Mid-ventricular hypertrophic cardiomyopathy with apical aneurysm: a multimodality imaging case report
Pavel Martinez-Dominguez, Manuel Horna-Noriega, María José Santa-Ana-Bayona, Sara Ramírez-Flores, Lucia Horna-Regalado, Nilda Espinola-Zavaleta

TL;DR
A rare heart condition with mid-ventricular thickening and an apical aneurysm was diagnosed using multiple imaging techniques in a 41-year-old man.
Contribution
This case report highlights the diagnostic value of multimodality imaging in a rare form of hypertrophic cardiomyopathy.
Findings
Mid-ventricular hypertrophy and apical aneurysm were confirmed using echocardiography and cardiac MRI.
The patient was at high risk for cardiac events and received an implantable cardioverter-defibrillator.
The case emphasizes the importance of advanced imaging in diagnosing complex cardiomyopathies.
Abstract
Mid-ventricular hypertrophic cardiomyopathy is a rare subgroup within hypertrophic cardiomyopathies that may present with apical aneurysm. This condition is associated with an increased risk of cardiac adverse events, including cardiac arrest, heart failure, thromboembolic events, or sudden cardiac death. We present a case of a 41-year-old man who presented with a history of exertional dyspnea and syncope. Multimodality imaging with echocardiography and cardiac magnetic resonance showed hypertrophy of the mid-ventricular segments with apical aneurysm. An implantable cardioverter-defibrillator was implanted to prevent sudden cardiac death.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
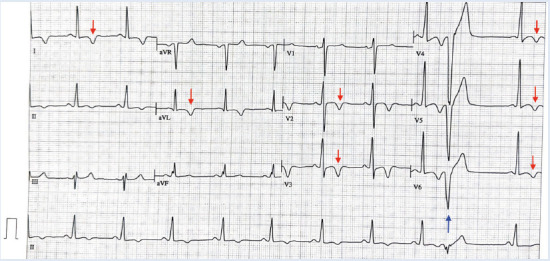 Figure 1
Figure 1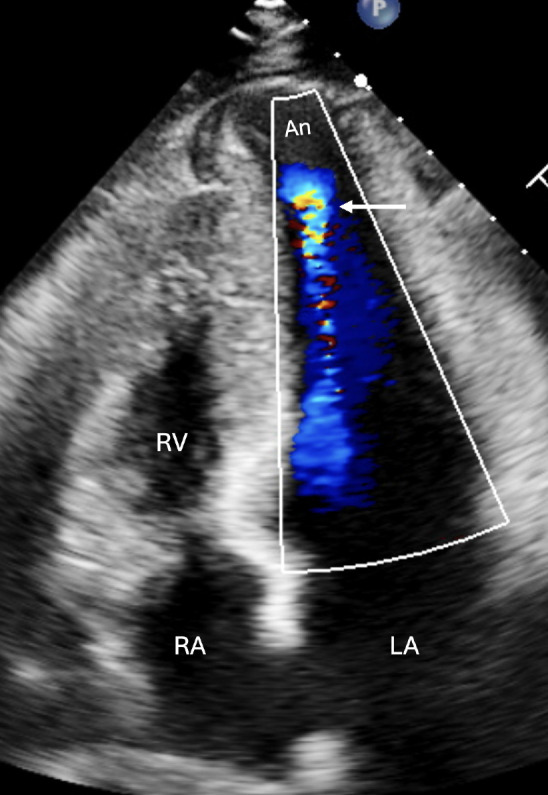 Figure 2
Figure 2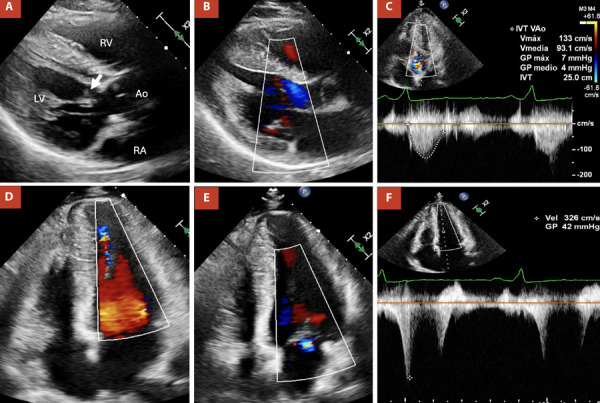 Figure 3
Figure 3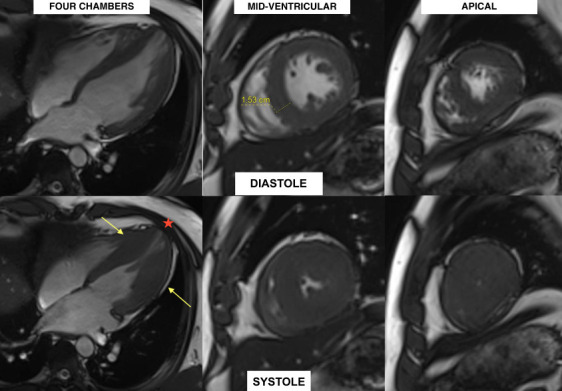 Figure 4
Figure 4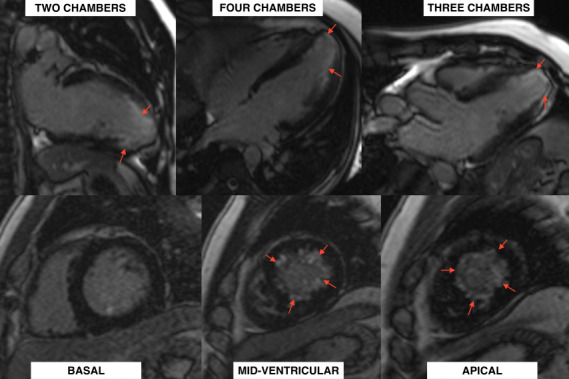 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiomyopathy and Myosin Studies · Coronary Artery Anomalies · Cardiac Structural Anomalies and Repair
Introduction
Hypertrophic cardiomyopathy is an inherited disorder that affects 1 out of 500 people and increases considerably the risk of sudden cardiac death (SCD). 1 Mid-ventricular hypertrophic cardiomyopathy (MHC) is a rare subgroup of hypertrophic cardiomyopathy that can present with apical aneurysm. Within this subgroup, an increased risk of adverse events, including cardiac arrest, heart failure, thromboembolic events or SCD, has been reported. 2
The presence of hypertrophic cardiomyopathy with apical aneurysm requires a close evaluation and assessment to determine the use of an implantable cardioverter-defibrillator (ICD) aiming to prevent SCD.
We describe a patient with history of syncope, preceded by shortness of breath. Echocardiography and Cardiac magnetic resonance (CMR) demonstrated mid-ventricular hypertrophic cardiomyopathy with apical aneurysm. After evaluation and SCD risk stratification, ICD was successfully implanted. This case report emphasizes the importance of a comprehensive assessment, including clinical presentation, imaging findings, and SCD risk evaluation, in determining the appropriate management approach.
Case report
A 41-year-old man with a 2-year history of hypertension presented with moderate exertional dyspnea and one episode of syncope. The patient reported no family history of cardiomyopathy or SCD. Upon admission, the vital signs were within normal limits, with a blood pressure of 125/72 mmHg, a heart rate of 67 beats/min, a respiratory rate of 17 breaths/min, and an oxigen saturation of 97%. Further examination revealed no significant findings.
An electrocardiogram (ECG) was performed, revealing sinus rhythm with 1:1 atrioventricular conduction, narrow QRS complex, and signs of left ventricular hypertrophy. Non-specific repolarization abnormalities were observed in precordial and high lateral leads, characterized by deep T wave inversions from V1 to V6 and leads I and aVL, as well as ventricular extrasystoles (Figure 1).
Figure 112-lead ECG revealing sinus rhythm with a heart rate of 63 beats/min. Sokolow-Lyon Criteria (S in V1 + R in V5 or V6) of 37 mm confirms left ventricular hypertrophy. Negative T waves measuring up to 5 mm in amplitude are present from V2 to V6, DI and aVL (red arrow). Premature ventricular contraction is observed (blue arrow).
Subsequent diagnostic assessment included a transthoracic echocardiogram (TTE). (Figures 2 and 3; Videos 1 and 2) This study reported a preserved left ventricle ejection fraction of 68%. However, there was evidence of hypertrophy in the middle-to-apical segments of the left ventricle, with a maximum wall thickness of 20 mm and a midventricular gradient of 42 mmHg. It also demonstrated signs of apical aneurysm with dyskinesia. Additionally, mild left atrial dilation (36 mL/m2), grade II diastolic dysfunction (E/A = 1.5, E’ = 4 cm/s), increased end-diastolic pressure (E/E’ = 15), and mild mitral regurgitation were observed.
Figure 2. Four-chamber transthoracic echocardiographic view with color Doppler, showing an apical aneurysm (arrow). Abbreviations: An, Aneurysm; LA, Left atrium; RA, Right atrium; RV, Right ventricle.
Figure 3A) Parasternal long-axis view showing redundant chordae tendineae (arrow). B) Parasternal long-axis view with color Doppler, demonstrating the absence of subaortic obstruction (Laminar flow). C) Apical five-chamber view with color and continuous-wave Doppler, showing no evidence of subaortic obstruction. D) Four-chamber view with color Doppler, revealing turbulence in the apical portion of the left ventricle. E) Four-chamber view showing mild mitral regurgitation. F) Four-chamber view with color and continuous-wave Doppler demonstrating apical obstruction with a maximum gradient of 42 mmHg, partially contaminated by mitral regurgitation flow.
A CMR was performed, which confirmed mid-ventricular hypertrophy of up to 15 mm in the infero-septal medial segment, along with the formation of an apical aneurysm (Figure 4). Late gadolinium enhancement (LGE) revealed patchy myocardial fibrosis in the middle and apical segments, accounting for less than 15% of the total left ventricular mass (Figure 5). No edema was detected in the T2 STIR and T2 mapping sequences.
Figure 4. Cardiac magnetic resonance with four-chamber, mid-ventricular and apical views during diastole (above) and systole (below) showing mid-ventricular hypertrophy of 15.3 mm (yellow arrows) with apical aneurysm (red asterisk). Increased trabeculations can be seen in anterolateral, basal, medial, and lateral apical segments.
Figure 5. Late gadolinium enhancement resonance with two, three, and four-chamber views (above) and basal to apical views (below) showing subendocardial late gadolinium enhancement in mid-apical segments less than 15% of the total ventricular mass (red arrows).
In addition, during an exercise stress test, a normal blood pressure response was observed, and no arrhythmic events were demonstrated in the 24-hour Holter monitoring. According to the 2020 AHA/ACC Guideline for the Diagnosis and Treatment of Patients With Hypertrophic Cardiomyopathy, 3 the patient had a 5.22% of SCD in the following 5 years. Considering the SCD-risk and imaging findings, the patient had a class 2A recommendation for the implantation of a cardioverter-defibrillator (ICD) for primary prevention, which was successfully implanted.
Discussion
Multimodal imaging is crucial in differentiating the etiology of myocardial hypertrophy, particularly in distinguishing hypertrophic cardiomyopathy from hypertensive heart disease and other infiltrative or metabolic disorders. 4^)^ Echocardiography remains the first-line modality, with characteristic findings varying by etiology. Hypertrophic cardiomyopathy typically presents with asymmetric septal hypertrophy, which can lead to dynamic left ventricular outflow tract obstruction (LVOT), often accompanied by systolic anterior motion (SAM) of the mitral valve.5 In contrast, hypertensive heart disease usually exhibits concentric left ventricular hypertrophy without LVOT obstruction and with preserved global longitudinal strain until later disease stages. 6
CMR provides superior myocardial characterization. LGE helps distinguish hypertrophic cardiomyopathy, which often shows patchy fibrosis at the right ventricular insertion points and in hypertrophied segments, from hypertensive heart disease, where fibrosis is more diffuse and subendocardial. Apical HCM, often underdiagnosed on echocardiography, is best visualized on CMR. 7 Meanwhile, amyloidosis is characterized by global LV thickening, diffuse subendocardial LGE, and markedly elevated native T1 and extracellular volume fraction. 8
MHC is a rare and infrequent form of hypertrophic cardiomyopathy, frequently associated with apical aneurysms. Apical aneurysms are present in less than 5% of patients with hypertrophic cardiomyopathy; however, they are more common in those with the mid-ventricular subtype. 9
The mechanism described for apical aneurysm formation is unclear. One mechanism suggests that an increased gradient between the basal and apical segments of the ventricle leads to elevated apical pressure and myocardial stress, culminating in wall weakening and formation of the aneurysm through a chronic and dynamic process.9
In patients with hypertrophic cardiomyopathy, echocardiographic criteria include a left ventricular thickness above 15 mm or above 13 mm if the patient has a first-degree relative with hypertrophic cardiomyopathy, in the absence of other causes of hypertrophy. Other signs of hypertrophic cardiomyopathy include mitral valve disease, left ventricle diastolic dysfunction, or mild atrial enlargement. 10
In our patient, the presence of these signs confirmed the important role of echocardiography in the assessment and diagnosis of MHC. Further examination with CMR allows to identify and measure the wall thickness, obstruction, and confirm the presence of aneurysms. 11 Moreover, CMR modalities such as late gadolinium enhancement, STIR, T2 are part of the routine evaluation in hypertrophic cardiomyopathy. 12
Patients with hypertrophic cardiomyopathy and late gadolinium enhancement are more likely to show a decreased ejection fraction and increased major adverse cardiac events.13 Thus, MHC represents a high-risk subgroup of hypertrophic cardiomyopathy, as reports have shown increased risk of ventricular arrhythmias such as nonsustained ventricular tachycardia (NSVT), sudden cardiac death, thromboembolic events, and heart failure. 2 NSVT mechanism is not well understood; however, it has a reported prevalence of 20%-30%.14 Additionally, there is an 8-fold increase in SCD in patients with hypertrophic cardiomyopathy accompanied by aneurysm than without aneurysms. 11
Initial treatment includes pharmacological therapy with beta-blockers and antiarrhythmics to prevent arrhythmias. 15^)^ Alternatives such as alcohol septal ablation, cryoablation and surgical myectomy may also be considered in patients with refractory symptoms despite medications. 16 Even though these interventions have shown good outcomes, further studies are needed to determine the appropriate timing and patient selection for these procedures. 17
Assessment of SCD is crucial during hypertrophic cardiomyopathy evaluation, as there are established risk factors for SCD, including age, family history, recent unexplained syncope, history of NSVT and echocardiographic parameters such as left atrial size, ventricular thickness, ventricular gradient.1 The 2020 AHA/ACC guidelines include left ventricular systolic dysfunction, apical aneurysm, and extensive LGE on CMR as risk factors for SCD. Risk stratification allows to determine if an ICD is necessary for primary prevention. 3
There is a difference between the current European and American guidelines regarding the role of aneurysm in sudden cardiac death. The ACC/AHA consider apical aneurysms as a risk factor for SCD and suggests ICD implantation in these patients, while the ESC guidelines suggest there is insufficient data and only consider apical aneurysm as class IIa for indication of ICD implantation. 4 However, after comprehensive evaluation of this patient, the cardiovascular team decided to implant an ICD to prevent future cardiac complications. This decision was supported by the presence of an apical aneurysm and the history of syncope.
In conclusion: MHC is a rare and high-risk subgroup of hypertrophic cardiomyopathies. The presence of apical aneurysm in these patients requires a comprehensive assessment including SCD-risk stratification to consider ICD implantation. We aim to underscore the importance of imaging in order to have a timely intervention and elucidate the significant role that ICDs play in SCD prevention within this unique subgroup, however further studies to understand how to appropriately manage these patients are needed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hong Y Su WW Li X Risk factors of sudden cardiac death in hypertrophic cardiomyopathy Curr Opin Cardiol 2022371152110.1097/HCO.000000000000093934636345 PMC 8654272 · doi ↗ · pubmed ↗
- 2Rowin EJ Maron BJ Haas TS Garberich RF Wang W Link MS Maron MS Hypertrophic Cardiomyopathy With Left Ventricular Apical Aneurysm Implications for Risk Stratification and Management J Am Coll Cardiol 201769776177310.1016/j.jacc.2016.11.06328209216 · doi ↗ · pubmed ↗
- 3Ommen SR Mital S Burke MA Day SM Deswal A Elliott P 2020 AHA/ACC Guideline for the Diagnosis and Treatment of Patients With Hypertrophic Cardiomyopathy Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines Circulation 202014225 e 533e 55710.1161/CIR.000000000000093833215938 · doi ↗ · pubmed ↗
- 4Pan JA Patel AR The Role of Multimodality Imaging in Cardiomyopathy Curr Cardiol Rep 202426768970310.1007/s 11886-024-02068-938753290 PMC 11236518 · doi ↗ · pubmed ↗
- 5Guigui SA Torres C Escolar E Mihos CG Systolic anterior motion of the mitral valve in hypertrophic cardiomyopathy a narrative review J Thorac Dis 20221462309232510.21037/jtd-22-18235813751 PMC 9264047 · doi ↗ · pubmed ↗
- 6Ismail TF Frey S Kaufmann BA Winkel DJ Boll DT Zellweger MJ Hypertensive Heart Disease-The Imaging Perspective J Clin Med 20231293122312210.3390/jcm 1209312237176563 PMC 10179093 · doi ↗ · pubmed ↗
- 7Burrage MK Ferreira VM Cardiovascular Magnetic Resonance for the Differentiation of Left Ventricular Hypertrophy Curr Heart Fail Rep 202017519220410.1007/s 11897-020-00481-z 32844347 PMC 7495998 · doi ↗ · pubmed ↗
- 8Lavall D Vosshage NH Ge Bner R Stobe S Ebel S Denecke T Native T 1 mapping for the diagnosis of cardiac amyloidosis in patients with left ventricular hypertrophy Clin Res Cardiol 2023112333434210.1007/s 00392-022-02005-235355115 PMC 9998594 · doi ↗ · pubmed ↗