Primary Cutaneous CD4+ Small/Medium T-cell Lymphoproliferative Disorder in a Young Japanese Male Patient
Yuta Norimatsu, Mina Komuta, Yuichiro Hayashi, Kennosuke Karube, Makoto Sugaya

TL;DR
A young Japanese man was diagnosed with a rare skin lymphoproliferative disorder after initial misdiagnosis and treatment failure.
Contribution
This case report highlights the possibility of misdiagnosing young patients with PCSM-LPD as pseudolymphoma.
Findings
The patient's skin biopsy showed CD4+ T-cell dominance and clonal T-cell expansion.
The lesion resolved after treatment with fludroxycortide tape.
NFATc1 staining was negative, supporting the diagnosis of PCSM-LPD over pseudolymphoma.
Abstract
A 34-year-old man became aware of an erythematous nodule on the left nasal wing. He was treated with topical steroids and oral antibacterial agents at his local doctor, but his condition did not improve, and he was referred to our hospital. A skin biopsy revealed diffuse cellular infiltration through the dermis. No epidermotropism was seen. The major infiltrate was small to medium-sized lymphoid cells. The number of CD3+ cells was almost the same as that of CD20+ cells, while CD4+ cells were dominant over CD8+ cells. Atypical lymphocytes were positive for BCL6 and PD-1. Polymerase chain reaction (PCR) analysis of immunoglobulin heavy chain and T-cell receptor gene rearrangements on paraffin-embedded tissue sections revealed a clonal expansion of T-cells. The patient was diagnosed as having primary cutaneous CD4+ small/medium T-cell lymphoproliferative disorder (PCSM-LPD) and treated…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1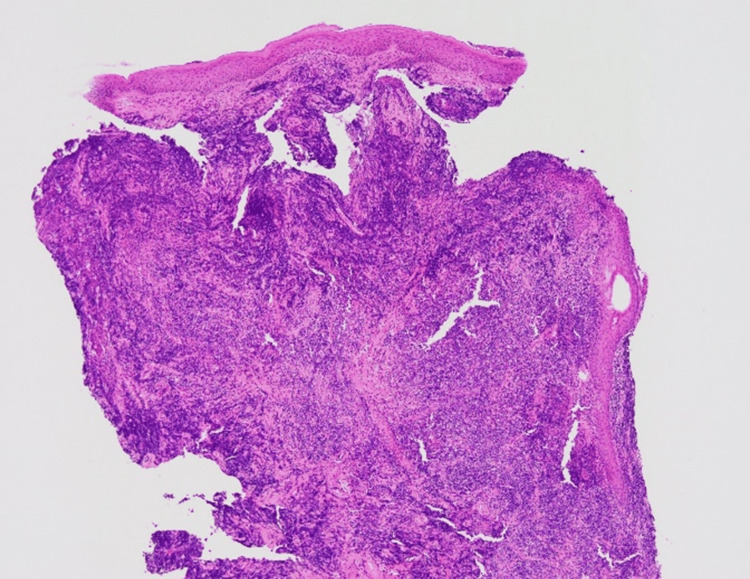 Figure 2
Figure 2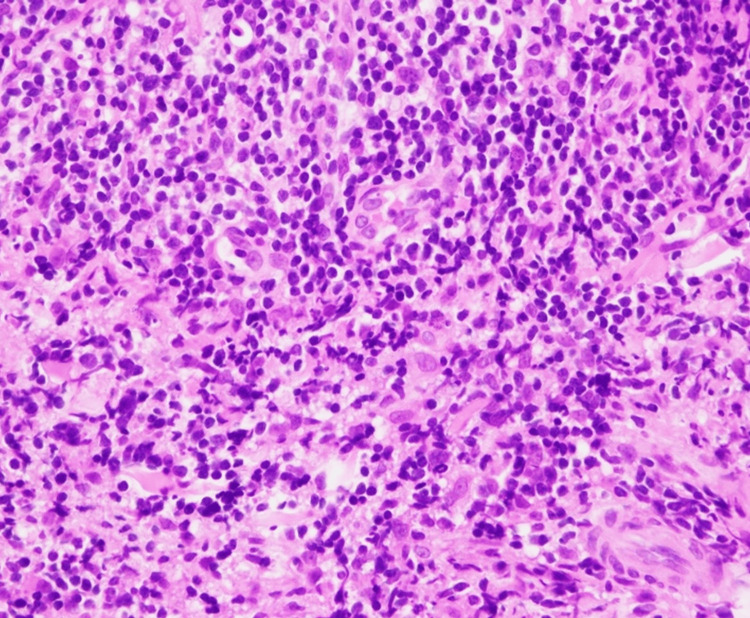 Figure 3
Figure 3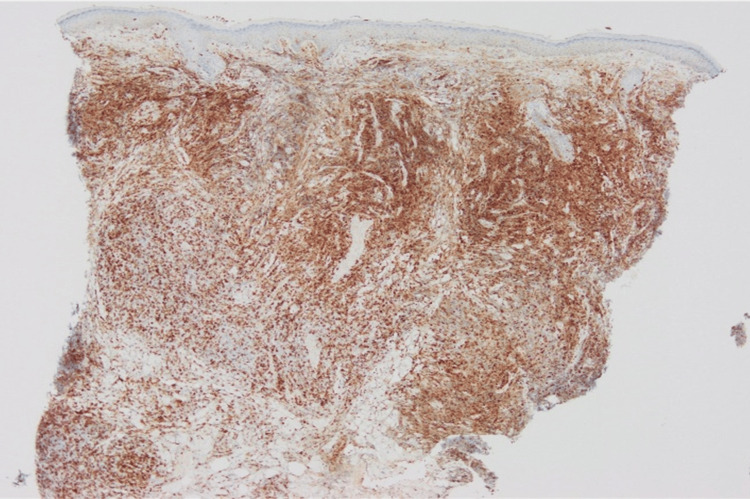 Figure 4
Figure 4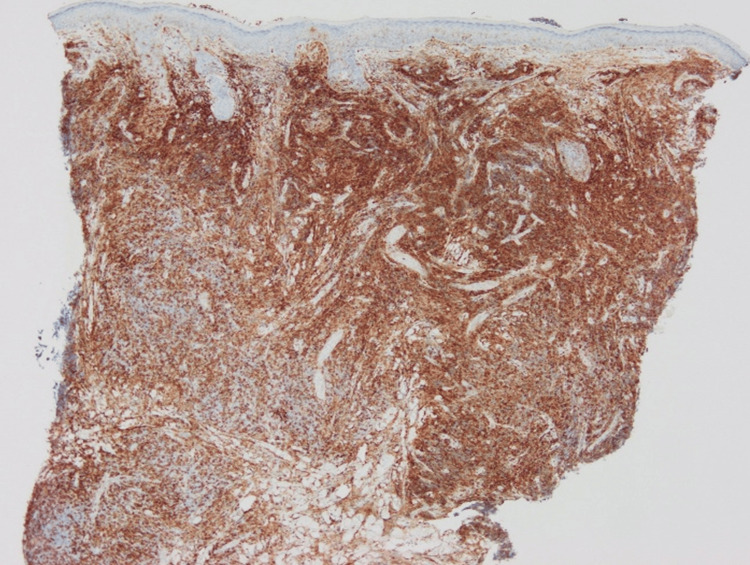 Figure 5
Figure 5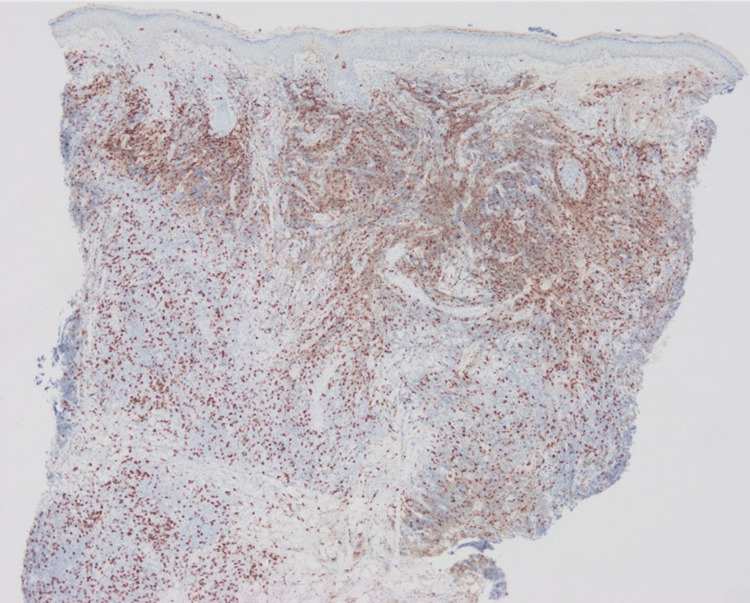 Figure 6
Figure 6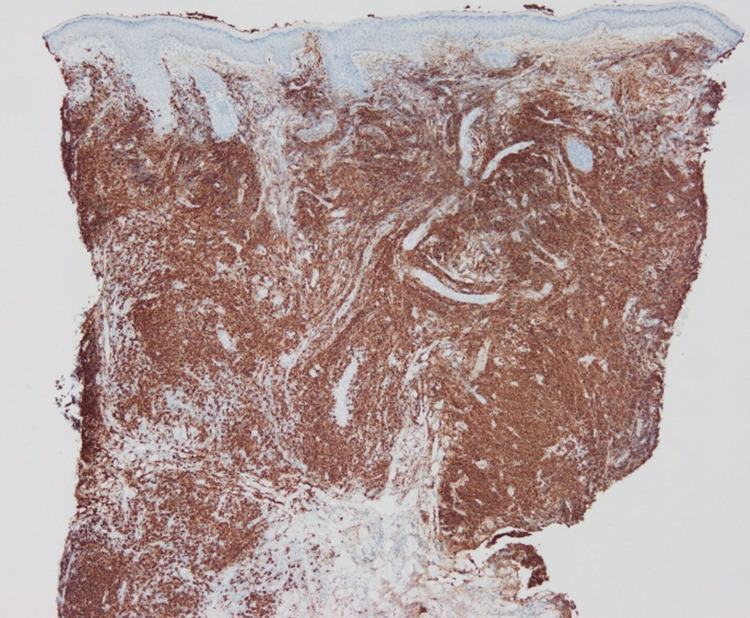 Figure 7
Figure 7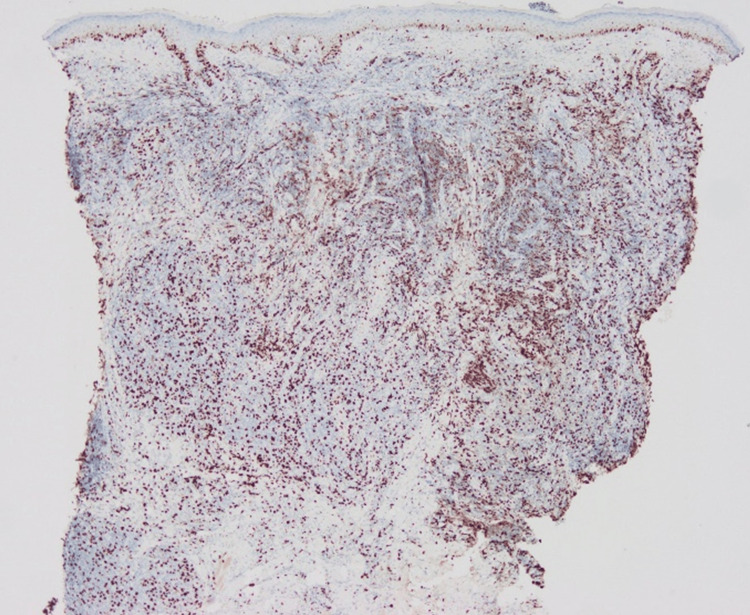 Figure 8
Figure 8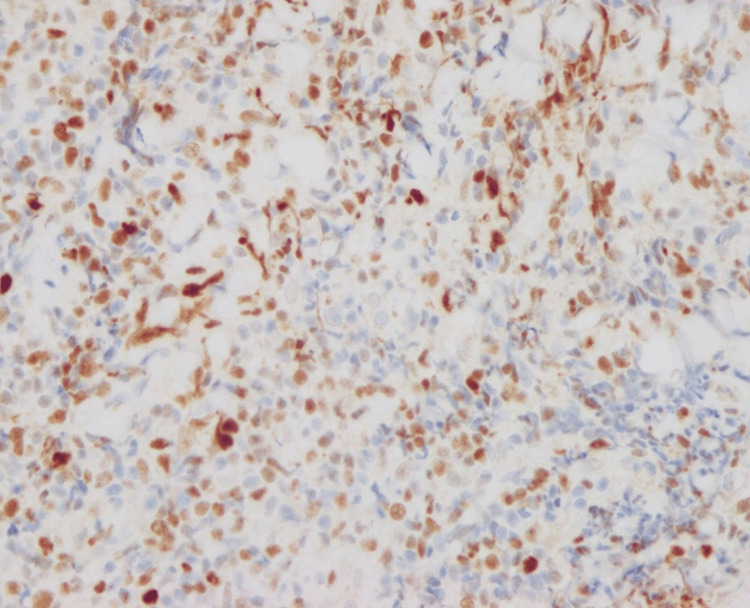 Figure 9
Figure 9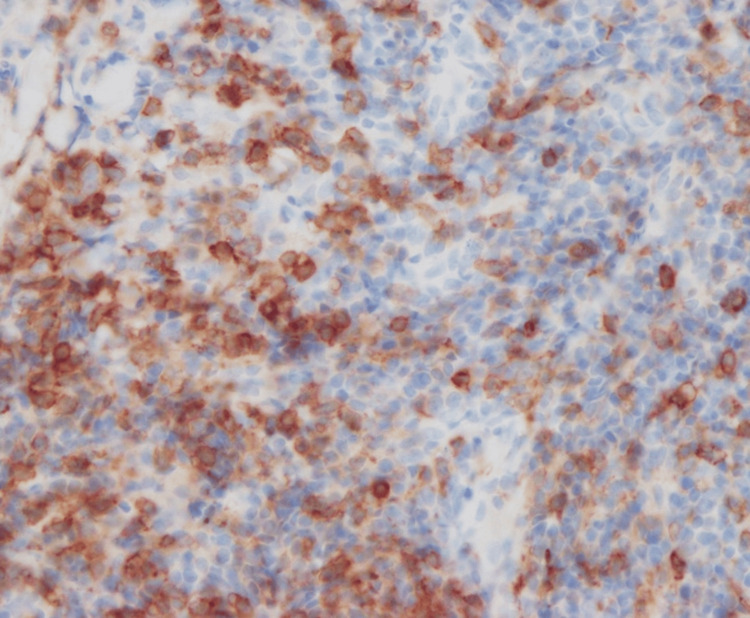 Figure 10
Figure 10 Figure 11
Figure 11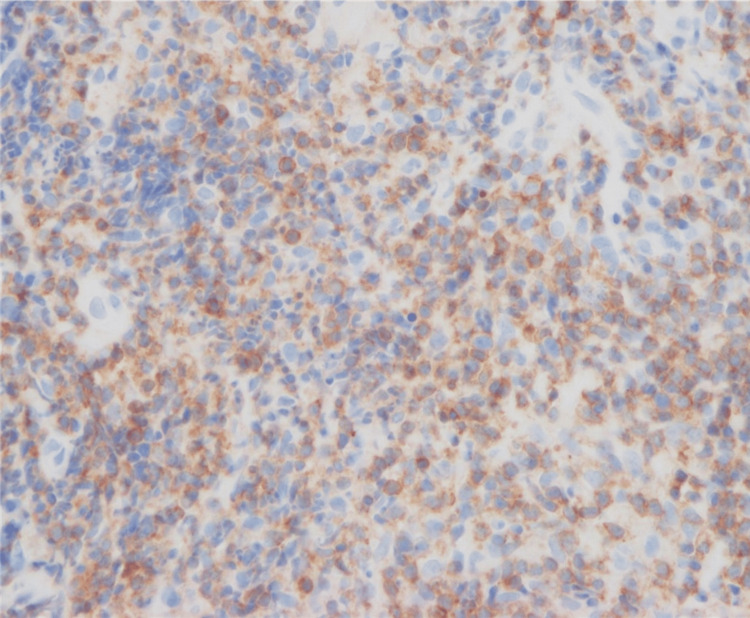 Figure 12
Figure 12Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous lymphoproliferative disorders research · Fungal Infections and Studies · CNS Lymphoma Diagnosis and Treatment
Introduction
Primary cutaneous CD4+ small/medium T-cell lymphoproliferative disorder (PCSM-LPD) is synonymous with what used to be called primary cutaneous CD4-positive small- and medium-sized T-cell lymphoma, which has recently been renamed [1]. PCSM-LPD is characterized by nodules or plaques on the face, neck, and upper body [1]. Histology shows nodular or diffuse infiltration of CD4+ small to medium-sized T cells. The tumor cells are positive for follicular helper T-cell markers such as PD-1, BCL6, and CXCL13. The proliferation rate assessed by Ki-67 positivity is low, ranging from less than 5% to a maximum of 20% [1-5]. The male-to-female ratio of PCSM-LPD European patients was 1:1, and 91% of patients were said to be rash-free and mildly relieved within a median of 63 months. The median age of the disease onset in Europe is 53 years. The remaining 9% of patients survive with residual skin symptoms. PCSM-LPD often resolves spontaneously after skin biopsy but may be treated with topical steroids, surgery, or radiation therapy [6]. In the Japanese report, the male-to-female ratio of PCSM-LPD was 11:14 [7]. The median age was 61.5 years, older than that of Europeans. It was relatively rare, occurring in 25 (1.4%) of 1733 patients with cutaneous lymphoma diagnosed between 2007 and 2011 [7]. Here, we report a young patient with PCSM-LPD, who was successfully treated with occlusive topical steroid.
Case presentation
A 34-year-old man was referred to our hospital with a suspicion of cutaneous lymphoma. The patient noticed a red nodule on the left nasal wing two months before. He visited his local doctor due to its gradual increase in size. He was treated with faropenem, topical bacitracin/fradiomycin sulfate, topical ketoconazole, and topical hydrocortisone butyrate, which were all ineffective. The nodule decreased in size while the patient took oral betamethasone, but it flared up when he stopped the drug. When the patient visited us, an erythematous nodule without ulceration was located on the left nasal wing (Figure 1).
Red nodule on the left wing of the nose at the first visit.
The skin biopsy specimen showed diffuse cellular infiltration through the dermis (Figure 2).
Hematoxylin and eosin stain shows significant cellular infiltration of the dermis (x40).
No epidermotropism was seen. The major infiltrate was small to medium-sized lymphoid cells (Figure 3).
Cells infiltrating the dermis in hematoxylin and eosin stain are small to medium-sized lymphoid cells (x400).
The number of CD3+ cells was almost the same as that of CD20+ cells, while CD4+ cells were dominant over CD8+ cells (Figures 4-7).
Immunohistological staining for CD3.
Immunohistological staining for CD4.
Immunohistological staining for CD8.
Immunohistological staining for CD20.
The ratio of Ki-67+ cells was about 20% (Figure 8).
Immunohistological staining for Ki-67.
Atypical lymphocytes were positive for BCL6 and PD-1 (Figures 9, 10).
Immunohistological staining for BCL6.
Immunohistological staining for PD-1.
Polymerase chain reaction (PCR) analysis of immunoglobulin heavy chain and T-cell receptor gene rearrangements on paraffin-embedded tissue sections revealed a clonal expansion of T-cells. CT scanning showed no extracutaneous lesions. The patient was diagnosed as PCSM-LPD and treated with fludroxycortide tape. The red nodule completely disappeared after three months (Figure 11).
Red nodule on left wing of nose completely disappeared after three months.
Discussion
A solitary red nodule on the nose with histologically dense lymphocytic infiltration is commonly seen. The diagnosis may be either cutaneous pseudolymphoma (CPL), lymphocytoma cutis, lymphadenosis benigna cutis, or cutaneous lymphoid hyperplasia, all of which refer to the same benign process mimicking lymphoma. CPL may occur at any age. It is not always easy to distinguish between CPL and PCSM-LPD. The latter is a better fit for our case because of the very high CD4+/CD8+ ratio, positivity of follicular helper T-cell makers, and clonal T-cell proliferation. Nuclear staining for nuclear factor of activated T-cells c1 (NFATc1) was reported to be a key finding of PCSM-LPD [8]. We performed additional staining for NFATc1. Unlike a previous study [8], NFATc1 was negative (Figure 12).
Nuclear staining for nuclear factor of activated T-cells c1 (NFATc1) in this case.In a previous study [8], the cytoplasm was stained; however, in the present case (as shown in the image), the cytoplasm is not stained.
A case report of PCSM-LPD in a 33-year-old woman was reported as a young case of PCSM-LPD from Japan [9]. However, this report is considered atypical for PCSM-LPD because of the high Ki-67 (40%) and negative T cell receptor gene rearrangements [9]. Another case report from Japan is that of a 52-year-old patient [10]. He was diagnosed as PCSM-LPD, but his CD30-positive status and aggressive course also made this case atypical for PCSM-LPD [10].
Conclusions
We experienced a young Japanese case of PCSM-LPD. This case was considered typical for PCSM-LPD, except for the fact that the patient was young. Our case suggested that young cases with PCSM-LPD may have been misdiagnosed with CPL, which may be one of the reasons why this type of lymphoproliferative disorder has been reported to occur in elderly people.
In addition, NFATc1 was not stained by either PCSM-LPD or CPL. Further investigation may be needed to determine if NFATc1 can be used to differentiate PCSM-LPD from CPL.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas Blood Willemze R Cerroni L Kempf W Berti E Facchetti F Swerdlow SH Jaffe ES 1703171413320193063528710.1182/blood-2018-11-881268 PMC 6473500 · doi ↗ · pubmed ↗
- 2Primary cutaneous T-cell lymphomas other than mycosis fungoides and Sézary syndrome. Part I: clinical and histologic features and diagnosis J Am Acad Dermatol Stoll JR Willner J Oh Y 107310908520213394009810.1016/j.jaad.2021.04.080 · doi ↗ · pubmed ↗
- 3Primary cutaneous CD 4+ small/medium-sized pleomorphic T-cell lymphoma expresses follicular T-cell markers Am J Surg Pathol Rodríguez Pinilla SM Roncador G Rodríguez-Peralto JL 81903320091898754110.1097/PAS.0b 013e 31818 e 52fe · doi ↗ · pubmed ↗
- 4Epstein-Barr virus negative clonal plasma cell proliferations and lymphomas in peripheral T-cell lymphomas: a phenomenon with distinctive clinicopathologic features Am J Surg Pathol BalaguéO Martínez A Colomo L 131013223120071772118510.1097/PAS.0b 013e 3180339 f 18 · doi ↗ · pubmed ↗
- 5Expression of programmed death-1 in primary cutaneous CD 4-positive small/medium-sized pleomorphic T-cell lymphoma, cutaneous pseudo-T-cell lymphoma, and other types of cutaneous T-cell lymphoma Am J Surg Pathol Cetinözman F Jansen PM Willemze R 1091163620122198934910.1097/PAS.0b 013e 318230 df 87 · doi ↗ · pubmed ↗
- 6Primary cutaneous CD 4+ small-/medium-sized pleomorphic T-cell lymphoma: a cutaneous nodular proliferation of pleomorphic T lymphocytes of undetermined significance? A study of 136 cases Am J Dermatopathol Beltraminelli H Leinweber B Kerl H Cerroni L 3173223120091946123410.1097/DAD.0b 013e 31819 f 19bb · doi ↗ · pubmed ↗
- 7Cutaneous lymphoma in Japan, 2012-2017: a nationwide study J Dermatol Sci Fujii K Hamada T Shimauchi T Asai J Fujisawa Y Ihn H Katoh N 1871939720203203386910.1016/j.jdermsci.2020.01.010 · doi ↗ · pubmed ↗
- 8Differential NFA Tc 1 expression in primary cutaneous CD 4+ small/medium-sized pleomorphic T-cell lymphoma and other forms of cutaneous T-cell lymphoma and pseudolymphoma Am J Dermatopathol Magro CM Momtahen S 951033920172709734210.1097/DAD.0000000000000597 · doi ↗ · pubmed ↗