Spontaneous rupture of a bicornuate uterus at 19 weeks gestation: A case report
Joudi Tarabishi, Fatima Breim, Aya Laila, Hibatullah Alhammoud

TL;DR
A rare case of spontaneous uterine rupture at 19 weeks is reported in a woman with a bicornuate uterus, highlighting the importance of considering this condition in mid-trimester abdominal pain.
Contribution
This case report highlights the rare but severe obstetric complication of uterine rupture in a bicornuate uterus during mid-pregnancy.
Findings
Spontaneous uterine rupture occurred at 19 weeks gestation in a woman with a bicornuate uterus.
Surgical exploration confirmed a ruptured left uterine horn with hemoperitoneum and fetal demise.
Management included excision of the ruptured horn and repair of the uterine defect.
Abstract
A bicornuate uterus (BU) is one of the four principal abnormalities resulting from defective embryological development of the Müllerian ducts, associated with increased risks of miscarriage, preterm birth, and malpresentation. This case report describes a rare instance of spontaneous uterine rupture in a 31-year-old woman with a bicornuate uterus at 19 weeks of gestation. She presented with severe abdominal pain and signs of hypovolemic shock. Ultrasound revealed a single dead fetus, and surgical exploration confirmed uterine rupture with the deceased fetus free in the abdominal cavity and significant hemoperitoneum. The ruptured left uterine horn was excised, and the uterine defect was repaired. The patient's postoperative recovery was uneventful. A bicornuate uterus is a rare anomaly that can lead to serious obstetric complications at any stage of pregnancy. In our case, despite the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
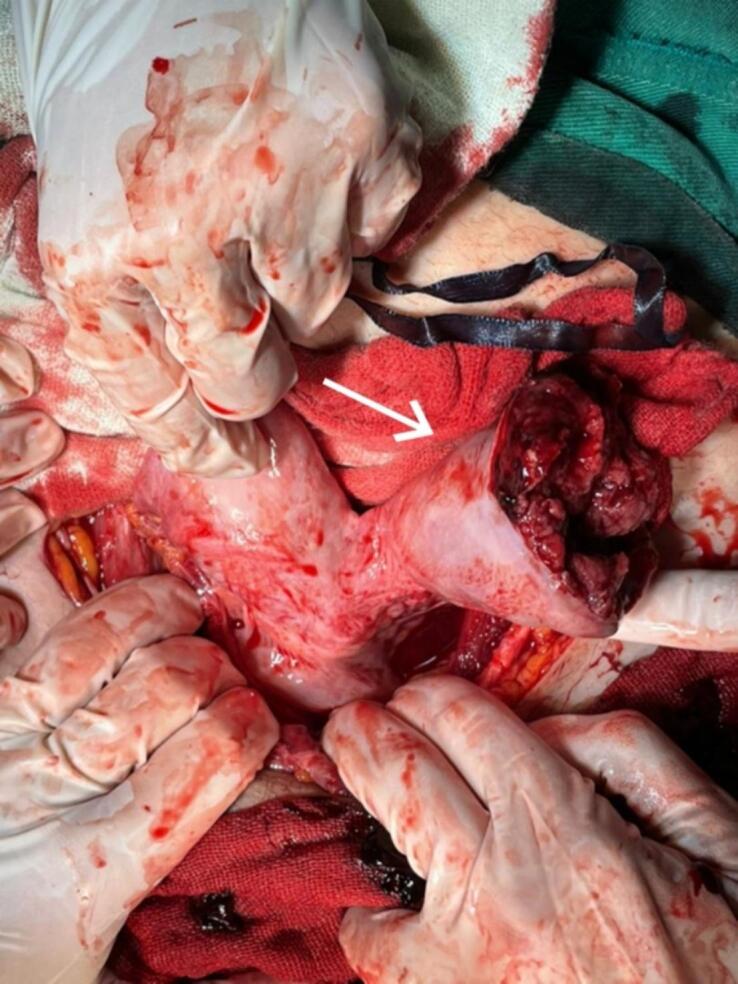 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGynecological conditions and treatments · Maternal and fetal healthcare · Uterine Myomas and Treatments
List of abbreviations
Unlabelled TableBUbicornuate uterusEDEmergency DepartmentBPDbiparietal diameterFLfemoral lengthICUintensive care unitWBCwhite blood cellsABGarterial blood gasesPROMpremature rupture of membranesPPROMpreterm premature rupture of membranes
Introduction
1
A bicornuate uterus (BU) is a rare congenital anomaly resulting from the incomplete fusion of the two Müllerian ducts during embryonic development, leading to a uterus with two distinct horns. This condition poses significant reproductive challenges and is associated with adverse outcomes [1].
Among the various types of Müllerian duct anomalies, BU accounts for approximately 25 % of cases [2]. Its prevalence varies from 0.4 % in the general population to between 1.1 % and 4.7 % among women experiencing reproductive issues [3].
Women diagnosed with BU may face several obstetric complications, including mid-trimester miscarriages, preterm labor and delivery, malpresentation, and antepartum and postpartum hemorrhage; however, uterine rupture remains a relatively rare event [3].
Rupture of the gravid uterus is a rare but serious obstetric emergency characterized by high morbidity and mortality rates. This complication is more frequently observed in multiparous women or those with a history of uterine surgery, such as cesarean sections or myomectomies, and typically occurs during labor [4]. In contrast, uterine rupture during early gestation—specifically in the first and second trimesters—is uncommon and is often associated with uterine anomalies like a bicornuate uterus or cornual pregnancies [4].
This case report discusses a spontaneous uterine rupture in a woman with a bicornuate uterus during the second trimester of pregnancy, emphasizing the critical need for awareness and careful monitoring in these high-risk situations.
The work has been reported in line with the SCARE criteria [5].
Case presentation
2
A 31-year-old G5P4004 woman, who has undergone one cesarean section a year ago, presented to our Emergency Department (ED) in March 2024. The woman was at 19 weeks of gestation according to her family with unmentioned last menstrual period (lactation period). The patient was unconscious with hypovolemic signs (hypotension, thready weak rapid pulse, pale skin color with peripheral cyanosis). Her family mentioned recurrent vomiting episodes with an average of seven times during the past 3 h. At the ED, sudden spasmodic movements occurred lasted for 3 min. The previous four pregnancies were uneventful. There was no history of either curettage or intrauterine device insertion. Additionally, she had no history of drug use, abdominal trauma, or smoking.
On physical examination at the time of admission, she was pale and unconscious, with a tender abdomen, muscle guarding, and unstable vital signs (hypotension = 70/40 mmHg, thready tachycardia = 110 bpm, and temperature = 36.5 °C). A vaginal exam revealed slightly opened external orifice with no observed vaginal bleeding.
Obstetric ultrasound examination showed a single dead fetus (absent fetal cardiac activity), normal amniotic fluid amount, with mostly placenta coverage, biparietal diameter (BPD) = 19 weeks, and femoral length (FL) = 17 weeks.
As there were no apparent signs of an obstetrical issue, the initial management was to enhance the general state of the patient by providing a venous line, maintaining the airway passage open, supplying well-hydration via saline solution and proton-pump inhibitor drugs, inserting a foley catheter, and requesting blood units.
After an extensive pre-operative laboratory tests were conducted (Table 1), three screened, cross-matched whole blood and two fresh frozen plasma units were transfused.Table 1. Laboratory results.Table 1. TestOn admissionOn dischargeNormal rangeBlood groupA+ positiveHemoglobin (g/dL)7.68.411.0–16.0Hematocrite (%)21.422.036.0–48.0White blood cells (WBC) (10^3^/μL)19.722.74.0–10.0Platelets (10^3^/μL)361206150–400Prothrombin time (s)14.514.5Activity (%)77 %77 %INR1.131.13C-reactive protein (mg/dL)30.4Up to 7Fasting glucose (mg/dL)191Glucose (mg/dL)153Urea (mg/dL)3310–40Creatinine (mg/dL)1.6410.6–1.1Lipase (U/L)228Up to 180Amylase (U/L)133Up to 80Alanine aminotransferase (U/L)15Up to 41Aspartate transaminase (U/L)2246Up to 40LDH (U/L)488623200–420Fibrinogen (mg/dL)440150–400Fibrin degradation products (F.D.P) (mg/dL)70–5D-dimer (ng/dL)7600–400Magnesium (mg/dL)1.91.7–2.4Total calcium1.69Ionized calcium (mmol/L)1.230.871.1–1.3Sodium (mmol/L)142141.9135–145Potassium (mmol/L)3.83.983.5–5.5Chloride (mmol/L)10410698–107Blood filmRed blood cell: normochromic normocytic; white blood cells: leukocytosis; neutrophelia few large immature cellsPlatelets: normal
A second abdominal ultrasonography was done after 1 h of admission, it showed excessive free fluid during the peritoneal cavity without organic hematomas. However, chest-X-ray was normal without subdiaphragmatic free gas or visceral perforation signs and an abdominal-X-Ray was normal without occlusion signs.
Two hours later, a general surgical consultation was conducted which revealed no emergency general surgical diagnosis after an extensive physical examination and radiological procedures check.
A diagnostic laparotomy was decided after an informed consent.
Intraoperative findings (Fig. 1) showed: 1) A massive hemoperitoneum of around 1.5 L of blood and blood clots. 2) A bicornuate uterus with a ruptured left horn. 3) Dead 19-week gestation embryo in the abdominal cavity (Fig. 2).Fig. 1A bicornuate uterus with a ruptured left horn.Fig. 1. Fig. 2Dead 19-week gestation embryo with attached placenta, and the left resected horn.Fig. 2
The management included: suctioning the hemoperitoneum, removing the placenta and fetus, and resecting the ruptured uterus horn and forwarding it to the pathology laboratory and suturing the defect using absorbable separated sutures, and eventually inserting two intraabdominal drainages. During the operation, three additional screened, cross-matched whole blood and three fresh plasma units were transfused. The woman was observed at the intensive care unit (ICU) for half a day and then was transferred to the ward where she stayed for one day before discharging.
The woman had an uneventful recovery and was discharged home on the fourth postoperative day. She was counseled about the high risk of recurrence and advised to avoid future pregnancies.
Outpatient follow-up was unavailable as the patient lived in an area with minimal socio-economic situation.
Discussion
3
A bicornuate uterus (BU) is a rare type of congenital uterine anomalies. BU is associated with increasing risks of obstetric complications including: miscarriage, placental abruption, premature rupture of membranes (PROM), preterm premature rupture of membranes (PPROM), fetal malpresentation at delivery, preterm delivery, cesarean delivery, fetal and perinatal mortality, and uterine rupture [1,6].
Most women with BU do not exhibit any symptoms, and the condition is often identified during pregnancy or childbirth when complications occur, or during abdominal surgeries like hysterectomy [3]. In our case, despite having undergone a previous cesarean section, neither the patient nor her family mentioned any uterine defects; after excluding general surgical diagnoses, a diagnostic laparotomy was conducted to identify the confirmed diagnoses.
Uterine rupture is commonly linked to a history of cesarean sections and multiple pregnancies. Additional risk factors include uterine anomalies, certain obstetric procedures, abnormal placentation, malpresentation, curettage, improper use of oxytocin, and long-term corticosteroid therapy [7]. In our case, a bicornuate uterus was identified as a significant risk factor, along with a prior cesarean section.
Uterine rupture manifests as an acute abdominal state that necessitates considering various obstetric, gynecologic and surgical differential diagnoses. Clinical presentation may include: acute abdominal pain, vaginal hemorrhage, and fetal distress and decelerations [8]. Obstetric and gynecologic differential diagnoses vary from ectopic pregnancy to ovarian torsion and ovarian cyst rupture [9]. In our case, the patient arrived at the emergency department with loss of consciousness, tenderness of abdomen, low blood pressure, and rapid heart rate, all indicating potential hypovolemia. A bedside ultrasound subsequently verified the existence of an indefinite massive free fluid in the abdomen.
The recommended management is prompt surgical resection of the ruptured horn. The subsequent procedure depends on the patient's desire of fertility. After counselling the patient about her plans and confirming her consent of termination of reproduction, hysterectomy is recommended, otherwise, the obstetrician needs to repair the uterus [3]. Our approach involved the prompt administration of blood, blood products, and fluid resuscitation to stabilize the mother's hemodynamics. This was followed by a diagnostic laparotomy to excision the ruptured left uterine horn and repair the uterus.
Regarding possible postoperative complications, a contraceptive plan should be discussed with the patient for at least a year after the operation.
As the pregnant suffering from uterus rupture will present with an acute abdominal state which will be challenging for the obstetrician to define the diagnosis, a rapid and prompt management should be administered regarding the patient's desire of fertility.
Conclusion
4
A bicornuate uterus (BU) is a rare congenital anomaly that may present with various obstetric complications. Uterine rupture should be considered as a differential diagnosis in each acute abdominal obstetric case at any gestational age. The initial management should include maintaining a stabilized maternal hemodynamic state by replacing blood products and fluids, followed by surgical intervention.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethics approval and consent to participate
Not required for case reports at our hospital. Single case reports are exempt from ethical approval in our institution.
Ethics approval and consent to participate
This study is exempt from ethical approval in our institution (Obstetrics and Gynecology University Hospital of Aleppo, Faculty of Medicine, University of Aleppo, Aleppo, Syria) because the content of the single case report does not require ethical approval.
Submission declaration
The article is not under consideration for publication elsewhere.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of competing interest
None.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hefny A.F.Kunhivalappil F.T.Nambiar R.Bashir M.O.A rare case of first-trimester ruptured bicornuate uterus in a primigravida Int. J. Surg. Case Rep.14201598100 Available from:10.1016/j.ijscr.2015.07.01926255004 PMC 4573601 · doi ↗ · pubmed ↗
- 2Singh N.Singh U.Verma M.L.Ruptured bicornuate uterus mimicking ectopic pregnancy: a case report J. Obstet. Gynaecol. Res.39120133643662269131110.1111/j.1447-0756.2012.01914.x · doi ↗ · pubmed ↗
- 3Abu H.Edweidar Y.Abu M.Abu I.Mid-trimester spontaneous rupture of a bicornuate uterus: a case report Case Rep. Women’s Health 39June 2023 e 00524 Available from:10.1016/j.crwh.2023.e 0052437954229 PMC 10636261 · doi ↗ · pubmed ↗
- 4Areys H.M.Omer N.H.Osman O.A.Second trimester spontaneous fundal rupture of unscarred bicornuate uterus in primipara: a case report and literature review Jigjiga University Sheik Hassen Yabare Comprehensive Specialized 2024181185(March)10.2147/IMCRJ.S 446718 PMC 1096053338524802 · doi ↗ · pubmed ↗
- 5Sohrabi C.Mathew G.Maria N.Kerwan A.Franchi T.Agha R.A.The SCARE 2023 guideline: updating consensus Surgical C Ase R Eport (SCARE) guidelines Int. J. Surg.10952023113611403701395310.1097/JS 9.0000000000000373 PMC 10389401 · doi ↗ · pubmed ↗
- 6Campo M.C.Milán F.P.Roig M.C.BartoloméE.M.Impact of congenital uterine anomalies on obstetric and perinatal outcomes: systematic review and meta-analysis Facts Views Vis. Obgyn.16120249223855147110.52054/FVVO.16.1.004PMC 11198883 · doi ↗ · pubmed ↗
- 7Walsh C.A.Baxi L.V.Rupture of the primigravid uterus: a review of the literature Obstet. Gynecol. Surv.625200710.1097/01.ogx.0000261643.11301.5617425811 · doi ↗ · pubmed ↗
- 8Toppenberg K.S.Hospital L.M.Uterine Rupture: What Family Physicians Need to Know 200282382812322775 · pubmed ↗