Endovascular treatment of a pseudoaneurysm in the right inferomedial genicular artery after arthroscopic anterior cruciate ligament reconstruction: a case report
Miguel Barrio Piqueras, Cristobal Varela, Angel Javier Muñoz Vázquez, Antonio Martinez de la Cuesta

TL;DR
A rare case of a pseudoaneurysm after ACL surgery was successfully treated with endovascular embolization.
Contribution
Presents a novel case of pseudoaneurysm in the inferomedial genicular artery after ACL reconstruction and its successful endovascular treatment.
Findings
A 47-year-old man developed a 24 mm pseudoaneurysm after ACL reconstruction.
Endovascular embolization using Squid Peri 18 successfully treated the pseudoaneurysm with no complications.
Anatomical variations like a high origin of the anterior tibial artery may contribute to such rare vascular injuries.
Abstract
Rupture of the anterior cruciate ligament (ACL) is a common knee injury, and reconstruction via arthroscopy is popular for its safety and low complication rate, around 1%. Vascular injuries from this procedure are extremely rare, with an incidence of 0.003%-1%. Pseudoaneurysms following knee arthroscopy are even less frequent. This paper discusses a rare case of pseudoaneurysm after ACL reconstruction in the articular branch of the right inferomedial genicular artery (IMGA), originating from an anterior tibial artery with a high origin. A 47-year-old man with Von Willebrand disease developed a 24 mm pseudoaneurysm 30 days post-ACL reconstruction. CT-angiography showed the pseudoaneurysm near the tibial tunnel screw and an unusually high anterior tibial artery origin. Emergency angiography confirmed this, and embolization using Squid Peri 18 was successful, with no complications. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
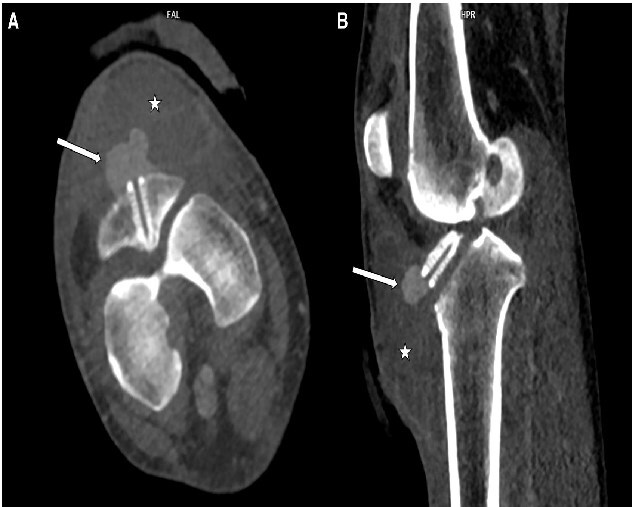 Figure 1
Figure 1 Figure 2
Figure 2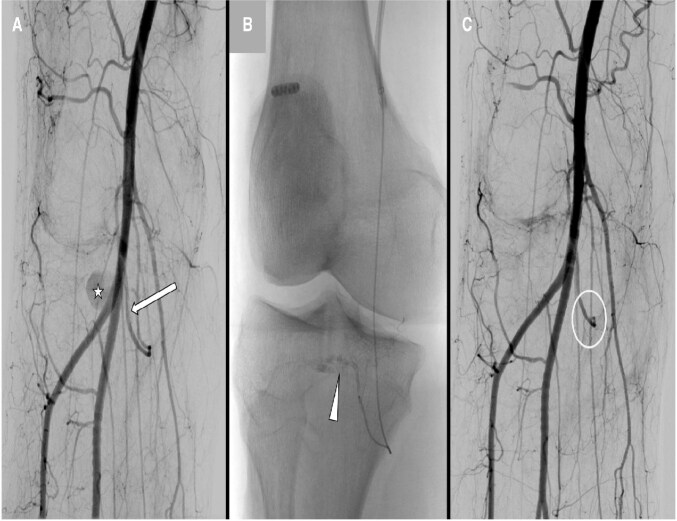 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Procedures and Complications · Venous Thromboembolism Diagnosis and Management · Knee injuries and reconstruction techniques
Background
Rupture of the anterior cruciate ligament (ACL) is one of the most prevalent knee injuries and consequently, the reconstruction of ACL is widely performed, commonly via arthroscopy. This technique is considered safe and has a low complication rate, with absolute risks associated with knee arthroscopy remaining minimal, at approximately 1%.1 Vascular injuries specific to this procedure are exceptionally rare, with studies indicating an incidence rate between 0.003% and 1%.2^,^3 Reports of pseudoaneurysm development after knee arthroscopy are significantly limited.
This paper presents a case of a pseudoaneurysm, developing after arthroscopic ACL reconstruction, in the articular branch of the right inferomedial genicular artery (IMGA), which itself arises from a right anterior tibial artery with a high origin.
Case presentation
A 47-year-old man, with a history of Von-Willebrand disease, was transferred to the Interventional Radiology department of our institution due to surgical wound dehiscence and suspected active bleeding 30 days after undergoing right ACL reconstruction. Upon admission, the patient was stable but showed a pulsatile swelling and signs of bleeding in the medial size of the treated knee. CT-angiography of the lower extremities revealed a significant haematoma associated with a 24 mm pseudoaneurysm, likely originating from the right IMGA that showed a downwards angulated origin. It was noted that the pseudoaneurysm was in close contact with the tibial tunnel screw (Figure 1). Additionally, an unusually high origin of the right anterior tibial artery (arising from the middle third of the right popliteal artery) was observed.
Axial (A) and sagittal (B) reconstruction of the CT angiography showing a haematoma (white star) and a hyperdense pseudonodular lesion in direct contact with the distal part of the tibial tunnel screw, compatible with a pseudoaneurysm.
Emergency angiography was performed straightaway, under local anaesthesia and sedation, in the Interventional Radiology suite. The procedure involved retrograde puncture of the left common femoral artery with ulterior catheterization of the right common femoral artery, using a Cobra 5F catheter (Cordis Medical Corp., Miami Lakes, FL, USA), followed by the advancement of a 5F introducer sheath (Terumo Europe N.V., Leuven, Belgium) to the distal right femoral artery. The angiography confirmed the CT-angiography findings and also demonstrated an IMGA originating from the anterior tibial artery (Figure 2). Subsequently, the IMGA was catheterized with a 2.0 F Merit Pursue microcatheter (Merit Medical Ireland Ltd, Galway, Ireland), and the pseudoaneurysm was embolized with SquidPeri 18 (Balt, Gland, Switzerland) (Figure 3).
(A) Angiography was performed from the distal right femoral artery, confirming the presence of the pseudoaneurysm (star) and revealing that the origin of the inferomedial genicular artery (IMGA) was indeed in the previously described high-origin anterior tibial artery (arrow). (B) Ulterior catheterization of the IMGA with more detailed visualization of IMGA disposition and the pseudoaneurysm.
(A) Pre-embolization image before treatment. (B) Administration of the embolic agent from the proximal portion of the inferomedial genicular artery. (C) Comparative arteriography after embolization, showing successful occlusion of the aneurysm.
No complications were observed during the follow-up.
Discussion
Pseudoaneurysms arise from a disruption in arterial wall continuity resulting from inflammation, trauma, or iatrogenic causes such as surgical procedures (in our case the tibial tunnel screw could have lacerated the arterial wall), percutaneous biopsy, or drainage. Under the influence of sustained arterial pressure, blood dissects into the tissues around the damaged artery and forms a perfused sac that communicates with the arterial lumen. The perfused sac is contained by the media or adventitia or simply by soft-tissue structures surrounding the injured vessel.4
Regarding knee procedures, the most commonly reported incidence of vascular injury and, consequently, pseudoaneurysms, occurs following total knee arthroplasty.5
As mentioned earlier, arthroscopy has a low complication rate. The absolute risk of complications associated with knee arthroscopy remains minimal, at around 1%.1 Vascular injuries are rare, with studies reporting an incidence between 0.003% and 1%.2^,^3
Pseudoaneurysms of the IMGA after arthroscopic ACL reconstruction are highly unusual and rarely described in the literature.6^,^7
Pseudoaneurysms can be treated with ultrasonography-guided compression, ultrasonography-guided thrombin, injection, open surgical ligation of the involved vessels, embolization by a microcatheter, or insertion of an endovascular stent.8
The traditional treatment for pseudoaneurysms has been surgical repair, but surgery has several drawbacks, including prolonged hospitalization, the requirement for general anaesthesia, and poor wound healing in patients with comorbidities. Additionally, surgery carries a higher risk of complications and mortality compared to interventional radiology techniques. Advances in technology have led to the increased use of interventional radiology, which is now the preferred treatment. However, surgery remains the gold standard for infected pseudoaneurysms, rapid expansion, ischaemia, neuropathy, and cases where percutaneous or endovascular treatments have failed.9
In our case, due to the presence of a significant haematoma, the risk of active bleeding and the possibility of an immediate endovascular access to the feeding vessel, the endovascular approach was performed with a successful outcome and a minimal recovery time for the patient.
Various embolic materials may be used for embolization of pseudoaneurysms, and the choice depends on various factors with no specific guidelines.
The decision to use a liquid agent in this case was due to the inability to advance the microcatheter beyond the proximal portion of the feeding artery due to its small calibre. By using a liquid agent that will flow across the pseudoaneurysm neck, distal and proximal embolization (sandwich technique) will be achieved, thereby preventing incomplete occlusion and development of collateral circulation.
A further point that makes this case particularly interesting is the presence of an unexpected anatomical variant consisting of an IMGA originating from the anterior tibial artery and not from the popliteal artery, together with a high origin itself of the anterior tibial artery from the middle third of the popliteal artery. To our knowledge, this variation has not been described before.10
Conclusion
Vascular injury is an extremely rare complication of knee surgery; however, there should be awareness for its occurrence in order to establish an early diagnosis and treatment.
The possibility of anatomical variants should always be considered to ensure a faster and more effective therapeutic approach.
Endovascular treatment of iatrogenic pseudoaneurysms is a fast, feasible, and safe technique that yields excellent results and enables quick post-procedural recovery.
Learning points
Inferomedial genicular artery pseudoaneurysms are a rare complication of arthroscopic anterior cruciate ligament reconstruction.However, it is essential to consider this complication due to its high risk of haemorrhage. Awareness of this possibility allows for timely intervention and appropriate planning to manage potential vascular complications effectively.Endovascular treatment has proven to be a safe, straightforward, and effective approach for addressing this complication, significantly reducing the risks associated with open surgical management.Awareness of potential anatomical variations in knee arterial vascularization is crucial during procedural planning to avoid prolonged surgery times and reduce unnecessary radiation exposure.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Friberger Pajalic K , Turkiewicz A, Englund M. Update on the risks of complications after knee arthroscopy. BMC Musculoskelet Disord. 2018;19:179. 10.1186/s 12891-018-2102-y 29859074 PMC 5984803 · doi ↗ · pubmed ↗
- 2Neagoe RM , Bancu S, Muresan M, Sala D. Major vascular injuries complicating knee arthroscopy. Videosurgery Other Miniinvasive Tech. 2015;10:266-274. 10.5114/wiitm.2015.52559 PMC 452085426240627 · doi ↗ · pubmed ↗
- 3Janssen RPA , Reijman M, Janssen DM, van Mourik JBA. Arterial complications, venous thromboembolism and deep venous thrombosis prophylaxis after anterior cruciate ligament reconstruction: a systematic review. World J Orthop. 2016;7:604-617. 10.5312/wjo.v 7.i 9.60427672574 PMC 5027016 · doi ↗ · pubmed ↗
- 4Saad NEA , Saad WEA, Davies MG, Waldman DL, Fultz PJ, Rubens DJ. Pseudoaneurysms and the role of minimally invasive techniques in their management. Radio Graphics. 2005; 25:S 173-S 189. 10.1148/rg.25si 05550316227490 · doi ↗ · pubmed ↗
- 5Wilson JS , Miranda A, Johnson BL, Shames ML, Back MR, Bandyk DF. Vascular injuries associated with elective orthopedic procedures. Ann Vasc Surg. 2003;17:641-644. 10.1007/s 10016-003-0074-214534848 · doi ↗ · pubmed ↗
- 6Mello W , de Brito WE, Migon EZ, Borges A. Pseudoaneurysm of the medial inferior genicular artery after anterior cruciate ligament reconstruction. Arthroscopy. 2011;27:442-445. 10.1016/j.arthro.2010.10.01521353173 · doi ↗ · pubmed ↗
- 7Filho ES , Isolani GR, Baracho FR, de Oliveira Franco APG, Ridder Bauer LA, Namba M. Pseudoaneurysm after arthroscopic procedure in the knee. Rev Bras Ortop (English Ed. 2015;50:131-135. 10.1016/j.rboe.2015.03.001PMC 451956126229905 · doi ↗ · pubmed ↗
- 8Farber A , Angle N, Avgerinos E, et al The society for vascular surgery clinical practice guidelines on popliteal artery aneurysms. J Vasc Surg. 2022;75:109S-120S. 10.1016/j.jvs.2021.04.04034023430 · doi ↗ · pubmed ↗