Cost-effectiveness of maintaining an active hospital microbiology laboratory service in Timor-Leste
Cherry Lim, Myo Maung Maung Swe, Angela Devine, Tessa Oakley, Karen Champlin, Pyae Sone OO, Nevio Sarmento, Ismael Da Costa Barreto, Rodney C. Givney, Jennifer Yan, Joshua R. Francis, Ben S. Cooper

TL;DR
This study shows that maintaining a hospital microbiology lab in Timor-Leste is cost-effective, reducing patient costs and deaths from bacterial infections.
Contribution
The study provides the first cost-effectiveness analysis of active microbiology services in a lower middle-income country like Timor-Leste.
Findings
Maintaining a microbiology lab reduces average patient care costs by $165,469 per 1000 patients with suspected bloodstream infection.
The service is estimated to reduce deaths by 34 to 51 per 1000 hospitalised patients.
The intervention is cost-effective due to reduced intensive care admissions and improved outcomes, especially for pediatric patients.
Abstract
Maintaining an active hospital microbiology laboratory allows definitive antibiotic treatment for bacterial infections to be given in a timely manner. This would be expected to improve patient outcomes and shorten length of hospital stay. However, many hospitals in low- and middle-income countries lack access to microbiology services, and the cost-effectiveness of an active microbiology service is unknown. We constructed a decision tree model and performed a cost-effectiveness analysis to determine whether maintaining an active microbiology laboratory service would be cost-effective in Timor-Leste, a lower middle-income country. The model was informed by local microbiology data, local patient treatment costs, results of an expert elicitation exercise and data from literature reviews. Compared with no active microbiology laboratory, average patient care costs would be reduced by…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
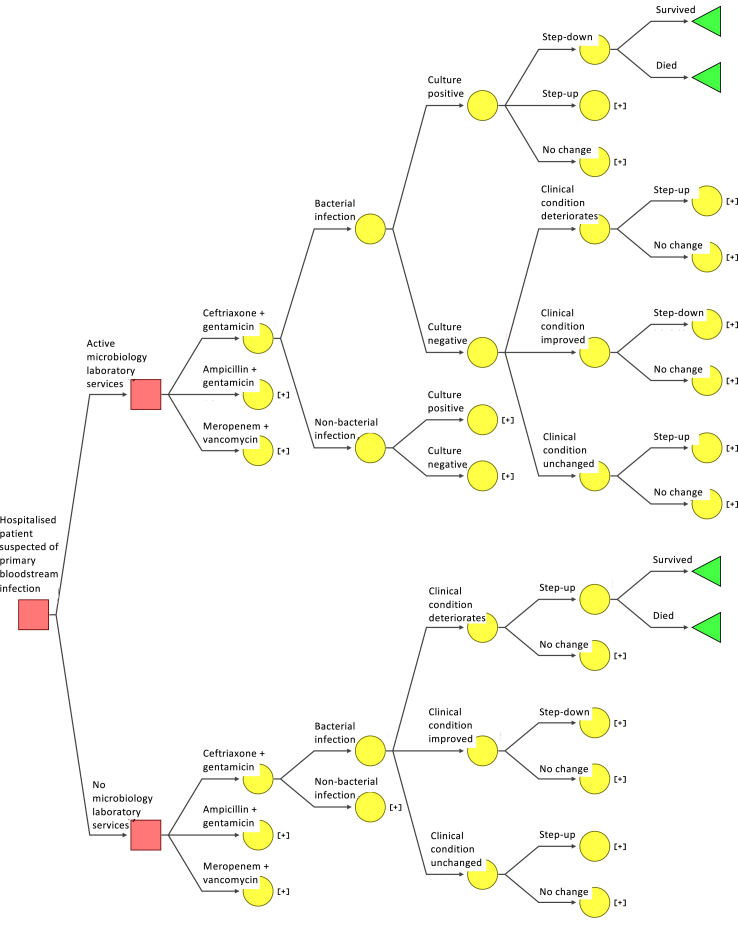 Figure 1
Figure 1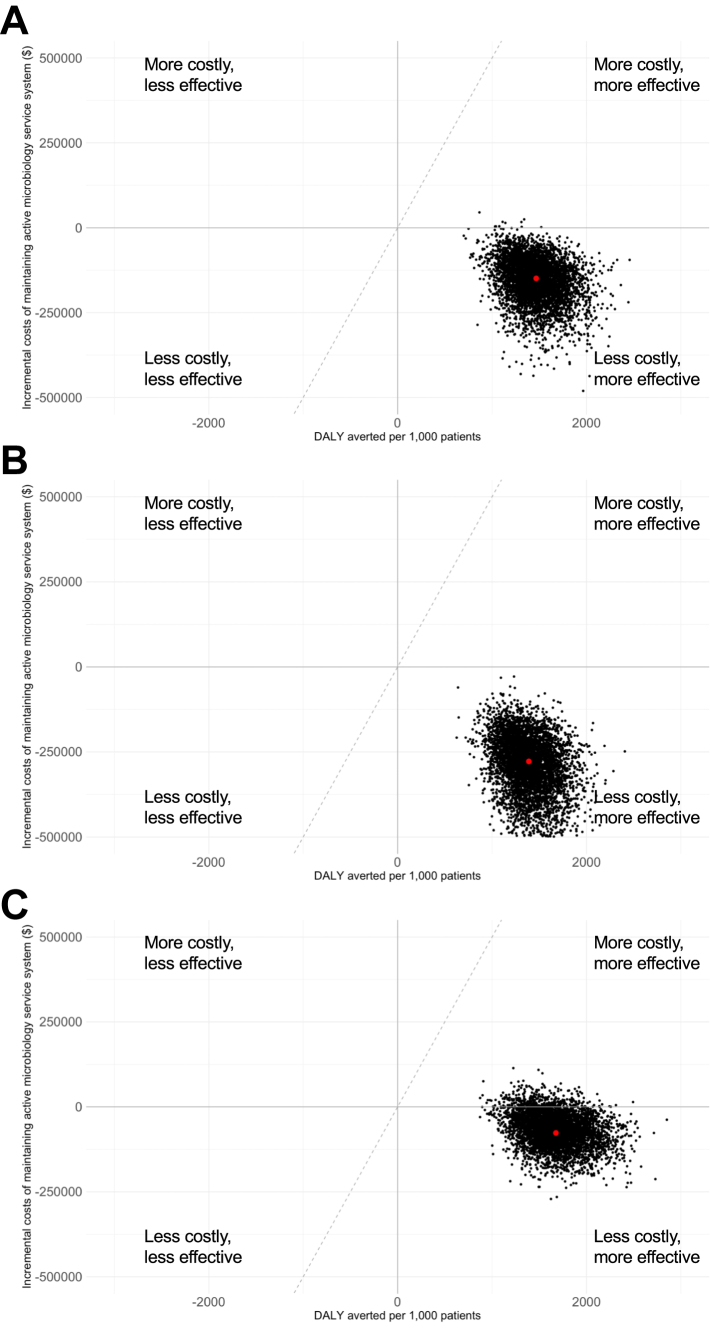 Figure 2
Figure 2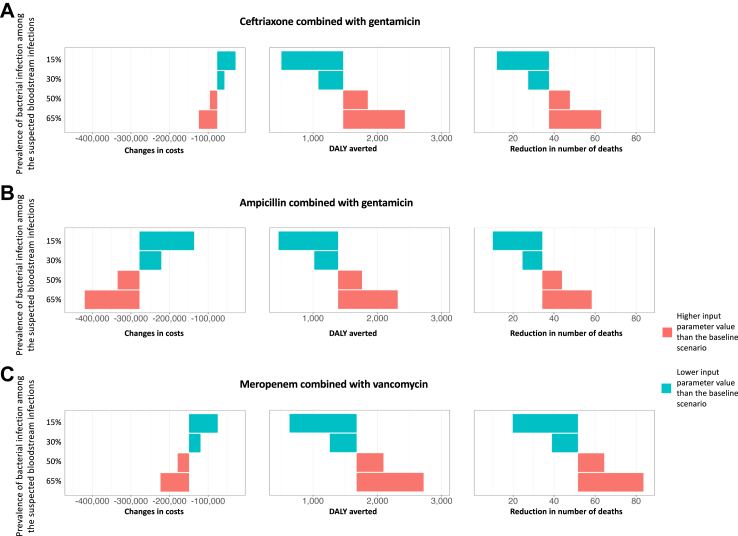 Figure 3
Figure 3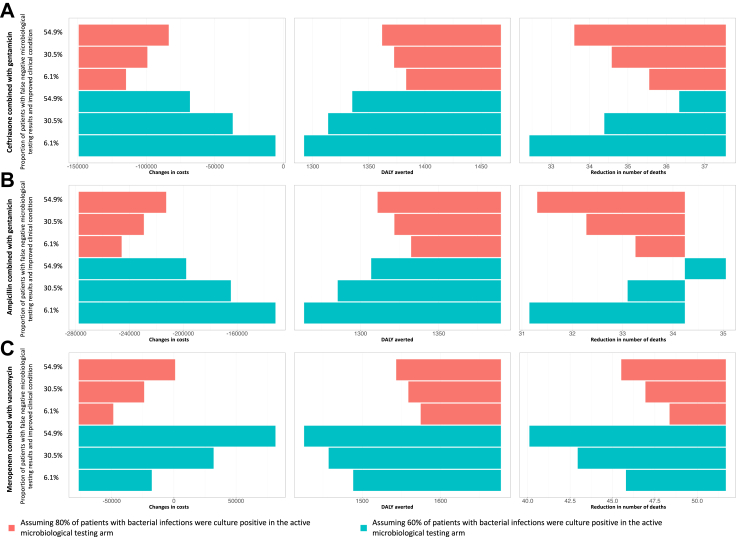 Figure 4
Figure 4- —10.13039/501100000276Department of Health and Social Care
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBacterial Identification and Susceptibility Testing · Antibiotic Use and Resistance · Nosocomial Infections in ICU
Research in contextEvidence before this studyTo identify existing literature related to cost-effectiveness evaluation of microbiology laboratory services, we searched PubMed for articles published in English with no date restriction using the search terms “cost-effective” AND (“diagnostic stewardship” OR “microbiology laboratory”). Through this search, we identified 12 papers focused on rapid diagnostic tests, 11 papers on different strategies of antimicrobial stewardship programmes, 8 papers on genomic diagnostic approaches, and 2 papers on imaging techniques. While one paper included an evaluation of the cost-effectiveness of surveillance for sepsis management in district level hospitals in Africa, this analysis considered only differences due to improved empirical prescribing (i.e. when the causative pathogen is not known), rather than individualised changes in prescribed antibiotics based on microbiology results.Added value of this studyOur study evaluates the cost-effectiveness of maintaining hospital-based microbiology laboratory services using detailed costing, microbiology and demographic data (including the most common age groups affected by suspected bloodstream infection) from a site in Timor-Leste. We found that there is a high probability that maintaining an active microbiology laboratory service is a cost-saving intervention. The policy is expected to not only improve patient outcome but also to reduce net costs primarily due to reduced ICU admissions. These conclusions were found to be robust to several sensitivity analyses.Implications of all the available evidenceMaintaining active microbiology services can lead to improved patient outcomes both due to improved empirical antibiotic treatment and due to individually targeted therapy, and may also save costs in LMIC settings. The results of this study further support existing guidance promoting diagnostic stewardship. Furthermore, our study provides evidence to support expansion of investment in local diagnostic capacity and has broad relevance for LMIC countries considering expanding microbiological diagnostic capacity or transitioning to sustainable government funding for such services. Trials to optimise the effectiveness of diagnostic stewardship are needed to improve implementation strategies.
Introduction
The emergence of antimicrobial resistance (AMR) is a global health threat, and the burden of AMR is highest in low- and middle-income countries (LMICs) with limited healthcare resources to respond to and monitor the spread of resistance.1 While international guidelines highlight the importance of diagnostic stewardship, the costs of microbiology testing in most settings are high. A conservative estimate of the cost for processing microbiology testing could range from 31 per specimen and from 304 per isolate.2 It is unknown whether maintaining an active microbiology laboratory would be overall cost-effective in improving patient care, while taking those costs into account.
Key reasons for potential reluctance to maintain active microbiology diagnostic testing services include low sensitivity of blood cultures,3^,^4 the required waiting time of more than 48 h for results to be available, and the relatively higher cost compared to empirical antibiotic therapy (often broad-spectrum antibiotic treatment).2 However, microbiology testing provides evidence-based guidance for targeted antibiotic treatment, which is potentially beneficial for reducing overuse of broad-spectrum antibiotics and, consequently, contributing to the control of antimicrobial resistance (AMR) spread.5 Moreover, microbiology testing results may direct clinicians to change management in cases where empiric antibiotic treatment does not cover the causative agent (e.g. in cases of Burkholderia pseudomallei infection or infection with antibiotic resistant pathogens) and would otherwise lead to mortality. Furthermore, aggregated microbiology data plays a vital role in designing and improving empirical antibiotic guidelines.6^,^7
A previous analysis of using blood culture surveillance in district hospitals in low to middle income countries in Africa to inform empirical antibiotic therapy policy in sepsis concluded that it was cost-effective for this purpose but not cost-saving.8 This study did not, however, consider whether the routine use of blood cultures for microbiologically-informed targeted antibiotic treatment in the patients tested was also economically rational.8 Given the growing threat of AMR, particularly outside high income settings, developing cost-effective interventions to reduce the associated burden of disease in low- and middle-income countries is increasingly important. The aim of the current study was to determine if, in Timor-Leste, a lower middle-income country, blood culture and susceptibility testing to guide individualised antibiotic therapy at tertiary referral hospitals is cost-effective, across three different empiric treatment regimens.
Methods
While local hospital active microbiological testing may provide many benefits, including providing information to support infection prevention and control programmes and to develop local empirical antibiotic guidelines, we consider only the health benefits arising from improved treatment of suspected bloodstream infection in hospital inpatients in this analysis. In this model, we assume the patient is hospitalised and is suspected to have a bloodstream infection.
Decision tree model
We consider two comparison arms and calculate expected costs and health-related outcomes including mortality and length of hospitalisation associated with each arm (Fig. 1). The decision trees were drawn in SilverDecisions 1.2.0 (https://silverdecisions.pl/), and all analyses were performed using R (version 4.0.5; The R Foundation for Statistical Computing, Vienna, Austria). The CHEERS checklist for the analysis can be found in Appendix 1. The analysis code is available at this link: https://github.com/Cherrylim128/CEA_maintain_active_microbiology.Fig. 1. Decision tree to estimate the cost-effectiveness of an active microbiology laboratory surveillance system compared to no microbiological testing. Squares indicate decision nodes, circles indicate chance nodes, and triangles indicate the end point. Collapsed branches of the tree are indicated by “[+]” and represent repeats of those shown at corresponding nodes on other branches of the tree.
In the active microbiology laboratory testing system arm, a patient with suspected bloodstream infection would have one set of blood sample bottles taken for testing, and be started on empirical antibiotic therapy before any potentially causative organism is identified. If bacterial pathogens are identified from those cultures, then definitive therapy based on the antibiotic susceptibility of the organisms may lead to the antibiotic regimen being changed. In the second arm, in which there is no microbiological testing, the patient would again be empirically treated, but any changes in treatment would be driven by clinical condition alone, without microbiological testing results.
In both arms, we consider three antibiotic regimens recommended at the time of writing in local guidelines for empirical antibiotic use in Timor-Leste: ceftriaxone and gentamicin, ampicillin and gentamicin, and meropenem and vancomycin.9 The first two antibiotic recommendations are also consistent with WHO recommendations for empiric antibiotics in clinical sepsis of unknown origin in adults and children respectively.10 Meropenem and vancomycin is a common antibiotic combination used in Timor-Leste for the critically unwell patient. Details on assumptions made on microbiology testing and antibiotic switching are in Appendix Text.
Populating the model
Transition probabilities
Each internal node of the decision tree has probabilities associated with each of the two or more branches splitting off from the main branch. These probabilities (which, for each node, must sum to one) represent either the probabilities of different decisions being made (e.g. step up, step down, no change) or probabilities relating to the patient's condition (e.g. clinical condition improves, deteriorates, or remains unchanged). These probabilities were derived from literature review,11, 12, 13, 14, 15 analysis of local hospital microbiology data from Timor-Leste and an expert elicitation exercise performed with physicians based at HNGV in Timor-Leste. Details of the expert elicitation are in Appendix 2, and detailed input values and references are in Appendix 3. Under the active microbiology laboratory service arm, there were four further transition events. These related to i) true bacterial infection state (which is imperfectly observed and is a “latent” variable); ii) microbiological testing result; iii) change in antibiotic treatment (assumed to be influenced by the microbiological testing); and iv) treatment outcome. Under the same arm when microbiological testing gave negative culture results, changes in antibiotic treatment were assumed to be based only on the clinical condition of the patient. In the no microbiological testing scenario, changes in antibiotic treatment were assumed to always depend only on the clinical condition of the patient regardless of the type of empirical antibiotic treatment received.
Under the active microbiology laboratory service arm, we assumed the antibiotic prescriber would receive one of two types of results from an active microbiology laboratory service: (a) culture negative, defined as no pathogenic bacteria growth after 5 days of culture, or (b) culture positive, defined as the growth of at least one pathogenic bacterium after 5 days of culture and with antimicrobial susceptibility test results available for the identified bacteria. We assumed that empiric antibiotics were administered for 3 days before re-assessing the treatment. Under the same arm when microbiological testing gave positive culture results, we assumed the transition probability of step-up could be reflected by the probability of coverage for each empiric antibiotic regimens11 from local microbiology data (See Appendix 3 for details on the probability of coverage calculation).
Costs
Appendix 4 shows the detailed cost breakdown and sources of data. All costs were in 2022 US dollars (1.76, 35.16, respectively. Costs for microbiology testing were derived from local data on laboratory equipment costs, antimicrobial-susceptibility testing (AST) costs, and maintenance costs of an active microbiology laboratory. The cost of one positive blood culture bottle (including microbiology culture, identification, AST, and other laboratory costs) was 5.80. We assume that each patient with suspected primary bloodstream infection would have two blood culture bottles taken for microbiological testing in the active microbiology laboratory service arm.
The costs of healthcare for patients were extracted from literature review and local staffing costs (Appendix 4). The cost of clinical deterioration was calculated based on the cost of patient care in an intensive care unit (ICU), and that of clinical improvement was based on the cost of patient care in a general medicine ward. Probability distributions were constructed to account for the uncertainty in costs of healthcare for patients. We also included the cumulative costs of antimicrobial resistance per full course of antibiotic treatment based on estimates from a previous study.16
The maintenance costs of an active microbiological testing laboratory were derived from local data provided by the local study investigator team. In brief, the per sample cost of maintaining an active microbiology laboratory could be as high as 24.96 (used in the sensitivity analysis to reflect a scenario with some external funding support). Both estimates accounted for the laboratory staff and space needed to maintain an active microbiology laboratory service. We summed the total additional costs (131,697) in 2023 for when the Fleming fund would only be partially available to support microbiology laboratory (used in the model for baseline scenario). We then divided these costs by the number of samples performed per year (3813 in 2021) to calculate the maintenance cost per sample.
Measurement of patient outcome
Disability-adjusted life years (DALYs) were calculated from mortality, length of hospitalisation, disability weights, and number of years lost for deaths. DALYs were calculated by estimating the sum of the years of life lost due to premature mortality (YLLs) and years of life lost due to time lived in states of less than full health, which is also known as the years of healthy life lost due to disability (YLDs). In other words, one DALY was the loss of one year of full health. The YLLs were calculated as the number of deaths multiplied by a loss function specifying the years lost for deaths as a function of the age at which death occurs, which is 11 years for patients in the age range of 55–59 years given the life expectancy of Timor-Leste population at birth of 70 years.12 This age group was chosen because this is one of the most common age groups for suspected bloodstream infections in Timor-Leste (unpublished data from National Laboratory Timor-Leste). YLDs were calculated from the length of hospitalisation after day of diagnosis with suspected bloodstream infection multiplied by a disability weight. The disability weight of severe acute episode of infectious disease used was 0.133 for adults based on the Global Burden of Disease (GBD) Study estimates.13 Patient mortality and length of hospitalisation given a specific trajectory of events were estimated based on evidence and inputs from experts working in hospitals in Timor-Leste. Details of outcomes, sources of data, and justification for the values are in Appendix 3–5. In addition, we performed a separate analysis with the same model but restricted to patients less than four years old, as prevalence of sepsis is high in this age group in the study hospital, assuming a loss function specifying the years lost for deaths as a function of the age at which death occurs was 66, and the disability weight for a severe acute episode of infectious disease for patients less than 4 years old of 0.402 was used.13
Measurement of cost-effectiveness
Results were expressed as an incremental cost-effectiveness ratio (ICER) for a hypothetical cohort of 1000 hospitalised patients with suspected bloodstream infection. This was calculated by dividing the difference in calculated cost between the two arms by the DALYs averted through having an active microbiology laboratory service:
which we report as the additional cost for every DALY averted per 1000 patients with suspected bloodstream infections.
Interventions and scenarios considered
Baseline scenario
In the baseline scenario, it was assumed that the prevalence of true bacterial infection among suspected primary bloodstream infections was 40%; and that the probability of pathogen detection and false positive rate of microbiological testing were 80% and 5%, respectively. Appendices 3 and 4 list the chances of having clinical condition deteriorate, improve or stay the same for each empirical treatment, as well as the probability of changing antibiotic prescription, which resulted from the expert elicitation exercise. The model assumed that the sensitivity of microbiological testing reflected both how well the microbiological testing can detect the causative organism and the bacterial load. For instance, if the bacterial load in a clinical sample was high the microbiological testing would be more likely to give a positive culture result and this would then impact the outcome of the patient.
Deterministic sensitivity analysis
We performed stepwise deterministic sensitivity analyses to check the robustness of the conclusions under various scenarios, including: i) low and high prevalence of bacterial infection among suspected bloodstream infections; ii) high cost of maintaining microbiology laboratory per tested sample; iii) different probabilities of changing antibiotic treatments; iv) low and high risks of ICU admission; v) low and high mortalities associated with different clinical conditions; and vi) different associated costs of care for patients whose clinical conditions deteriorated post empirical antibiotic therapy. Additionally, we performed a deterministic sensitivity analysis assuming the years lost for deaths was 20 years for patients in the age range of 55–59 years based on the WHO life table.14 Sensitivity analysis assuming two sets of blood cultures (four bottles) was also performed.
Probabilistic sensitivity analysis
A probabilistic sensitivity analysis was performed using 5000 iterations.17 In this analysis each parameter in the decision tree (Fig. 1) was defined by an appropriate probability distribution. Specifically, the probabilities attached to each internal node that has more than two probabilities (i.e. changes in clinical conditions) were sampled from Dirichlet distributions and binomial transition probabilities were sampled from beta distributions. For patient care costs, a lognormal distribution was used to avoid negative values. Details of the distributions used are in Appendices 3 and 4.
Role of funding source
The funder had no role in writing of this study. The views expressed in this publication are those of the authors and not necessarily those of the UK DHSC or its Management Agent, Mott MacDonald.
Results
Baseline scenario analysis
Active microbiology surveillance reduced overall patient care costs by 134,834–200,902) for every 1000 hospitalised adult patients with suspected bloodstream infection, primarily due to reduced ICU admission risk. Maintaining an active microbiology laboratory was consistently cost-saving compared to no active microbiological testing. It was most cost-saving in a setting where ampicillin and gentamicin was predominantly used as empiric treatment (Table 1). In settings where ampicillin and gentamicin, ceftriaxone and gentamicin, and meropenem and vancomycin were used as empirical antibiotic treatment, the estimated costs that an active microbiology laboratory would have saved were 149,341, and $76,597 per 1000 hospitalised patients with suspected bloodstream infections, respectively.Table 1. Estimated incremental costs and Disability-adjusted life years (DALYs) averted per 1000 hospitalised adult patients from maintaining a microbiology laboratory compared to no microbiological testing under the baseline scenario. Costs are in 2022 US dollars.Empirical antibiotic therapyAn active laboratoryNo active microbiological testingIncremental costs with an active laboratoryDALYs averted with an active laboratoryICERCostsDALYsCostsDALYsCeftriaxone + gentamicin523,3022636672,6434103−149,3411468Active laboratory dominatesAmpicillin + gentamicin537,7082640815,5874030−277,8791390Active laboratory dominatesMeropenem + vancomycin717,6702479794,2674156−76,5971677Active laboratory dominatesICER: incremental cost-effectiveness ratio.
For every 1000 hospitalised adult patients aged 50–59 years with suspected bloodstream infections, 37 (IQR: 31–44) deaths, 34 (IQR: 28–40) deaths, and 51 (IQR: 43–60) deaths would have been prevented with expanded microbiology testing capacity under the three choices of empirical antibiotic treatment (ceftriaxone and gentamicin, ampicillin and gentamicin, and meropenem and vancomycin, respectively). Similar findings were observed in the population with age under 4 years (Table 2; Appendix 6). For every 1000 hospitalised patients under 4 years of age with suspected bloodstream infections, 2575 (IQR: 2181–3025), 2329 (IQR: 1969–2761), and 3560 (IQR: 3038–4159) DALYs would be averted with an active microbiology laboratory under the three empirical regimens considered (Fig. 2).Table 2. Estimated costs saved and deaths averted per 1000 hospitalised paediatric patients (under four years of age) from maintaining a microbiology laboratory compared to no microbiological testing from a probabilistic model sensitivity analysis. Costs are in 2022 US dollars.Empirical antibioticCost saved (IQR) per 1000 hospitalised patientsNumber of deaths saved (IQR) per 1000 hospitalised patientsICERCeftriaxone + gentamicin277,855 (227,899–336,830)34 (28–40)Active laboratory dominatesMeropenem + vancomycin500, while points above this line would not be considered cost-effective at this threshold.
Factors influencing the cost-effectiveness of maintaining an active microbiology laboratory
The key factors that influenced the cost difference and DALYs averted between the intervention and control arm were prevalence of true bacterial infection among suspected bloodstream infections, patient characteristics (i.e. risks of ICU admission), cost of patient care in ICU, cost of maintaining active microbiological testing service, and patient age. The number of preventable deaths due to an active microbiology laboratory would be higher in a setting with a high prevalence of true bacterial infection, compared to that in a setting with low prevalence (Fig. 3). Maintaining an active microbiological testing laboratory service was more cost-saving per unit of increase in health benefit (smaller ICER and higher cost-effectiveness) in a setting with a high prevalence compared to a low prevalence of true bacterial infection. This could be explained by a proportionally increased number of true bacterial infections diagnosed by microbiological testing that would lead to timely appropriate treatments. In other words, the impact of overall delays in appropriate antibiotic treatment would be expected to increase proportionally with the increased number of true bacterial infections. The observation was further supported by the wider gaps in DALYs between the scenarios when narrow spectrum empirical antibiotics were used compared to scenarios using broad spectrum empirical antibiotics (meropenem and vancomycin, which have broader coverage compared to ceftriaxone and gentamicin or ampicillin and gentamicin).Fig. 3. The estimated changes in costs, Disability-adjusted life years (DALYs) averted and in number of deaths per 1000 hospitalised adult patients from maintaining a microbiology laboratory compared to no microbiological testing from deterministic sensitivity analysis for parameters related to prevalence of adult bacterial infection under (A) ceftriaxone and gentamicin; (B) ampicillin and gentamicin; and (C) meropenem and vancomycin empirical antibiotic treatment. The baseline scenario assumed that the prevalence of bacterial infection among the suspected primary bacteraemia was 40%. Note the differences in scale of the x-axis in the three plots. The length of the bars represents the magnitude of changes in cost (column 1), averted DALYs (column 2) and reduction in number of deaths (column 3) of maintaining active microbiological testing services compared to no microbiological testing.
In settings where false negative blood cultures resulted in highly detrimental clinical consequences (equivalent to those experienced by patients with bloodstream infections where the empirical treatment did not cover the causative organisms), the active microbiological testing service arm would still be cost-saving as long as the proportion of false negative is not high (Fig. 4). When meropenem and vancomycin were used as empirical antibiotic treatment and probability of culture positive among bacterial infections was as low as 60% and the probability of clinical condition improving among false culture negative (culture results showed negative among patients with bacterial infection) was as low as 1.4%, the ICER would be 2389)18 in 2022 in Timor-Leste), per DALY averted.Fig. 4. The estimated changes in costs, Disability-adjusted life years (DALYs) averted and in number of deaths per 1000 hospitalised adult patients from deterministic sensitivity analyses for parameters on clinical conditions of patients who had false negative cultures under the active microbiological testing arm. The analyses were performed independently for when (A) ceftriaxone and gentamicin; (B) ampicillin and gentamicin; and (C) meropenem and vancomycin were used as empirical antibiotic treatments. The dashed line represents incremental cost-effectiveness ratios calculated using base case parameters. The estimated proportion of patients with suspected primary bacteraemia and false negative blood cultures whose clinical condition deteriorated under the scenarios of ceftriaxone and gentamicin, ampicillin and gentamicin, and meropenem and vancomycin treatment were 39%, 39%, and 26%, respectively, based on the expert elicitations that meropenem and vancomycin treatment would have higher coverage rate than the other two treatment strategies. The length of the bars represents the magnitude of changes in cost (column 1), averted DALY (column 2) and reduction in number of deaths (column 3) of maintaining active microbiological testing services compared to no microbiological testing. The negative scales in costs changes suggests maintaining a microbiology laboratory is cost-saving compared to no microbiological testing.
When the cost of maintaining the microbiological testing service exceeds 3.78 per DALY averted. Similarly, sensitivity analyses assuming two sets of blood samples, which is equivalent to four sample bottles, found that maintaining the microbiological testing service is cost-effective and cost-saving under the scenarios in which ceftriaxone and gentamicin, and ampicillin and gentamicin were used as empirical treatments (Appendix 7). Empirical meropenem and vancomycin treatment would cost 13.31 per DALY averted, which is less than one GDP per capita. Presuming a setting with 40% prevalence of true bacterial bloodstream infections among suspected BSIs and using ceftriaxone combined with gentamicin as empiric treatment, the microbiology laboratory would need to be processing over 1200 samples annually (cost per sample 131,697 to maintain the service (Appendix 8). In the same setting but with meropenem combined with vancomycin as empiric treatment, maintaining an active microbiology laboratory service, while not cost-saving, would remain cost-effective (500 per DALY averted. In other words, assuming a fixed annual cost of 500.
Discussion
We modelled the cost-effectiveness of providing a blood culture service for HNGV in Timor-Leste, compared to not having this service. The model outputs in this study suggest that maintaining a microbiology laboratory service for this hospital is cost-effective in this lower middle-income country, even with the conservative parameter values used in the base case analysis. Our findings indicate that the microbiology laboratory service may be particularly important in reducing deaths in settings where the prevalence of bacterial infection among suspected bloodstream infection is high.
If the sensitivity of microbiological testing is low (with high rates of false negative tests), the cost effectiveness of maintaining a microbiology laboratory service would be reduced due to a higher proportion of patients needing ICU care due to delayed appropriate treatment. We found that if the sensitivity of microbiological testing was less than 60% and the probability of clinical condition improving in patients who were false culture negative was 1.4%, even under a low cost-effectiveness per DALY averted threshold of 2.5% GDP per capita in Timor-Leste (with 2389 of the GDP per capita[18](#bib18) in 2022), maintaining a microbiology laboratory service would be cost-effective compared to no microbiology testing. The cost-effectiveness thresholds estimated by Woods et al.[19](#bib19) using an empirical approach that adjusted for purchasing power parity were 1–51% GDP per capita (1–116) for Malawi, 4–51% GDP per capita (472–1786) for Indonesia.19 Accordingly, our results would be likely to viewed as cost-effective in Timor Leste. This remains true for an alternative health expenditure-based threshold of $1584 for Timor-Leste suggested by Pichon-Riviere et al.20
Steps to ensure high sensitivity of microbiological testing, including training focused on sample collection prior to antibiotics, and collection of adequate blood volumes for blood cultures, as well as laboratory quality assurance factors, remain important to ensure effectiveness treatment and optimise the value of microbiology testing. The US Centers for Disease Control and Prevention (CDC) recommended at least two blood culture sets (four bottles) should be obtained within a few hours of each other via peripheral venipuncture to increase sensitivity in detecting pathogens.21 A concern is whether such recommendations, which require additional costs, would still be cost-effective in resource-limited settings. The sensitivity analysis from the current study indicates that while increasing the number of bottles will increase costs substantially, the microbiological testing intervention would remain cost saving for when ceftriaxone and gentamicin or ampicillin and gentamicin were the recommended empirical antibiotic treatments (Appendix 7). For empirical treatment of meropenem and vancomycin, it would likely still be cost saving with an ICER of $13.
Based on the decision tree constructed, a narrower difference in costs between the microbiological testing service and no microbiological testing arms was observed in settings where meropenem and vancomycin were used to treat patients with suspected primary bloodstream infection compared to settings where ceftriaxone and gentamicin, or ampicillin and gentamicin were used. This was due to the high costs of meropenem and vancomycin compared to the other empirical antibiotic regimens considered (1.76 per day for ceftriaxone and gentamicin) and the fact that stepping-up to antibiotics such as colistin (assuming these antibiotics could be available in the near future in Timor-Leste) would impose large treatment costs. Moreover, based on the expert elicitation, empirical treatment with meropenem and vancomycin was less likely to result in deteriorating clinical condition compared with treatment with ceftriaxone and gentamicin or ampicillin and gentamicin. This in turn reduced costs of care and narrowed the cost gap between microbiological testing and no microbiological testing arms in settings where meropenem and vancomycin was appropriately used as empirical antibiotic treatment, noting the risks of contributing to further antimicrobial resistance with inappropriate empiric broad spectrum antibiotic use.
Timor-Leste is a relatively new country, gaining formal independence from Indonesia in 2002 with a current population of 1.3 million, predominantly rural (74%).22 Our case study analysis is based in Hospital Nasional Guido Valadares (HNGV), the tertiary referral hospital for the country, which located in the capital city of Dili with a 340-bed capacity.23 HNGV receives a microbiology service from the adjacent referral laboratory, Laboratorio Nacional de Saude. Previous studies have indicated a high rate of AMR in Timor-Leste.24, 25, 26 Since 2019, Timor-Leste has participated in the Fleming Fund project, a UK Government funded initiative which supports low- and middle-income countries to generate, share and use data to improve antimicrobial use and encourage investment in the prevention of antimicrobial resistance.27 Consequently, Timor-Leste has undergone significant laboratory strengthening activities including improvements to infrastructure, diagnostic test availability, and standardization of microbiology results. These activities combined with increased awareness of the benefits of surveillance have led to a significant increase in utilization of the diagnostic microbiology service. Health economic analysis of the cost effectiveness of a microbiology laboratory service is helpful for informing decision-making regarding ongoing government investments in tackling AMR in Timor-Leste.
There are limitations in this model. Firstly, the clinical inputs, such as mortality, are not based on actual collected patient data from the national hospital. We have assumed the same mortality rates for patients with bloodstream infections receiving different antibiotic regimens regardless of age (children and adults), and that having microbiological testing results available will lead to changes in antibiotic prescribing. These assumptions may not always be true, especially if the trust in microbiological testing results among antibiotic prescribers is low and antibiotic prescribing behaviour is influenced by alternate prescriber preferences and beliefs. Moreover, the model did not adjust for differences in model parameters by sex, age, socioeconomic status, and exploring how adding such complexity would change the conclusion is an area to be explored in the future. Secondly, the estimated cost saving in the active microbiological testing arm was driven largely by ICU costs. However, the assumption that reduction in ICU admissions in a given hospital translates proportionally to a reduction in costs when bed capacity and staffing level is maintained may not hold for all settings. Furthermore, the optimal method to cost hospital bed stays is an area of ongoing research.28 Thirdly, the long-term population and individual-level impact of antibiotic overuse were not systematically accounted for in this analysis. Finally, the model did not account for potential improvements from stepping down (for example due to fewer side effects or greater effectiveness of narrower spectrum antibiotic treatments). Neglecting this complexity represents a conservative assumption, which could lead to an underestimation of the potential health benefits of the intervention. Our conclusion that the intervention could provide health benefits and save costs will therefore be robust to this assumption, though more accurately capturing such complexity could be important to consider in future work or in settings where the benefits of the intervention are less clear.
Conclusion
The findings suggest that maintaining a microbiology laboratory service compared to no microbiological testing is likely to be cost-saving in the HNGV tertiary referral hospital in Timor-Leste, both reducing mortality and saving costs. These benefits primarily result from the fact that a microbiological diagnostic service enables severe bacterial infections to be treated with appropriate antibiotics in a timely manner which is expected to result in fewer ICU admissions and lower mortality. These results would be helpful for informing decision-making regarding ongoing government investments in tackling AMR in Timor-Leste. Finally, our analysis provides a framework for informing such investment decisions in other LMIC countries.
Contributors
CL & BSC: Conceptualisation, data management, data analysis, writing original draft, finalizing manuscript and approval; CL, TO, RCG and JY: Data management, data analysis, manuscript review and approval; CL, MMMS and PSO conceptualisation, data analysis, and collection for the expert elicitation exercise. AD, TO, KC, NS, IDCB, RCG, JY, and JRF: project resource, data curation, manuscript editing, manuscript review and approval; KC: project coordination. All authors have read and agreed to the published version of the manuscript. All authors contributed to interpretation, drafting and critical revision of the work, and final approval of the manuscript. All authors, both external and internal, had full access to all the data in the study (including statistical reports and tables) and take full responsibility for the integrity of the data and the accuracy of the data analysis.
Data sharing statement
Summary data underlying the results reported in this article are provided in the Supplementary Materials.
Declaration of interests
All authors declare no conflict of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Antimicrobial Resistance Collaborators Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis Lancet 3991032520226296553506570210.1016/S 0140-6736(21)02724-0PMC 8841637 · doi ↗ · pubmed ↗
- 2Roberts T.Luangasanatip N.Ling C.L.Antimicrobial resistance detection in Southeast Asian hospitals is critically important from both patient and societal perspectives, but what is its cost?PLOS Glob Public Health 1102021 e 000001810.1371/journal.pgph.0000018 PMC 761194734746931 · doi ↗ · pubmed ↗
- 3Connell T.G.Rele M.Cowley D.Buttery J.P.Curtis N.How reliable is a negative blood culture result? Volume of blood submitted for culture in routine practice in a children's hospital Pediatrics 119520078918961747308810.1542/peds.2006-0440 · doi ↗ · pubmed ↗
- 4Riedel S.Bourbeau P.Swartz B.Timing of specimen collection for blood cultures from febrile patients with bacteremia J Clin Microbiol 4642008138113851830513310.1128/JCM.02033-07PMC 2292961 · doi ↗ · pubmed ↗
- 5Tacconelli E.Sifakis F.Harbarth S.Surveillance for control of antimicrobial resistance Lancet Infect Dis 1832018 e 99e 1062910232510.1016/S 1473-3099(17)30485-1 · doi ↗ · pubmed ↗
- 6Lim C.Ashley E.A.Hamers R.L.Surveillance strategies using routine microbiology for antimicrobial resistance in low- and middle-income countries Clin Microbiol Infect 27102021139113993411158310.1016/j.cmi.2021.05.037PMC 7613529 · doi ↗ · pubmed ↗
- 7Global Burden of Disease 2021 Antimicrobial Resistance Collaborators Global burden of bacterial antimicrobial resistance 1990-2021: a systematic analysis with forecasts to 2050 Lancet 404104592024119912263929926110.1016/S 0140-6736(24)01867-1PMC 11718157 · doi ↗ · pubmed ↗
- 8Penno E.C.Baird S.J.Crump J.A.Cost-effectiveness of surveillance for bloodstream infections for sepsis management in low-resource settings Am J Trop Med Hyg 93420158508602617503210.4269/ajtmh.15-0083 PMC 4596611 · doi ↗ · pubmed ↗