Infectious Diarrhea in Kidney Transplant Recipients
Yassin Loucif, Collin Mackenzie, Olga Tselikmann, Lars C Rump

TL;DR
This study examines infectious diarrhea in kidney transplant patients, identifying common pathogens and the impact of immunosuppression.
Contribution
The study characterizes the specific pathogen spectrum and risk factors for infectious diarrhea in a German kidney transplant cohort.
Findings
Clostridioides difficile was the most common pathogen (26.3%) in kidney transplant recipients.
CMV-related diarrhea occurred exclusively in transplant patients and recurred frequently.
Immunosuppression significantly increased susceptibility to infections like C. difficile and CMV.
Abstract
Introduction Infectious diarrhea represents a significant and frequent complication among kidney transplant recipients, primarily due to the immunosuppressive therapy required to prevent graft rejection. This condition poses substantial risks to both graft function and patient survival, driven by increased susceptibility to opportunistic pathogens and potential medication-related gastrointestinal effects. This study aims to characterize the pathogen spectrum and associated risk factors of infectious diarrhea in a German cohort of kidney transplant recipients, providing insights into regional patterns and clinical implications. Methods A retrospective cohort study was conducted, analyzing 604 patients, including 436 kidney transplant recipients, who were hospitalized with infectious diarrhea (ICD-10 codes A00-A09) at the Universitätsklinikum Düsseldorf (UKD) between January 2019 and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
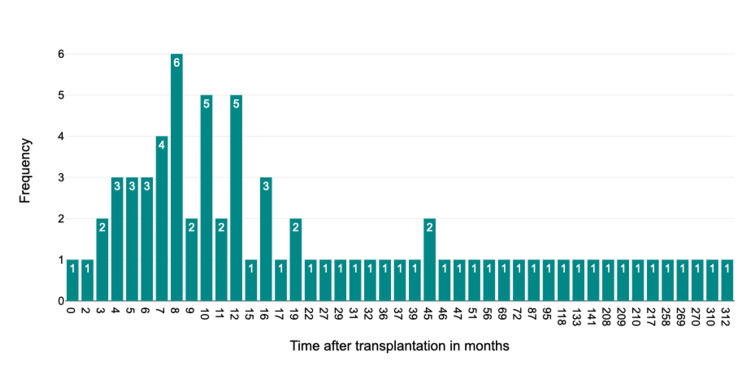 Figure 1
Figure 1| Pathogen | Absolute frequency (N) | Relative frequency (%) |
| Clostridioides difficile | 96 | 34.78 |
| Cytomegalovirus | 74 | 26.81 |
| Enteropathogenic | 40 | 14.49 |
| Norovirus | 28 | 10.14 |
| Campylobacter jejuni | 7 | 2.54 |
| EAEC | 6 | 2.17 |
| Adenovirus | 6 | 2.17 |
| EHEC | 5 | 1.81 |
| Rotavirus | 5 | 1.81 |
| Astrovirus | 3 | 1.09 |
| Yersinia enteroclitica | 2 | 0.72 |
| Microsporidien | 1 | 0.36 |
| Kryptosporidien | 1 | 0.36 |
| Salmonella spp. B | 1 | 0.36 |
| Salmonella typhimurium | 1 | 0.36 |
| Total | 276 | 100.0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClostridium difficile and Clostridium perfringens research · Mycobacterium research and diagnosis · Viral gastroenteritis research and epidemiology
Introduction
In Germany, more than 2,000 kidney transplants are performed annually, and over 10,000 patients remain on the national transplant waiting list [1]. Kidney transplant recipients are at increased risk for infectious complications due to long-term immunosuppressive therapy, with estimates suggesting that up to 70% of all transplant recipients experience at least one infectious complication within the first three years after transplantation [2]. Gastrointestinal symptoms, particularly diarrhea, are among the most frequent clinical issues in this population. The pathogen spectrum of infectious diarrhea can vary substantially depending on regional epidemiology, immunosuppressive regimens, and individual patient characteristics. Data from India suggest a wide variety of microbial agents, including bacteria, viruses, and parasites [3]. However, there is a significant lack of data on the specific microbial pathogens that lead to hospitalization in kidney transplant recipients within Central Europe.
The aim of this study is to systematically identify and characterize the pathogens associated with both acute and chronic forms of infectious diarrhea in hospitalized kidney transplant recipients. In addition, we assessed patient-specific clinical parameters to determine potential risk factors and relevant clinical associations. A further focus was placed on differentiating infectious from drug-induced toxic diarrhea, which remains a common diagnostic challenge in transplant medicine.
Identifying the most relevant pathogens in this vulnerable patient group may help reduce diagnostic delays between symptom onset and microbiological confirmation. In the long term, this could support the implementation of efficient, targeted, and resource-conscious diagnostic strategies. This study contributes to closing an important research gap and to improving both clinical care and the cost-effectiveness of patient management.
Materials and methods
Study design
This retrospective cohort study was performed at the Universitätsklinikum Düsseldorf (UKD), Nephrology Department. Patients hospitalized from January 1, 2019, to December 31, 2023, with an infectious diarrhea diagnosis (ICD-10 A00-A09) were included if clinical records were complete. Data were sourced from the GCM Medico hospital information system.
Patient cohort
The cohort comprised 604 hospitalized patients, including 436 kidney transplant recipients (436/604; 72.2%). In addition to kidney transplant recipients, a smaller group of nontransplanted patients with infectious diarrhea was included for comparative purposes of the pathogen spectrum. Collected variables included transplantation status, transplantation date, admission date, identified pathogens, recurrence status, immunosuppression regimens, and demographics (age, gender). Patients with incomplete records were excluded.
Microbiological analysis
Pathogen detection was conducted at UKD’s Institute of Microbiology and Virology. Stool samples underwent DNA extraction with the Qiagen EZ1 DNA Tissue Kit, followed by real-time polymerase chain reaction (PCR) using fluorescence-labeled probes targeting Clostridioides difficile toxin genes, cytomegalovirus (CMV) DNA, enteropathogenic* Escherichia coli* (EPEC) intimin gene (eae), and norovirus RNA.
Statistical analysis
Data were processed using Apple Numbers and analyzed with the DATAtab software. Fisher’s exact test was used to compare pathogen frequencies between transplant and nontransplant groups, the Kruskal-Wallis Test was used to assess seasonal clustering, and Mood’s median test was used to evaluate time from transplantation to infection.
Statistical significance was defined as p < 0.05. Numerical values are presented as N, %, or mean ± standard deviation (SD), as indicated. Where applicable, test statistics (e.g., χ²-value, t-value, F-value) are provided alongside the corresponding p-value in tables. Decimal separators were standardized using periods (e.g., 1.25).
Results
Among 436 transplant recipients, a pathogen was detected in 276 cases. The identified pathogens are presented in Table 1.
Impact of immunosuppression
Standard immunosuppressive therapy consisted of a combination of calcineurin inhibitors (cyclosporine or tacrolimus) or mTOR inhibitors (sirolimus), mycophenolate mofetil, and corticosteroids (triple therapy). In total, n = 374 patients (85.98%) received triple therapy. Dual immunosuppressive therapy (either a calcineurin inhibitor or mTOR inhibitor combined with corticosteroids) was documented in n = 52 cases (11.95%). Monotherapy with corticosteroids alone was observed in n = 9 patients (2.07%).
Immunosuppressive therapy was significantly associated with an increased risk of infection. Patients receiving immunosuppressive therapy showed a significantly higher incidence of Clostridioides difficile infections compared to non-immunosuppressed patients (Fisher’s exact test, test statistic = 0.208, p = 4.08 × 10^-^⁹). CMV was exclusively detected in kidney transplant recipients (test statistic = ∞, p = 1.45 × 10^-^¹¹).
Temporal patterns
CMV infections occurred at a median of 13.5 months post-transplantation, coinciding with the end of standard antiviral prophylaxis. This was significantly earlier than the median for all other pathogens (Mood’s median test, test statistic = 9.63, p = 0.0019). *Clostridioides difficile *infections also occurred significantly earlier, with a median of 15.5 months post-transplantation (Mood’s median test, test statistic = 6.54, p = 0.0106). Other pathogens showed no significant temporal clustering (Figure 1).
Time-dependent occurrence of cytomegalovirus-associated infectious diarrhea following kidney transplantation CMV: cytomegalovirusHistogram of CMV-positive diarrhea cases (N = 74) by months after kidney transplantation. A statistically significant clustering was observed at 13 months post-transplantation (Mood’s median test, test statistic = 9.63, p = 0.0019)
Seasonal variation
No statistically significant seasonal variation in pathogen detection was observed across calendar months (Kruskal-Wallis test, test statistic = 11.00, p = 0.443). This indicates a uniform distribution of infectious diarrhea cases throughout the year, with no evidence of temporal clustering.
Discussion
Key findings
This single-center study conducted at the University Hospital of Düsseldorf identified Clostridioides difficile, CMV, EPEC, and norovirus as the predominant pathogens causing infectious diarrhea in kidney transplant recipients. Immunosuppressive therapy significantly increased both infection and recurrence risk, with CMV being exclusively detected among transplant recipients (Fisher’s exact test, test statistic = ∞, p < 0.001). The absence of seasonal variation (Kruskal-Wallis test, test statistic = 11.00, p = 0.443) suggests that immunosuppression may be a more relevant risk factor than environmental exposure.
Literature context
These findings are consistent with prior studies reporting EPEC and norovirus as frequent pathogens in kidney transplant recipients [4] and confirming Clostridioides difficile as a major cause of infectious diarrhea in this population [5]. Interestingly, the peak incidence of CMV infections at approximately 13 months post-transplant contrasts with earlier studies describing peaks within 30 to 90 days post-transplantation [6]. Parasitic infections, commonly reported in other studies [7], were rarely detected in this cohort, potentially due to regional differences, improved hygiene standards, or the specific diagnostic PCR panel used.
Clinical implications
Multiplex PCR proved effective in identifying causative pathogens and is recommended as a standard diagnostic tool in immunocompromised patients [4]. Enhanced screening for CMV and Clostridioides difficile is particularly warranted following the cessation of prophylaxis, especially within the first two years post-transplantation. Implementing rigorous antibiotic stewardship and infection control protocols may help reduce the recurrence of Clostridioides difficile-associated diarrhea [8]. Given that persistent diarrhea is associated with an increased risk of graft dysfunction, careful adjustment of immunosuppressive regimens, particularly involving agents such as mycophenolate mofetil, should be considered [9].
Limitations
As a retrospective single-center study, this analysis is subject to several limitations. Selection and information bias cannot be fully excluded. Patients without sufficient clinical or microbiological documentation, such as missing discharge summaries or absent pathogen testing, were not included in the final analysis; however, the exact number of excluded cases was not recorded. There is no specific International Classification of Diseases (ICD) coding for all diarrheal episodes, and microbiological testing was not performed systematically in all cases, but rather based on clinical judgment at the time of presentation. Therefore, it is not possible to determine how many patients may have experienced diarrhea without undergoing microbiological testing. Data on prior antibiotic use, duration of diarrhea, recent travel history, and temporal changes in immunosuppressive therapy were not extracted and could not be analyzed due to inconsistent or incomplete documentation in the medical records. Likewise, we did not evaluate comorbidities such as cardiovascular or metabolic conditions, as they were not part of the study’s predefined focus. Medications known to predispose to diarrhea or *Clostridioides difficile *infection, such as proton pump inhibitors or mycophenolate mofetil, were not systematically assessed. These aspects may warrant further investigation in future prospective studies with standardized data collection.
Future directions
Prospective studies are needed to better assess the impact of extended antiviral prophylaxis and to explore the utility of microbiota-based therapeutic approaches [10]. Multicenter trials may help identify regional pathogen patterns and validate the findings of this study across diverse transplant populations.
Conclusions
Infectious diarrhea remains a significant complication among kidney transplant recipients, primarily due to the effects of immunosuppressive therapy. This study identified Clostridioides difficile, CMV, EPEC, and norovirus as the most frequently detected pathogens. The findings emphasize the importance of targeted diagnostic approaches and the timely identification of high-risk patients. Advanced diagnostic tools such as multiplex PCR, alongside individualized preventive and therapeutic strategies, are essential to preserve graft function and improve long-term patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Deutsche stiftung organtransplantation (DSO), jahresbericht 2023, S. 862023 https://www.dso.de/Site Collection Documents/DSO-Jahresbericht%202023.pdf
- 2Diarrhea in kidney transplant recipients: etiology and outcome Indian J Gastroenterol Sonambekar A Mehta V Desai D 1411463920203235072410.1007/s 12664-020-01022-1 · doi ↗ · pubmed ↗
- 3Infection in Kidney Transplantation Contemporary kidney transplantation Nambiar P Silibovsky R Belden KA 3073272018
- 4Microbiological diagnosis of severe diarrhea in kidney transplant recipients by use of multiplex PCR assays J Clin Microbiol Coste JF Vuiblet V Moustapha B 184118495120132355420510.1128/JCM.03366-12PMC 3716061 · doi ↗ · pubmed ↗
- 5Diarrhea after kidney transplantation: a study of risk factors and outcomes J Postgrad Med Patil AD Saxena NG Thakare SB Pajai AE Bajpai D Jamale TE 2052146920233767566710.4103/jpgm.jpgm_601_22PMC 10846809 · doi ↗ · pubmed ↗
- 6The efficacy and safety of 200 days valganciclovir cytomegalovirus prophylaxis in high-risk kidney transplant recipients Am J Transplant Humar A Lebranchu Y Vincenti F 122812371020102035346910.1111/j.1600-6143.2010.03074.x · doi ↗ · pubmed ↗
- 7Parasitic infection in renal transplant recipients Transplant Proc Valar C Keitel E Dal PráRL 4604623920071736275910.1016/j.transproceed.2007.01.025 · doi ↗ · pubmed ↗
- 8Clinical practice guideline by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA): 2021 focused update guidelines on management of Clostridioides difficile infection in adults Clin Infect Dis Johnson S Lavergne V Skinner AM Gonzales-Luna AJ Garey KW Kelly CP Wilcox MH 04473202110.1093/cid/ciab 54934164674 · doi ↗ · pubmed ↗