Rheumatoid Arthritis Society, Crohn’s & Colitis UK, National Ankylosing Spondylitis Society, Lupus UK and Psoriasis Association. Eligible participants were required to be ≥18 years of age, diagnosed with an inflammatory condition (i.e. RA, Crohn’s disease, ulcerative colitis, psoriasis with or without arthritis, AS and SLE) and currently treated with a DMARD for ≥6 months. They self-reported age, gender, ethnicity, physician-diagnosed inflammatory condition, presence of pre-specified cardiovascular comorbidities and cardiovascular risk factors, the recommended interval between monitoring blood tests by their clinical care team and how often they did not comply with such a recommendation. Non-compliance was defined as either missing a blood test or delaying attending a blood test by >1 month in at least 2 of the previous 10 occasions. Number (%), mean (s.d.) and median [interquartile range (IQR)] were used for descriptive purposes. Data were analysed using Stata/MP (StataCorp, College Station, TX, USA).
Data for 630 eligible responders [613 (97.3%) White, 466 (74.0%) women] were included in this analysis. Their mean age was 34.36 years (s.d. 15.73). Their self-reported diagnoses were RA [n = 143 (22.7%)], psoriasis with or without arthritis [n = 113 (18.0%)], inflammatory bowel disease [n = 182 (28.9%)], AS [n = 179 (28.4%)] and lupus [n = 12 (1.9%)]. As shown in Fig. 1, among them, 220 (34.9%) self-reported being prescribed conventional DMARDs (cDMARDs) alone, 237 (37.6%) self-reported being prescribed biologic DMARDs (bDMARDs) or targeted synthetic DMARDs (tsDMARDs) alone and 173 (27.5%) self-reported being prescribed a combination of cDMARDs with bDMARDs or tsDMARDs. The usual place of monitoring blood tests was primary care for 335 (53.2%) participants, hospital for 264 (41.9%) participants and either primary care or hospital for 27 (4.3%) participants. Data on the location of monitoring blood tests were missing for four patients.
The median recommended interval between monitoring blood tests was 3 months (IQR 2–3) overall. Among those prescribed methotrexate (n = 203), thiopurines (n = 114) and leflunomide (n = 21), the recommended interval between monitoring blood tests was 3 (IQR 1–3), 3 (IQR 2–3) and 1 (IQR 1.5–3) months, respectively. In those prescribed bDMARD or tsDMARD monotherapy, the recommended interval between monitoring blood tests was 3 months (IQR 3–6) compared with 3 months (IQR 2–3) in those prescribed combined cDMARDs and bDMARDs or tsDMARDs. In those prescribed 5-aminosalicylic acid monotherapy (n = 19, 17 prescribed sulfasalazine), the median recommended interval between monitoring blood tests was 3 months (IQR 3–3).
A total of 51 (8.1%) participants missed or delayed by >1 month at least 2 of 10 previous monitoring blood test appointments. All of them were <60 years of age. This observation is limited by the fact that there were only 42 participants >60 years in age. Non-adherence was comparable in women [37 (8.0%)] and men [14 (8.5%)]. It was greater in magnitude in those prescribed bDMARDs or tsDMARDs alone [n = 28 (11.8%)] than in those prescribed cDMARDs alone [12 (5.5%)] and cDMARDs with bDMARDs or tsDMARDs in combination [11 (6.4%)].
In conclusion, we found substantial variations in the recommended frequency of monitoring blood tests in this large survey, suggesting the need to standardize monitoring, e.g. by developing a single national guideline issued by NICE. A limitation of this study is that we did not assess reasons for variations in recommended intervals between monitoring blood tests, e.g. due to risk factors of drug-induced toxicity, coexisting renal disease or the presence of abnormal baseline blood test results. These should be explored in future studies.
In general, patients adhered with monitoring blood tests. Adherence was lower in those <60 years of age and in those prescribed bDMARD or tsDMARD monotherapy. There were only a minority of people >62 years of age, and further research is needed in this population. These findings are limited by potential bias due to the self-reported nature of the data, which may have inflated the adherence estimates.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kay LJ , Lapworth K. Safety monitoring for disease-modifying anti-rheumatic drugs in primary and secondary care: adherence to local and national guidelines and patients’ views. Rheumatology (Oxford) 2004;43:105.14681561 10.1093/rheumatology/keg 437 · doi ↗ · pubmed ↗
- 2Helliwell PS , O’Hara M. Shared care between hospital and general practice: an audit of disease-modifying drug monitoring in rheumatoid arthritis. Br J Rheumatol 1995;34:673–6.7670788 10.1093/rheumatology/34.7.673 · doi ↗ · pubmed ↗
- 3Simon CH , Vliet Vlieland TP, Dijkmans BA et al Laboratory screening for side effects of disease modifying antirheumatic drugs in daily rheumatological practice. Scand J Rheumatol 1998;27:170–9.9645411 10.1080/030097498440778 · doi ↗ · pubmed ↗
- 4Krantz Å , Carrero JJ, Yang Y, Schalin L, Lysell J, Mazhar F. Psoriasis/psoriatic arthritis patients’ long-term treatment patterns and adherence to systemic treatments monitoring recommendations. Acta Derm Venereol 2023;103:6505.37318074 10.2340/actadv.v 103.6505 PMC 10281042 · doi ↗ · pubmed ↗
- 5Ledingham J , Gullick N, Irving K et al BSR and BHPR guideline for the prescription and monitoring of non-biologic disease-modifying anti-rheumatic drugs. Rheumatology (Oxford) 2017;56:865–8.28339817 10.1093/rheumatology/kew 479 · doi ↗ · pubmed ↗
- 6Warren RB , Weatherhead SC, Smith CH et al British Association of Dermatologists’ guidelines for the safe and effective prescribing of methotrexate for skin disease 2016. Br J Dermatol 2016;175:23–44.27484275 10.1111/bjd.14816 · doi ↗ · pubmed ↗