A cross-sectional study on the relationship between dietary magnesium intake and periodontitis in different body mass index and waist circumference groups: National Health and Nutrition Examination Survey, 2009–2014
Huijie Huang, Shiyan Chen, Li Cong, Yingjuan Zeng

TL;DR
This study found that higher magnesium intake is linked to lower periodontitis risk, but only in non-obese populations.
Contribution
The study reveals that magnesium's protective effect on periodontitis is significant only in non-obese groups.
Findings
Higher magnesium intake was associated with a 28% lower odds of periodontitis in non-obese individuals.
The protective effect of magnesium was not observed in general or abdominal obese populations.
Subgroup analysis showed magnesium's benefit is limited to non-general and non-abdominal obese groups.
Abstract
This cross-sectional study aimed to investigate the correlation between magnesium consumption and periodontitis in different body mass index (BMI) and waist circumference (WC) groups. 8385 adults who participated in the National Health and Nutrition Examination Survey during 2009–2014 were included. The correlation between dietary magnesium intake and periodontitis was first tested for statistical significance by descriptive statistics and weighted binary logistic regression. Subgroup analysis and interaction tests were performed to investigate whether the association was stable in different BMI and WC groups. There was a statistical difference in magnesium intake between periodontitis and non-periodontitis populations. In model 3, participants with the highest magnesium consumption had an odds ratio of 0.72 (0.57-0.92) for periodontitis compared to those with the lowest magnesium…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
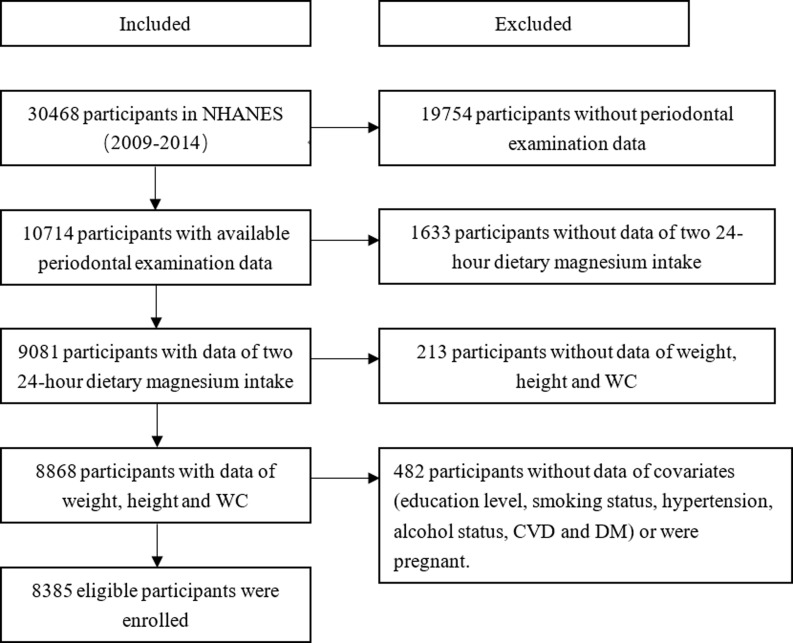 Figure 1
Figure 1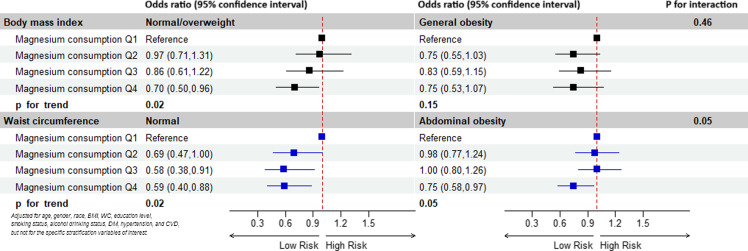 Figure 2
Figure 2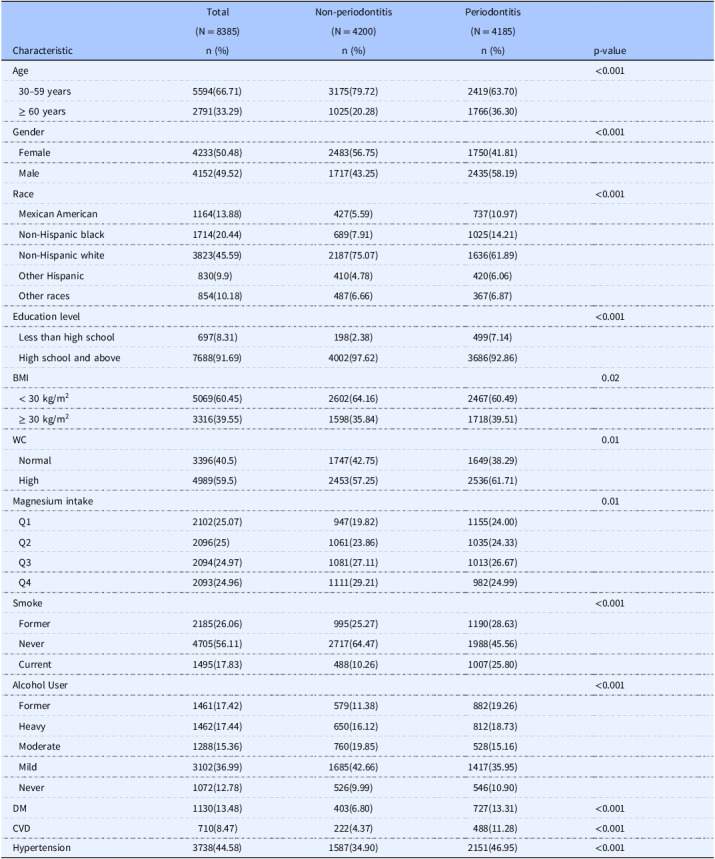 Figure 3
Figure 3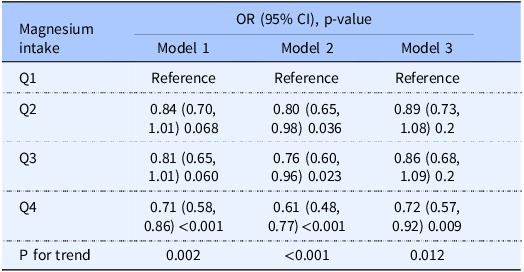 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMagnesium in Health and Disease
Introduction
Periodontitis is a non-communicable disease induced by dental plaque and host-mediated inflammatory destruction of tooth-supporting tissues^(1)^, with a prevalence of 50% in China and 40% in the United States, making it the sixth most common disease^(2,3)^. A substantial body of evidence links periodontitis to several systemic diseases^(4)^ such as atherosclerotic disease^(5)^, cardiovascular diseases (CVD)^(6,7)^, diabetes mellitus (DM)^(8,9)^, rheumatic disease^(10)^, Alzheimer’s disease^(11)^, and chronic lower respiratory diseases^(12)^. Moreover, periodontal therapy may improve systemic disease outcomes in patients with periodontitis, for example, by improving arterial stiffness for its beneficial effects on flow-mediated dilatation and carotid intima-media thickness^(13)^, and lowering glycated haemoglobin in diabetic patients^(14)^, resulting in a growing interest in periodontitis.
Nutrients derived from the diet are essential for lifelong health and development by providing a vital energy source and essential cofactors required for enzymes to function, structural moieties, and transport^(15)^. Magnesium, one of the nutrients, plays an important role in regulating oxidative stress and inflammatory responses^(16)^. Studies support the statement that the deficiency of magnesium may have a significant contribution to the occurrence of periodontitis^(17–19)^ and systemic diseases^(20–25)^. An investigation involving 4290 participants indicated that the periodontal health of subjects taking magnesium-containing drugs was improved compared with nonusers of magnesium-containing drugs^(26)^. Therefore, deterioration of periodontal health should be viewed as an early warning sign to control the quality of the patient’s diet in order to reduce the risk of developing systemic diseases later in life. These suggestions may have significance in obesity, which is characterised as a chronic low-grade inflammation component, and shares a comorbidity effect with common non-communicable diseases^(27)^. However, the relationships between magnesium, obesity, and periodontitis are uncertain. To our knowledge, there was limited information available on whether the correlation between dietary magnesium intake and oral health remains consistent in non-obese and obese populations. Therefore, the current study analysed the data from the National Health and Nutrition Examination Survey (NHANES, 2009–2014) aiming to evaluate the potential association between dietary magnesium intake and periodontitis in the obese population which would be defined by body mass index (BMI) and waist circumference (WC).
Methods
Study population
The current study collected data from NHANES, a complex, multistage, probability sampling survey designed to assess the health and nutritional status of the non-institutionalised United States population. The NHANES interview includes demographic, socioeconomic, dietary, and health-related questions. The examination component consists of medical, dental, and physiological measurements, as well as laboratory tests administered by highly trained medical personnel. According to NHANES standards for periodontal exams, only participants who were 30 years of age or older and who retained at least one natural tooth performed periodontal exams. Therefore, the exclusion criteria for this study were (1) people who did not receive periodontal exams (people younger than 30 years of age or without a single natural tooth); (2) people without valid data of two 24-hour dietary magnesium intake; (3) people without weight, height, and WC data; (4) pregnant women; (5) people without data for potential confounders (including age, gender, race, educational attainment, smoke status, alcohol use status, DM, CVD, and hypertension). We selected 30,468 participants from 3 survey cycles over six years (2009–2014). 10714 participants with periodontal examination data were enrolled in the study. Then we excluded 1633 participants without valid data on two 24-hour dietary magnesium intake, 213 participants with missing data on weight, height, and WC, and 482 participants with missing information on potential confounders or who were pregnant, leaving a total of 8385 subjects included in the analysis (Fig. 1).
Fig. 1.Flowchart for the selection of eligible participants. Abbreviation: NHANES, National Health and Nutrition Examination Survey; WC, waist circumference; DM, diabetes mellitus; CVD, cardiovascular disease.
Definition of general obesity and abdominal obesity
BMI is calculated by dividing weight in kilograms by height square in metres. In accordance with World Health Organization classification (WHO), cut-off points recommendations for the increased risk of metabolic complications (WHO, 2008), general obesity was characterised by a BMI greater than 30 kg/m^2^, and abdominal obesity was defined as having a WC >102 cm in men and >88 cm in women.
Definition of periodontal disease
Periodontitis data were obtained from Oral Health-Periodontal in Examination Data of NHANES 2009–2014. Participants aged ≥ 30 years were eligible for a full-mouth periodontal examination if they had ≥1 natural tooth present. In this study, we used the criteria proposed by Eke et al.^(28)^. Two sets of clinical periodontal measurements were included: clinical attachment loss (AL) and probing depth (PD). The Centers for Disease Control and Prevention and the American Academy of Periodontology (CDC-AAP) definition was used to define periodontitis. The classification of periodontitis includes four categories: no, mild, moderate, and severe. Mild periodontitis was characterised by the presence of at least two interproximal sites with AL ≥ 3 mm or more and at least two interproximal sites with PD ≥ 4 mm (not on the same tooth) or one site with PD ≥ 5 mm. Moderate periodontitis was characterised by the presence of at least two interproximal sites with AL ≥ 4 mm (not on the same tooth) or at least two interproximal sites with PD ≥ 5 mm (not on the same tooth). Severe periodontitis was characterised by the presence of at least two interproximal sites with AL ≥ 6 mm (not on the same tooth) and at least one interproximal site with PD ≥ 5 mm. Therefore, no periodontitis was no evidence of mild, moderate, or severe periodontitis. In this study, periodontitis was dichotomised into two groups, present or absent, meaning that participants with mild, moderate, or severe periodontitis were all categorised as having periodontitis.
Dietary magnesium intake
Trained interviewers conducted two 24-hour dietary recalls to assess total dietary intakes using the Automated Multiple Pass Method (AMPM), a structured interview where participants reported all foods and beverages consumed over the previous 24 hours. The amount of food/beverage consumed is estimated in grams. The magnesium content of foods was estimated using the U.S. Department of Agriculture Food and Nutrient Database for Dietary Studies (FNDDS), which matches reported foods to standardised nutrient values. More details can be found in the Protocol and Procedure of dietary interview in NHANES database. The first 24-hour personal interview was conducted face-to-face in the Mobile Examination Center, and the second was conducted by telephone around 3–10 days later. Dietary magnesium intakes were calculated from the average of data from two dietary recalls. The amount of dietary magnesium intake was separated by quartiles: Q1 (≤ 215.5 mg/d), Q2 (215.6–282 mg/d), Q3 (282.1-368 mg/d) and Q4 (≥ 368.1 mg/d) for data analysis.
Covariates
Demographic data comprised age (30–59 and ≥ 60 years), gender (male, female), race/ethnicity (White, Black, Mexican American, Other Hispanic, Other Race), and education level (Less Than High School, and High School and above). Smoking status was classified as never smokers, current smokers, and former smokers, based on the answers to the question of whether they have smoked at least 100 cigarettes in their lifetime and whether they were currently smoking. Alcohol status was categorised into five groups: never drinkers (less than 12 drinks throughout their lifetime), former drinkers (more than 12 drinks in their lifetime but not in the past year), mild drinkers (an average intake of no more than 1 drink per day for women and 2 drinks per day for men), moderate drinkers (an average intake of no more than 2 drinks per day for women and 3 drinks per day for men, with ≥ 2 binge drinking days per month) and heavy drinkers (an average of 3 or more drinks per day for women and 4 or more drinks per day for men, with 5 or more binge drinking days per month). DM, CVD, and hypertension were classified based on self-reported.
Statistical analysis
The statistical analysis was conducted in accordance with guidelines from the Centers for Disease Control and Prevention (https://wwwn.cdc.gov/nchs/nhanes/tutorials/default.aspx). Given the complex probabilistic clustering design of NHANES, which assigns individual sample weights to each respondent, weights were accounted for in all statistical analyses in this study. For the dietary recall interviews, the dietary data are weighted using the respective dietary weight (WTDR2D) for each cycle. Given the proportions of each cycle in the survey design, the weight for each cycle is calculated as 2/6 * WTDR2D. We analysed the data using appropriate sampling weights (1/3 * WTDR2D) to account for the complex survey design used in the NHANES survey.
Continuous variables were converted to categorical variables. The categorical variables are reported as weighted frequencies and weighted percentages. Survey-weighted chi-squared tests were utilised to assess differences of participants with and without periodontitis. Weighted logistic regression was applied to estimate odds ratios (OR) and a corresponding 95% confidence interval (CI) for the associations of dietary magnesium intake with periodontitis. Model 1 was unadjusted for covariates, Model 2 was adjusted for age, gender, and race/ethnicity. Model 3 was additionally adjusted by BMI, WC, education level, smoking status, alcohol drinking status, DM, hypertension, and CVD. Furthermore, subgroup analysis was performed to investigate the potential effect of modification of BMI and WC on the association between magnesium consumption and periodontitis.
The statistical analysis was performed using R version 4.2.1 and the NHANES R package, and p < 0.05 was considered statistically significant.
Results
The characteristics of the study population
Table 1 compares the main characteristics of the enrolled subjects based on with or without periodontitis in this study. The prevalence of periodontitis was 49.91%. Compared to the non-periodontitis group, subjects in the periodontitis group were more likely to be older, male, non-Hispanic white, and educated below high school. Participants with general or abdominal obesity were more prone to periodontitis. Those who were never smokers and mild/moderate alcohol users had a lower proportion of periodontitis. Participants with a lower magnesium intake, DM, CVD, and hypertension had a significantly higher prevalence of periodontitis.
Table 1.Descriptive characteristics of the study population stratified by periodontitisCharacteristicTotalNon-periodontitisPeriodontitisp-value(N = 8385)(N = 4200)(N = 4185)n (%)n (%)n (%)Age<0.001 30–59 years5594(66.71)3175(79.72)2419(63.70) ≥ 60 years2791(33.29)1025(20.28)1766(36.30)Gender<0.001 Female4233(50.48)2483(56.75)1750(41.81) Male4152(49.52)1717(43.25)2435(58.19)Race<0.001 Mexican American1164(13.88)427(5.59)737(10.97) Non-Hispanic black1714(20.44)689(7.91)1025(14.21) Non-Hispanic white3823(45.59)2187(75.07)1636(61.89) Other Hispanic830(9.9)410(4.78)420(6.06) Other races854(10.18)487(6.66)367(6.87)Education level<0.001 Less than high school697(8.31)198(2.38)499(7.14) High school and above7688(91.69)4002(97.62)3686(92.86)BMI0.02 < 30 kg/m^2^ 5069(60.45)2602(64.16)2467(60.49) ≥ 30 kg/m^2^ 3316(39.55)1598(35.84)1718(39.51)WC0.01 Normal3396(40.5)1747(42.75)1649(38.29) High4989(59.5)2453(57.25)2536(61.71)Magnesium intake0.01 Q12102(25.07)947(19.82)1155(24.00) Q22096(25)1061(23.86)1035(24.33) Q32094(24.97)1081(27.11)1013(26.67) Q42093(24.96)1111(29.21)982(24.99)Smoke<0.001 Former2185(26.06)995(25.27)1190(28.63) Never4705(56.11)2717(64.47)1988(45.56) Current1495(17.83)488(10.26)1007(25.80)Alcohol User<0.001 Former1461(17.42)579(11.38)882(19.26) Heavy1462(17.44)650(16.12)812(18.73) Moderate1288(15.36)760(19.85)528(15.16) Mild3102(36.99)1685(42.66)1417(35.95) Never1072(12.78)526(9.99)546(10.90)DM1130(13.48)403(6.80)727(13.31)<0.001CVD710(8.47)222(4.37)488(11.28)<0.001Hypertension3738(44.58)1587(34.90)2151(46.95)<0.001Abbreviation: BMI, body mass index; WC, waist circumference; DM, diabetes mellitus; CVD, cardiovascular disease.
Association between dietary magnesium intake and periodontitis
The correlation between dietary magnesium intake and periodontitis is presented in Table 2. We found that participants with the highest quartile of the dietary magnesium intake were less likely to have the risk of periodontitis compared with the lowest quartile of magnesium intake (OR: 0.71; 95%CI: 0.58-0.86; p < 0.001), and the trend p-value was 0.002 in the unadjusted model. After controlling for covariates (Model 2 and Model 3), participants with the highest magnesium consumption had a 39% and 28% lower risk of periodontitis, respectively (Model 2: OR: 0.61; 95%CI: 0.48-0.77; p < 0.001; Model 3: OR: 0.72; 95%CI: 0.57-0.92; p = 0.009).
Table 2.Weighted association between dietary magnesium intake and periodontitisMagnesium intakeOR (95% CI), p-valueModel 1Model 2Model 3Q1ReferenceReferenceReferenceQ20.84 (0.70, 1.01) 0.0680.80 (0.65, 0.98) 0.0360.89 (0.73, 1.08) 0.2Q30.81 (0.65, 1.01) 0.0600.76 (0.60, 0.96) 0.0230.86 (0.68, 1.09) 0.2Q40.71 (0.58, 0.86) <0.0010.61 (0.48, 0.77) <0.0010.72 (0.57, 0.92) 0.009P for trend0.002<0.0010.012Model 1 unadjusted.Model 2 adjusted for age, gender and race.Model 3 adjusted for age, gender, race, body mass index, waist circumference, education level. Smoking status, alcohol drinking status, diabetes, hypertension, and cardiovascular disease.p < 0.05 indicates statistical significance.
Subgroup analyses
Subgroup analyses and interaction tests stratified by BMI and WC were performed to assess whether the relationship between magnesium intake and periodontitis was consistent in the general population and to identify any potentially different population settings (Fig. 2). For participants without general obesity, the higher dietary magnesium intake was associated with periodontitis (p for trend = 0.02). Furthermore, the association was still relevant in subjects without abdominal obesity (p for trend = 0.02). Conversely, in the general obesity and abdominal obesity subgroups, the relationship between dietary magnesium intake and periodontitis was not significant (general obesity: p for trend = 0.15; abdominal obesity: p for trend = 0.05).
Fig. 2.Subgroup analyses for the association between dietary magnesium intake and periodontitis stratified by BMI and WC. Abbreviation: BMI, body mass index; WC, waist circumference; DM, diabetes mellitus; CVD, cardiovascular disease.
Discussion
The current study revealed a negative association between dietary magnesium intake and periodontitis, but the association was not significant in general obese or abdominal obese populations. The prevalence of periodontitis differed among different socio-demographic segments of the population. The prevalence of periodontitis increases with advancing age. Males, non-Hispanic Whites, and those with general obesity, abdominal obesity, DM, CVD, and hypertension were more likely to suffer from periodontal health problems. Never smokers, mild/moderate alcohol users, and participants with higher education levels had a lower prevalence of periodontitis. The results are consistent with previous studies on periodontitis using the NHANES database^(29–31)^.
The essential function of magnesium in the human body is attributed to its role as a cofactor in more than 300 enzyme systems that regulate a variety of biochemical reactions in the body, including cellular energy metabolism, inflammation, nucleic acid metabolism, protein synthesis, and electrolyte balance^(32)^. Studies confirmed that magnesium was significantly and inversely associated with the concentrations of diverse inflammatory cytokines^(33–36)^. The primary mechanism by which magnesium deficiency has this effect is related to magnesium’s role as a physiologic Ca2+ channel blocker. When magnesium is insufficient, cellular Ca2+ increases, which is the signal that results in the priming of cells to give the inflammatory response^(37)^. Periodontitis, a chronic inflammatory periodontal health condition, has been suggested to be linked to magnesium consumption by a number of studies. Marina et al. verified that a deficiency of magnesium influences periodontitis through systemic loss of bone mass and aggravates inflammatory bone resorption^(38)^. Furthermore, magnesium deficiency has been shown to alter the phenotypic profile of immune cell infiltrate^(18,39)^, suggesting that it might influence immune-mediated tissue destruction in periodontitis. Magnesium, one of the six micronutrients (vitamin A, C, E, selenium, magnesium, and zinc) in the daily diet, was used to calculate dietary antioxidant quality score, and Tianyi et al. analysed data from the NHANES for 2009 to 2014 and found that high-quality group of dietary antioxidant quality score was related to the decreased risk of periodontitis^(17)^. Taking into account that the dietary antioxidant quality score reflects the interactions of multiple nutrients and does not represent the role of a single nutrient, Xin-Yu Li et al. only focused on dietary magnesium intake, treated dietary magnesium intake by quintiles, and confirmed that insufficient magnesium consumption was associated with periodontitis^(19)^. However, the study population was relatively sizable, including only one cycle data from the NHANES, and missed the obesity subgroup when performing stratified analysis. When analysing the relationship between dietary magnesium intake and periodontitis, it is necessary to attach importance to the issue of obesity, since there are different opinions on the relationship between obesity and both magnesium intake and periodontitis.
That magnesium deficiency appeared to be a high-risk factor for obesity was proved in a longitudinal study^(40)^. Comparing the highest to the lowest quintile of dietary magnesium intake, the risk of central obesity was reduced by 18%^(41)^. In Mexican adults, an increase in 10 mg per 1000 kcal/day of magnesium was associated with an average decrease of 0.72% in BMI and 0.49 cm in WC^(42)^. Similarly, several clinical studies have shown that obesity seems to increase the risk of periodontitis^(43)^. It was verified that people with high obesity indices, including BMI, WC, WC-to-height ratio, waist-to-hip ratio, and visceral adiposity index had higher hazards of periodontal disease progression events^(44–47)^. On the contrary, many studies have reached inconsistent conclusions. Studies revealed that the associations between magnesium consumption and body composition indices were meaningless^(48,49)^. In Australian adults, there was a positive association between overweight/weight and periodontitis, but the statistical significance disappeared after adjustment^(50)^. A study of the Fourth Korean National Health and Nutrition Examination Survey led to the conclusion that a high WC seemed to be associated with periodontal infections, whereas BMI was not^(51)^. According to a 4-year study conducted by Tuomas et al. there was no evidence that overweight and obesity can be considered important risk factors in the pathogenesis of periodontitis^(52)^. In consideration of the above conflicting views, further analysis of the correlation between magnesium intake and periodontitis in different BMI and WC groups.
In the current cross-sectional study, we utilised the data of three survey circles from the NHANES (2009–2014) and applied the procedures for participant selection and inclusion, resulting in a total of 8385 participants enrolled for the final analysis. The covariates included age, gender, race, BMI, WC, education level, smoking status, alcohol drinking status, DM, hypertension, and CVD. We came to the same conclusion that the magnesium consumption levels were negatively associated with the prevalence of periodontitis in unadjusted and adjusted models. Furthermore, when performing stratified analysis, this association remained significant only in populations without general obesity or abdominal obesity. One possible reason is that the beneficial role of nutrients appears to be relatively limited when an individual is obese. Obesity signals that the body already has an aggravated systemic inflammation, more severe insulin resistance, and decreased immune function, which is associated with a massive release of a range of inflammatory factors. Adipose tissue secretes a biologically active substance called ‘adipocytokine’, which may be potentially harmful to periodontal tissues and that plasminogen activator inhibitor-1 expressed in visceral fat induces visceral blood coagulation and increases the risk of ischaemic vascular disease, which may also reduce blood flow to the periodontium in obese individuals, and promote periodontal disease^(53)^. The research conducted by Tianyi et al. can support this conjecture. They found that in participants with DM or hyperlipidaemia or both, which are generally considered to be closely related to obesity and chronic inflammation, the association between dietary antioxidant quality score and periodontitis was not significant^(17)^. Another reason may be that individuals with obesity have increased concentrations of cortisol in the blood and urine and that this hormone plays a role in the compartmentalisation of the minerals zinc, selenium, and magnesium, ultimately leading to hypozincemia, hyposelenemia, and hypomagnesemia and increased urinary excretion of these minerals^(54)^. The lower intracellular concentration of magnesium may impair the physiologic function of this nutrient^(55)^. However, these findings still need to be confirmed in future studies.
There are several limitations in the current study: First, as a cross-sectional study, we were unable to determine a causal relationship between magnesium consumption and periodontitis. Second, the data in this study was from the NHANES and applied primarily to the U.S. population. Third, there may be recall bias as the dietary data from NHANES relies on self-reporting. Finally, we cannot completely exclude residual confounding.
Conclusions
Collectively, these results implied that there was a correlation between dietary magnesium intake and periodontitis in the American population, but this correlation was attenuated in obese populations. This might be related to the fact that magnesium levels decrease in obesity or that the more severe levels of inflammation induced by obesity itself outweigh the anti-inflammatory effects of dietary magnesium. The study emphasised that people should be more aware of lifestyle modification interventions such as healthy diets to successfully tackle multimorbid periodontitis and other chronic diseases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Belibasakis GN , Belstrøm D , Eick S , Gursoy UK , Johansson A , Könönen E. Periodontal microbiology and microbial etiology of periodontal diseases: historical concepts and contemporary perspectives. Periodontology. 2000:1–17.10.1111/prd.1247336661184 · doi ↗ · pubmed ↗
- 2Zhang Q , Li Z , Wang C , et al. Prevalence and predictors for periodontitis among adults in China, 2010. Global Health Action. 2014;7:24503.25008055 10.3402/gha.v 7.24503 PMC 4090366 · doi ↗ · pubmed ↗
- 3Kwon T , Lamster IB , Levin L. Current concepts in the management of periodontitis. Int Dental J. 2021;71(6):462–476.10.1111/idj.12630 PMC 927529234839889 · doi ↗ · pubmed ↗
- 4Isola G , Polizzi A , Serra S , Boato M , Sculean A. Relationship between periodontitis and systemic diseases: a bibliometric and visual study. Periodontology. 2000. Published ahead of print, January 8, 2025.10.1111/prd.12621 PMC 1284284739775963 · doi ↗ · pubmed ↗
- 5Herrera D , Molina A , Buhlin K , Klinge B. Periodontal diseases and association with atherosclerotic disease. Periodontology 2000. 2020;83(1):66–89.32385870 10.1111/prd.12302 · doi ↗ · pubmed ↗
- 6Persson GR , Persson RE. Cardiovascular disease and periodontitis: an update on the associations and risk. J Clin Periodontol. 2008;35(8):362–379.18724863 10.1111/j.1600-051X.2008.01281.x · doi ↗ · pubmed ↗
- 7Kim JY , Lee K , Lee MG , Kim SJ. Periodontitis and atherosclerotic cardiovascular disease. Mol Cells. 2024;47(12):100146.39515611 10.1016/j.mocell.2024.100146 PMC 11612374 · doi ↗ · pubmed ↗
- 8Winning L , Patterson CC , Neville CE , Kee F , Linden GJ. Periodontitis and incident type 2 diabetes: a prospective cohort study. J Clin Periodontol. 2017;44(3):266–274.28036104 10.1111/jcpe.12691 · doi ↗ · pubmed ↗