Mechanistic classification of isolated severe aortic regurgitation in a contemporary cohort of patients
Rudy R Unni, Munir Boodhwani, Ibrahim Jelaidan, David T Harnett, Samia Massalha, Calvin Liang, Graeme Prosperi-Porta, David Glineur, Ian G Burwash, Kwan-Leung Chan, Thais Coutinho, Angel Fu, Nadav Willner, David Messika-Zeitoun, Luc Beauchesne

TL;DR
This study classifies the mechanisms of severe aortic regurgitation in patients and finds that leaflet prolapse is the most common cause, especially in those with bicuspid aortic valves.
Contribution
The study provides a contemporary classification of aortic regurgitation mechanisms and their surgical implications in a large patient cohort.
Findings
Leaflet prolapse (Type II) was the most common AR mechanism, observed in 48.6% of patients.
Bicuspid aortic valve patients had a higher frequency of multiple AR mechanisms compared to others.
Aortic valve repair was performed in nearly half of surgical interventions, highlighting the importance of mechanism identification.
Abstract
Aortic regurgitation (AR) arises from leaflet disease and/or dilatation of the functional aortic annulus complex. Understanding the mechanisms of AR informs surgical planning of valve and aorta repair. This study investigates the mechanisms, aetiologies, and outcomes of isolated native severe AR in a consecutive cohort of patients. Patients with moderate-to-severe (3+)/severe (4+) native valve AR, identified from our institutional echocardiography database (2014–2018), were included. Exclusions were significant concomitant valve disease, endocarditis, or aortic dissection. AR was classified per the El-Khoury system: Type I (normal leaflet motion: Ia–ascending aorta/sinotubular junction dilatation, Ib–aortic root dilation, Ic–aortic annular dilation), Type II (leaflet prolapse), and Type III (leaflet restriction). Valve anatomy and clinical outcomes, including mortality and surgical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
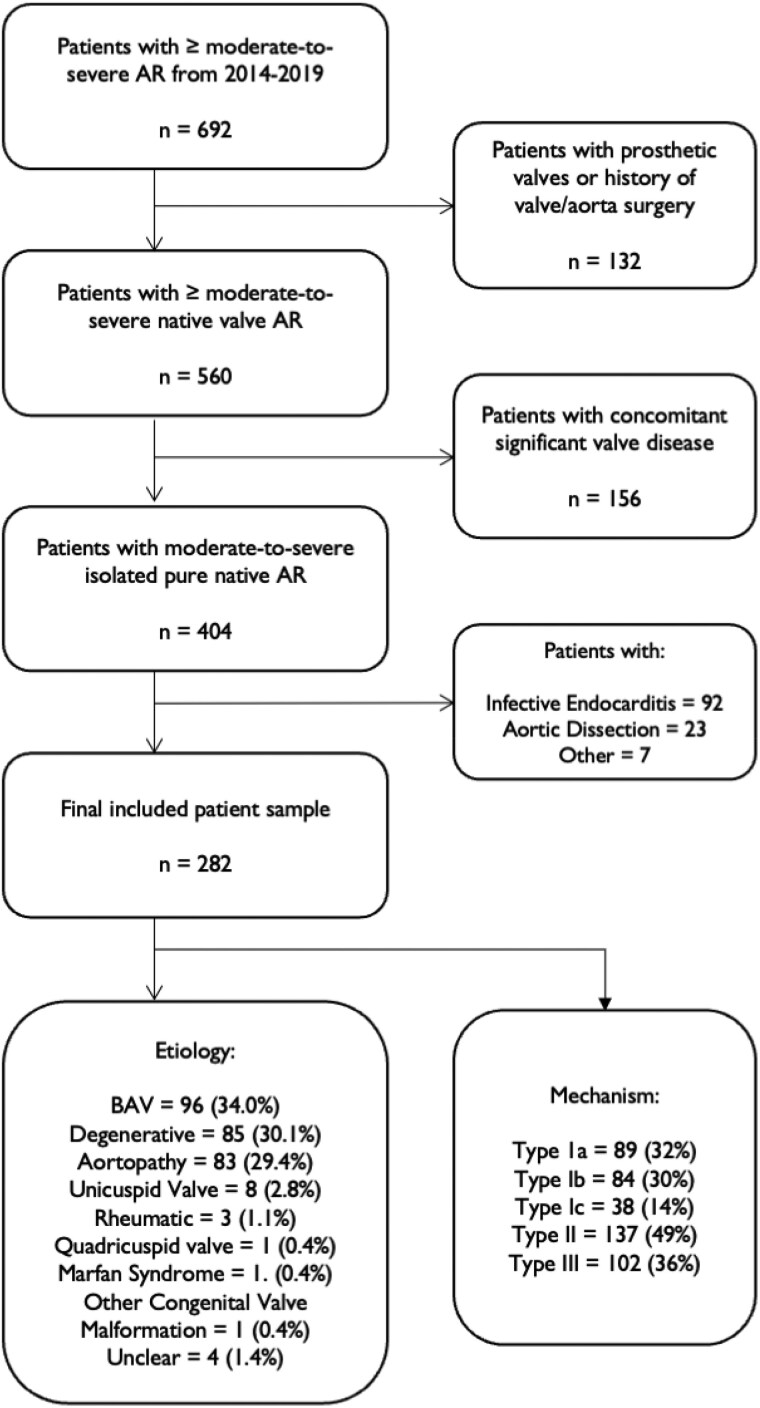 Figure 1
Figure 1| Characteristic | Patients ( | BAV ( | Degenerative ( | Aortopathy ( |
|---|---|---|---|---|
| Age, mean (SD), y | 59.6 (17.4) | 47.7 (15.6) | 68.6 (10.6) | 67.6 (13.8) |
| Male, | 218 (77.3) | 83 (86.5) | 62 (72.9) | 61 (73.5) |
| BMI, median (IQR), kg/m2 | 25.9 (23.4–29.6) | 26.0 (5.4) | 26.0 (6.3) | 26.0 (6.4) |
| Pulse pressure, MMHG (IQR) | 70 (59–87) | 68 (23) | 75 (29) | 77 (32) |
| Severity of AR, | ||||
| 3+ AR | 176 (62.4) | 57 (59.4) | 59 (69.4) | 49 (59.0) |
| 4+ AR | 106 (37.6) | 39 (40.6) | 26 (30.6) | 34 (41.0) |
| Valve anatomy, | ||||
| Tricuspid | 160 (56.7) | 0 (0) | 77 (90.6) | 77 (92.8) |
| Bicuspid | 100 (35.5) | 96 (100) | 1 (1.2) | 2 (2.4) |
| Right/left coronary cusp fusion | 81 | 73 | 1 | 2 |
| Right/non-coronary cusp fusion | 13 | 13 | 0 | 0 |
| Left/non-coronary cusp fusion | 2 | 2 | 0 | 0 |
| Unclear | 4 | |||
| Unicuspid | 8 (2.8) | 0 (0) | 0 (0) | 0 (0) |
| Quadricuspid | 2 (0.7) | 0 (0) | 0 (0) | 1 (1.2) |
| Unclear | 12 (4.3) | 0 (0) | 7 (8.2%) | 3 (3.6) |
| LV function, | ||||
| Normal LV function | 191 (67.7) | 74 (77.1) | 56 (65.9) | 48 (57.9) |
| Borderline LV dysfunction | 25 (8.9) | 8 (8.3) | 6 (7.1) | 8 (9.6) |
| Mild LV dysfunction | 38 (13.5) | 10 (10.4) | 11 (12.9) | 15 (18.1) |
| Moderate LV dysfunction | 16 (5.7) | 2 (2.1) | 6 (7.1) | 8 (9.6) |
| Severe LV dysfunction | 10 (3.6) | 2 (2.1) | 5 (5.9) | 3 (3.6) |
| Unclear | 2 (0.7) | 0 (0) | 1 (1.1) | 1 (1.2) |
| Mechanism |
| Age | BAV | Rheum | Ao | Deg | Unsure | UAV | QAV | Marfan | CVA |
|---|---|---|---|---|---|---|---|---|---|---|---|
| IA | 30 | 66.2 | 0 | 0 | 28 | 2 | 0 | 0 | 0 | 0 | 0 |
| IB | 23 | 68.8 | 2 | 0 | 21 | 0 | 0 | 0 | 0 | 0 | 0 |
| IC | 1 | 26 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| III | 39 | 66.2 | 8 | 1 | 1 | 26 | 3 | 0 | 0 | 0 | 0 |
| IA + II | 26 | 61.3 | 15 | 0 | 3 | 7 | 0 | 1 | 0 | 0 | 0 |
| IA + III | 32 | 63.5 | 7 | 0 | 6 | 15 | 0 | 3 | 1 | 0 | 0 |
| IB + II | 45 | 51.8 | 22 | 0 | 6 | 16 | 0 | 0 | 0 | 1 | 0 |
| IB + III | 13 | 65.2 | 5 | 2 | 2 | 4 | 0 | 0 | 0 | 0 | 0 |
| IC + II | 31 | 42.8 | 20 | 0 | 0 | 9 | 0 | 1 | 0 | 0 | 1 |
| IC + III | 5 | 54.8 | 2 | 0 | 0 | 2 | 0 | 1 | 0 | 0 | 0 |
| II + III | 8 | 70.6 | 3 | 0 | 0 | 5 | 0 | 0 | 0 | 0 | 0 |
| IA + II + III | 1 | 69 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 |
| IB + II + III | 3 | 44 | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 |
| IC + II + III | 1 | 26 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 |
| Unclear | 2 | 53.5 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Aortic Disease and Treatment Approaches · Cardiovascular Function and Risk Factors
Introduction
With an estimated prevalence of ∼1–2%, AR is the third-most common valvular heart disease (VHD) following aortic stenosis and mitral regurgitation (MR). The El-Khoury system classifies AR according to leaflet motion into normal aortic valve leaflet motion (Type I, further subdivided into Ia-ascending aorta dilation, Ib-aortic root dilation, and Ic-annular dilation), excessive leaflet motion/prolapse (Type II), and restricted leaflet motion (Type III).^1^ A detailed description of the mechanism of aortic regurgitation (AR) facilitates surgical decision-making. AR mechanisms have been examined in surgical cohorts^2-4^ but rarely in the general population. We aimed to describe the mechanisms of isolated AR in an echocardiography-derived cohort of patients and examine mid-term outcomes associated with each AR type.
Methods
Study participants
All patients who underwent an echocardiography at the University of Ottawa Heart Institute between 1 January 2014 and 15 January 2019 with moderate-to-severe (3+) or severe (4+) AR were identified. Patients with other concomitant significant VHD (>mild aortic or mitral stenosis, >moderate MR), and/or prior cardiac/aorta surgery were excluded. AR secondary to infective endocarditis or aortic dissection was also excluded. All echocardiograms and the electronic medical records of included patients were reviewed to identify demographics and patient characteristics, date of last follow-up, survival, dates and type of valve surgery performed.
Echocardiographic analysis
AV anatomy, including number of cusps, raphe presence and location, and aortic dimensions was identified and measured in accordance with the American Society of Echocardiography guidelines.^5^ Cut-offs for aortic root and ascending aorta enlargement were established using the age, sex, and body surface area reference values from the most recent guidelines.^6^ The aortic annulus was considered enlarged if its diameter exceeded 25 mm.
AR aetiology was assessed based on leaflets’ anatomy, aorta dimensions and the presence of advanced degenerative features or a history of systemic illness. Aortic valve (AV) prolapse/flail leaflet was defined as a malcoaption of the tip of culprit cusp in diastole below the adjacent leaflet with an effective height of ≤ 9 mm.
Statistical analysis
Comparisons between groups were performed using the Welch’s t-test, χ^2^ test The Kruskall-Wallis test followed by Wilcoxon rank-sum tests was used to identify differences in median age based on valve anatomy. A two-sided P-value ≤0.05 was used to define statistical significance.
Results
Patient cohort and characteristics
Of the 86 358 echocardiograms performed at our centre between 1 January 2014 and 15 January 2019, 692 patients presented with moderate-to-severe or severe AR. After the exclusion of prior AV surgery, concomitant VHD and endocarditis or dissection 282 patients were identified (Figure 1). The characteristics of the study cohort are described in Table 1.
Patients with isolated moderate-to-severe (3+) or severe (4+) aortic regurgitation identified on transthoracic or transoesophageal echocardiography. AR, aortic regurgitation; Ao, aortopathy; Rheum, rheumatic; BAV, Bicuspid aortic valve; CVA, congenital valve abnormality; Deg, degenerative/other; QAV, quadricuspid aortic valve; UAV, unicuspid aortic valve; Unc, unclear.
Aetiology of AR
The most common aetiologies of AR were bicuspid aortic valve (BAV) in 96 patients (34.0%), degenerative in 85 patients (30.1%), and aortopathy in 83 patients (29.4%). Other aetiologies included unicuspid valves in patients 8 (2.8%), rheumatic AV disease in 3 (1.1%) patients, a quadricuspid valve in 1 (0.4%) patient, Marfan syndrome in 1 (0.4%) patient and malformation (0.4%) in one patient. In 4 (1.4%) patients, the aetiology was unclear.
Mechanisms of AR
A single AR mechanism was noted in 115 patients (40.8%), while 165 patients (58.5%) had multiple mechanisms. In 2 (0.7%) patients, the mechanism could not be determined (Table 2). Type II (leaflet prolapse) was the most frequently encountered mechanism seen in 137 (48.6%) of patients, followed by Type III (leaflet restriction) in 102 (36.2%) of patients. Type Ia (dilated ascending aorta) AR was seen in 89 (31.6%) patients, Type Ib (dilated aortic root) in 84 (29.8%) patients, and Type Ic (dilated aortic annulus) in 38 (13.5%) patients.
Among the 165 patients with multiple AR mechanisms, the most common combination was Type Ib and II, seen in 45 (27.3%) patients, followed by Type Ia and III in 32 (19.4%) patients. Five (3.0%) patients had three distinct mechanisms of AR. Among the 115 patients with single mechanisms of AR, Type III was the most common in 39 patients (33.9%), followed by Type Ia in 30 (26.1%) of patients, Type Ib in 23 (19.7%), and Type II in 22 (18.8%). One (0.1%) patient had isolated Type Ic AR. One hundred (35.5%) of patients had a BAV. The presence of Type II AR (72% vs. 28%, P < 0.001), as well as AR due to multiple mechanisms (77% vs. 48%, P < 0.001), was more common in patients with than without BAV.
Severity of AR
Patients with Type II AR were more likely to have severe (4+) AR than those without (50.3% vs. 25.6%, P < 0.001), whereas patients with leaflet restriction were less likely to have severe (4+) AR than those without (18.6% vs. 48.3%, P < 0.01). No significant differences in severity of AR were found between aetiology of AR, number of cusps, or number of mechanisms of AR.
Interventions and mortality
During a median follow-up of 4.7 years, IQR (3.0–6.6) [available in 275 (97.5%) patients], 19 patients (6.9%) died, and 158 patients (57.5%) underwent AV surgery, which comprised 77 (48.7%) AV repair or valve-sparing aortic root replacement, and 80 (50.6%) patients AV replacement [mostly (82.5%) bioprosthetic valve]. One patient with severe AR and mild stenosis underwent a transcatheter aortic valve implantation. Rates of any intervention were similar between patients with and without BAV (58.0% vs. 57.1%, P = 0.89) that persisted after adjustment for age, sex and AR severity.
The rate of valve repair/valve-sparing aortic root repair varied with AR type and was higher in Type I AR compared with other types (56% vs. 21%, P < 0.001). For patients with Type II AR, the rate was similar to those other types (54% vs. 41%, P = 0.1), while the rate was lower in Type III compared with other types (19% vs. 60%, P < 0.001). The rate of valve repair was similar among patients with and without BAV (51.7 vs. 48.3%, P = 0.6).
Discussion
This study reports mechanisms of isolated AR using the El-Khoury classification in a non-surgical cohort. Surgical cohorts of patients with isolated AR have previously described the mechanism of AR but are highly selected.^2-4^ Compared with prior surgical reports, our patient population was older, which was likely driven by the inclusion of patients who were either non-surgical candidates or in whom the risk-benefit ratio favoured a conservative approach. Presence of a BAV was common (34–44%) in our and prior studies, reflecting the relatively high frequency of this abnormality as an aetiology for AR. As in our study, prolapse was found to be the most common AR mechanism in surgical studies that specifically reported on this finding. The presence of multiple mechanisms was somewhat higher in our study. This difference may be driven by our older population with an associated higher rate of degenerative leaflet disease complicating root or ascending aorta dilatation. Our study also found that the most common mechanistic combination type was root dilatation and prolapse.
Surgical intervention and outcomes
Over a 4.7-year period, over half of the included patients underwent a surgical intervention, of which close to half were an AV repair/annuloplasty. This high rate of valve-sparing repair reflects growing recognition of the feasibility, and favourable outcomes in selected patients, as well as our local expertise. Despite the increasing volume of AV repair reported in the literature, the general current rates are not well described and are centre and operator dependent.
Limitations
Our study has several limitations, including (i) being a single-centre retrospective design, (ii) enrolment based on index echocardiogram which included both transthoracic echocardiogram or transesophageal echocardiogram, (iii) exclusion of patients with AV endocarditis (which explains why we did not identify patients with Type Id AR), (iv) AV repair is only performed by highly experienced surgeons at our site and our results may not be applicable to all centres or regions, and (v) patients deemed not to be surgical patients were not identified in the data review process. In addition to echocardiography, cross-sectional imaging such as CT and MRI are frequently used in further determining the presence of aortic root and ascending aorta dilatation. The potentially complementary role of these advanced cardiac imaging techniques for the classification of the mechanism of severity of AR was also not assessed in this study.
Conclusion
We report AR aetiologies and mechanisms in a consecutive cohort of patients with isolated AR identified through echocardiography at a quaternary cardiac care centre. Leaflet prolapse was the most common AR mechanism, followed by leaflet restriction. Most patients had multiple mechanisms, especially those with BAV, who represented one-third of the population. The most common combinations were aortic root dilatation and leaflet prolapse, followed by leaflet restriction and ascending aorta dilatation. AV repair was performed in about half of all patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1El Khoury G, Glineur D, Rubay J, Verhelst R, d'Acoz Y, Poncelet A, Astarci P, Noirhomme P, van Dyck M. Functional classification of aortic root/valve abnormalities and their correlation with etiologies and surgical procedures. Curr Opin Cardiol 2005;20:115–121.15711197 10.1097/01.hco.0000153951.31887.a 6 · doi ↗ · pubmed ↗
- 2Lansac E, Di Centa I, Raoux F, Al Attar N, Acar C, Joudinaud T, Raffoul R. A lesional classification to standardize surgical management of aortic insufficiency towards valve repair. Eur J Cardiothorac Surg 2008;33:872–878; discussion 8–80.18258445 10.1016/j.ejcts.2007.12.033 · doi ↗ · pubmed ↗
- 3Boodhwani M, de Kerchove L, Glineur D, Poncelet A, Rubay J, Astarci P, Verhelst R, Noirhomme P, El Khoury G. Repair-oriented classification of aortic insufficiency: impact on surgical techniques and clinical outcomes. J Thorac Cardiovasc Surg 2009;137:286–294.19185138 10.1016/j.jtcvs.2008.08.054 · doi ↗ · pubmed ↗
- 4Yang LT, Michelena HI, Maleszewski JJ, Schaff HV, Pellikka PA. Contemporary etiologies, mechanisms, and surgical approaches in pure native aortic regurgitation. Mayo Clin Proc 2019;94:1158–1170.31272566 10.1016/j.mayocp.2018.11.034 · doi ↗ · pubmed ↗
- 5Zoghbi WA, Adams D, Bonow RO, Enriquez-Sarano M, Foster E, Grayburn PA, Hahn RT, Han Y, Hung J, Lang RM, Little SH, Shah DJ, Shernan S, Thavendiranathan P, Thomas JD, Weissman NJ. Recommendations for noninvasive evaluation of native valvular regurgitation: a report from the American society of echocardiography developed in collaboration with the society for cardiovascular magnetic resonance. J Am Soc Echocardiogr 2017;30:303–371.28314623 10.1016/j.echo.2017.01.007 · doi ↗ · pubmed ↗
- 6Goldstein SA, Evangelista A, Abbara S, Arai A, Asch FM, Badano LP, Bolen MA, Connolly HM, Cuéllar-Calàbria H, Czerny M, Devereux RB, Erbel RA, Fattori R, Isselbacher EM, Lindsay JM, Mc Culloch M, Michelena HI, Nienaber CA, Oh JK, Pepi M, Taylor AJ, Weinsaft JW, Zamorano JL, Dietz H, Eagle K, Elefteriades J, Jondeau G, Rousseau H, Schepens M. Multimodality imaging of diseases of the thoracic aorta in adults: from the American society of echocardiography and the Europea · doi ↗ · pubmed ↗