Parental first aid literacy in epistaxis: do parents know what to do?
Alya AlZabin, Ebtesam Almajed, Reem AlTamimi, Nuwayyir Abdullah Alqasimi, Yasser Albalawi, Nasser AlWehaibi

TL;DR
This study finds that many parents in Saudi Arabia lack proper knowledge of first aid for nosebleeds in children, highlighting the need for better education.
Contribution
The study provides new insights into parental first aid literacy for epistaxis in Saudi Arabia and identifies demographic factors influencing knowledge gaps.
Findings
Only 15.8% of parents recognized posterior nosebleeds as life-threatening.
Just 54.8% knew the correct position for managing nosebleeds.
Geographic and demographic disparities were found in first aid knowledge.
Abstract
Epistaxis is a common otorhinolaryngology emergency, especially among the pediatric population. While prompt first aid is essential, there is limited data on parents’ knowledge regarding its management in Saudi Arabia. This study assessed parental literacy in epistaxis first aid and its correlation with sociodemographic factors. A cross-sectional online study was conducted from May to June 2023, targeting parents of children aged ≤12 years across Saudi Arabia. Using a structured questionnaire, data on demographic characteristics and epistaxis first aid knowledge were collected from 777 participants. Descriptive statistics and binary logistic regression were utilized for analysis. The majority of parents (79%) reported that their child had experienced epistaxis, and 72.7% considered it an emergency. However, knowledge gaps were evident: only 15.8% recognized posterior bleeds as…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1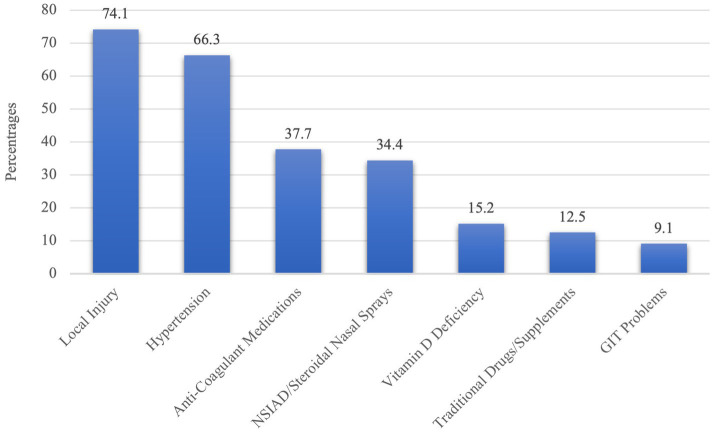 Figure 2
Figure 2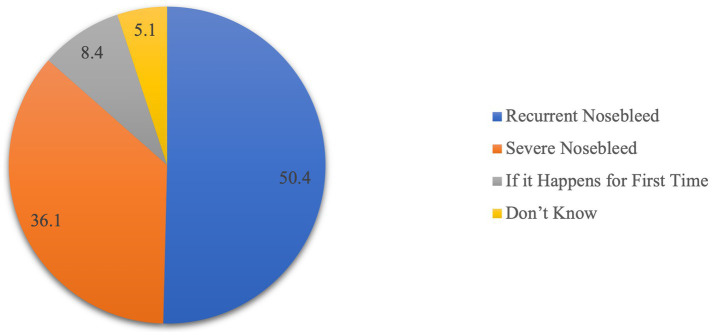 Figure 3
Figure 3| Variable |
| % | |
|---|---|---|---|
| Gender | Mother | 665 | 85.6 |
| Father | 112 | 14.4 | |
| Age | Mean (SD) | 37.2 (8.4) | |
| Range | 19–67 | ||
| Nationality | Non-Saudi | 67 | 8.6 |
| Saudi | 710 | 91.4 | |
| Marital status | Married | 728 | 93.7 |
| Divorce/Widowed | 49 | 6.3 | |
| Current residency | Western Region | 242 | 31.1 |
| Central Region | 156 | 20.1 | |
| South Region | 152 | 19.6 | |
| Eastern Region | 116 | 14.9 | |
| North Region | 111 | 14.3 | |
| Educational status | School | 192 | 24.7 |
| Bachelors | 505 | 65 | |
| Post-Graduate Degree | 80 | 10.3 | |
| Occupational status | Unemployed | 42 | 5.4 |
| Employee | 379 | 48.8 | |
| Housewife | 254 | 32.7 | |
| Student | 60 | 7.7 | |
| Retired | 42 | 5.4 | |
| Monthly income | < 5,000 SAR | 164 | 21.1 |
| 5,000–10,000 SAR | 406 | 52.3 | |
| >10,000 SAR | 207 | 26.6 | |
| Number of children | Median | 3 | 100 |
| Range | 1–10 | ||
| Age of oldest child | Mean (SD) | 12.4 (7.4) | |
| Range | 1–31 | ||
| Age of youngest child | Mean (SD) | 5.1 (3.5) | |
| Range | 1–12 | ||
| Survey item |
| % | |
|---|---|---|---|
| Have you ever heard/witnessed/experienced nosebleeds? | No | 163 | 21 |
| Yes | 614 | 79 | |
| Do you consider nosebleeds as one of the emergencies? | No | 212 | 27.3 |
| Yes | 565 | 72.7 | |
| Have you ever received any training or awareness program on first-aid management? | No | 412 | 53 |
| Yes | 365 | 47 | |
| Epistaxis is Bleeding from | I do not know | 16 | 2.1 |
| Nose | 748 | 96.3 | |
| Ear | 13 | 1.7 | |
| Which of the following can be a life-threatening nosebleed? | Anterior | 79 | 10.2 |
| Lateral | 17 | 2.2 | |
| Medial | 21 | 2.7 | |
| Posterior | 123 | 15.8 | |
| I do not know | 537 | 69.1 | |
| For how long shall nose pinching be performed? (mins) | At least 10 to 15 min | 234 | 30.1 |
| At least 20 min | 15 | 1.9 | |
| At least 5 min | 384 | 49.4 | |
| I do not know | 144 | 18.5 | |
| For how long shall nose pinching in children be performed? (mins) | At least 10 to 15 min | 144 | 18.5 |
| At least 20 min | 26 | 3.3 | |
| At least 5 min | 427 | 55 | |
| I do not know | 180 | 23.2 | |
| Which part of the nose shall be pinched with fingers to stop nose bleeding? | Bony (upper part) | 261 | 33.6 |
| Cartilage (lower part) | 262 | 33.7 | |
| Both | 135 | 17.4 | |
| I do not know | 119 | 15.3 | |
| What care should be taken for breathing during nose pinching? Breathing shall be | Allowed through mouth avoiding blood swallowing | 555 | 71.4 |
| Halted during nose pinching | 20 | 2.6 | |
| Maintained through oxygen pump | 19 | 2.4 | |
| I do not know | 183 | 23.6 | |
| What is the proper position that a patient with epistaxis should take? | Lying down with ice pack over the nasal bridge | 80 | 10.3 |
| Sitting with head tilted backward | 187 | 24.1 | |
| Sitting with head tilted forward | 426 | 54.8 | |
| I do not know | 84 | 10.8 | |
| Do you think sucking an ice cube can help in reduction of nose bleeding? | No | 231 | 29.7 |
| Yes | 231 | 29.7 | |
| I do not know | 315 | 40.5 | |
| Do you think the icing on the neck region may help in the management of epistaxis? | No | 282 | 36.3 |
| Yes | 116 | 14.9 | |
| I do not know | 379 | 48.8 | |
| Do you think cooling or icing on the nose helps in slowing blood flow from the nose? | No | 102 | 13.1 |
| Yes | 461 | 59.3 | |
| I do not know | 214 | 27.5 | |
| If your child’s nose is bleeding, how would you stop it? | Obstruct nose with cotton | 100 | 12.9 |
| Obstruct nose with tissue paper | 95 | 12.2 | |
| Pinching the nose | 497 | 64 | |
| Other method | 85 | 10.9 | |
| Scenario to seek ER care | Mean (SD) | Mean rank |
|---|---|---|
| If the bleeding is severe, causing breathing difficulty (dyspnea) | 4.54 (1.2) | 1st |
| If the bleeding still does not stop even after performing first aid | 4.44 (1.2) | 2nd |
| If the nosebleeds are severe, and the person suffers chest pain, or feels dizzy | 4.42 (1.2) | 3rd |
| If the person appears pale or fatigued | 4.38 (1.3) | 4th |
| If the nosebleeds occur frequently, or when bruises appear in the body or bleeding from other places, while current bleeding does not stop | 4.33 (1.3) | 5th |
| If bleeding occurs after surgery close to the nose, or if the person has a nasal tumor | 4.32 (1.3) | 6th |
| If the person is taking anticoagulant medications, such as aspirin, clopidogrel, or warfarin, while nosebleeds do not stop | 4.23 (1.3) | 7th |
| If bleeding occurs after a facial injury | 4.21 (1.4) | 8th |
| Preventive measure | Strongly disagree/disagree | Neutral | Strongly agree/agree | |
|---|---|---|---|---|
| Local application of bacitracin or petrolatum ointment |
| 392 | 228 | 157 |
| % | 50.5 | 29.3 | 20.2 | |
| Use nasal saline spray |
| 307 | 270 | 200 |
| % | 39.5 | 34.7 | 25.7 | |
| Humidifying the air with a cool mist vaporizer |
| 180 | 255 | 342 |
| % | 23.2 | 32.8 | 44.0 | |
| Should sneeze gently with the mouth open |
| 184 | 272 | 321 |
| % | 23.7 | 35.0 | 41.3 | |
| Avoid digital trauma (e.g., nose picking) by keeping the child’s nails well-trimmed |
| 129 | 122 | 526 |
| % | 16.6 | 15.7 | 67.7 | |
| Avoid strenuous activities |
| 145 | 179 | 453 |
| % | 18.7 | 23.0 | 58.3 | |
| Avoid hot showers |
| 173 | 236 | 368 |
| % | 22.3 | 30.4 | 47.4 | |
| Avoid nose blowing and excessive sneezing |
| 136 | 196 | 445 |
| % | 17.5 | 25.2 | 57.3 | |
| Avoid hot and spicy foods and drink plenty of fluids |
| 191 | 234 | 352 |
| % | 24.6 | 30.1 | 45.3 | |
| Predictor variable |
| Sig. | aOR | 95% CI | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Gender (male) | −0.108 | 0.721 | 0.898 | 0.496 | 1.624 |
| Age of parents | 0.023 | 0.302 | 1.023 | 0.980 | 1.068 |
| Nationality (Saudi) | 0.081 | 0.829 | 1.084 | 0.521 | 2.258 |
| Current Residency (Western) | 0.027* | ||||
| Current Residency (Central) | −0.490 | 0.112 | 0.613 | 0.335 | 1.120 |
| Current Residency (South) | −0.961 | 0.001* | 0.382 | 0.213 | 0.685 |
| Current Residency (Eastern) | −0.488 | 0.153 | 0.614 | 0.314 | 1.199 |
| Current residency (North) | −0.750 | 0.027* | 0.472 | 0.243 | 0.918 |
| Marital status (divorced/widow) | 0.036 | 0.934 | 1.037 | 0.441 | 2.438 |
| Highest educational (post-graduate) | −0.257 | 0.188 | 0.774 | 0.528 | 1.133 |
| Occupation status (unemployed) | 0.775 | ||||
| Occupation status (employee) | 0.060 | 0.894 | 1.062 | 0.443 | 2.545 |
| Occupation status (housewife) | −0.138 | 0.758 | 0.871 | 0.363 | 2.092 |
| Occupation status (student) | 0.395 | 0.463 | 1.485 | 0.516 | 4.271 |
| Occupation status (retired) | 0.173 | 0.810 | 1.189 | 0.291 | 4.861 |
| Household income | 0.193 | 0.247 | 1.213 | 0.875 | 1.682 |
| Number of children | 0.011 | 0.919 | 1.011 | 0.822 | 1.244 |
| Age of oldest child | −0.016 | 0.638 | 0.984 | 0.920 | 1.053 |
| Age of youngest child | 0.031 | 0.492 | 1.032 | 0.944 | 1.129 |
| Constant | 1.299 | 0.184 | 3.667 | ||
| Predictor variable |
| Sig. | aOR | 95% CI | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Gender (male) | −0.468 | 0.039* | 0.626 | 0.402 | 0.976 |
| Age of parents | −0.003 | 0.825 | 0.997 | 0.966 | 1.028 |
| Nationality (Saudi) | −0.560 | 0.044* | 0.571 | 0.331 | 0.985 |
| Current residency (Western) | 0.493 | ||||
| Current residency (Central) | −0.300 | 0.157 | 0.741 | 0.489 | 1.123 |
| Current residency (South) | −0.266 | 0.224 | 0.767 | 0.500 | 1.177 |
| Current residency (Eastern) | −0.259 | 0.283 | 0.772 | 0.481 | 1.238 |
| Current residency (North) | −0.006 | 0.981 | 0.994 | 0.613 | 1.612 |
| Marital status (divorced/widow) | 0.055 | 0.860 | 1.056 | 0.575 | 1.942 |
| Highest educational (post-graduate) | −0.297 | 0.046* | 0.743 | 0.555 | 0.995 |
| Occupation status (unemployed) | 0.012* | ||||
| Occupation status (employee) | 0.314 | 0.362 | 1.369 | 0.696 | 2.692 |
| Occupation status (housewife) | −0.342 | 0.327 | 0.710 | 0.359 | 1.407 |
| Occupation status (student) | −0.432 | 0.307 | 0.649 | 0.283 | 1.488 |
| Occupation status (retired) | 0.193 | 0.690 | 1.212 | 0.470 | 3.127 |
| Household income | 0.043 | 0.727 | 1.044 | 0.820 | 1.329 |
| Number of children | −0.018 | 0.812 | 0.982 | 0.847 | 1.139 |
| Age of oldest child | 0.006 | 0.805 | 1.006 | 0.959 | 1.055 |
| Age of youngest child | −0.001 | 0.985 | 0.999 | 0.936 | 1.067 |
| Constant | 1.045 | 0.145 | 2.844 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Anomalies and Treatments · Tracheal and airway disorders · Foreign Body Medical Cases
Introduction
1
Epistaxis is defined as bleeding from the nasal cavity or the nasopharynx. Among pediatric patients, epistaxis is one of the most common acute otorhinolaryngology emergencies; the incidence of epistaxis is rare during the first 2 years of life, but it increases rapidly afterward (1). Epistaxis can be classified as anterior or posterior epistaxis. Anterior epistaxis occurs more frequently. In contrast, posterior epistaxis is less common (2).
As an urgent medical emergency, epistaxis requires first aid to reduce pain and prevent deterioration (3). The primary objectives of a first aid provider are to preserve life, alleviate suffering, prevent further illness or injury, and to promote recovery (4). Per guidelines issued by the Ministry of Health (MOH) of Saudi Arabia, epistaxis first aid involves holding the lower portion (cartilage) of the nose on both sides while bending forward. Ideally, the pressure should be applied for at least 5 min for children and 10 to 15 min for adults. A cold pack may be applied if necessary. Emergency medical attention should be sought if the bleeding persists for more than 30 min (5).
Children are at risk for developing epistaxis spontaneously and due to trauma. However, most parents may not be familiar with the proper first aid management of epistaxis. A recent study led in 2021 conducted in AlQassim region focused explicitly on mothers’ knowledge of first aid measures. The findings of this study highlighted that only 38% of mothers knew how to help a child who had a nosebleed (6). Another cross-sectional study investigated the knowledge and practice of first aid among parents attending primary health care centers in Madinah city in Saudi Arabia. According to the study results, only 27.9% of the 390 parents correctly answered the question regarding how to manage a case of epistaxis (7). In Buraidah City, Saudi Arabia, Bassam (8) conducted a study to evaluate maternal knowledge and attitudes regarding first aid. The study sample consisted of 1,000 mothers. The study results indicated that less than half (45%) of mothers knew the correct epistaxis first aid (8). A quasi-experimental study evaluated how educational guidelines affect mothers’ performance regarding care for children with epistaxis. According to this study, 68.6% of mothers had unsatisfactory practices regarding epistaxis pre-educational guidelines (9).
To our knowledge, no nationwide study has been conducted on parents’ knowledge of epistaxis first aid in Saudi Arabia. Despite being common, there is a lack of general awareness of how to treat this condition among parents. Most of a child’s time is spent at home with their parents. A child’s curiosity makes them susceptible to unintentional injuries. If parents intervene quickly and correctly, they can limit the severity of the child’s injuries. Herein, this study aims to assess the literacy of parents in Saudi Arabia regarding epistaxis first aid and pediatric epistaxis and whether literacy score correlates with different sociodemographic factors.
Materials and methods
2
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board at Princess Nourah bint Abdulrahman University (PNU) (IRB log number: 23-0323). All participants were provided with informed consent prior to the commencement of the study. The research objectives were explained to all participants, and it was clarified that they could withdraw from the study without any consequences.
Sample and data collection
2.1
An online-based cross-sectional study with national coverage was conducted in Saudi Arabia. Saudi Arabia is the largest country in the Arabian Peninsula, spans 2.15 million square kilometers. It has five major regions (Central, Western, Eastern, Northern, and Southern) and a population of around 36 million as of 2024. The country has a well-developed healthcare system with both public and private sectors. Study participants were recruited from the five major regions and data collectors who resided in the corresponding region distributed the survey to ensure a representative sample. We used convenience sampling, distributing the survey through social media (X, WhatsApp, and Instagram) and parenting groups. The study was conducted from May 2023 to June 2023. The Inclusion criteria included (1) Parents aged 18 and older with children aged ≤ 12 years, (2) currently residing in Saudi Arabia, and (3) agreed to participate and complete the questionnaire. No gender restrictions were applied. The exclusion criteria included (1) individuals who did not consent to participate and (2) participants who did not complete the questionnaire. The sample size was estimated based on a power of 80% with a margin error of 5% and a confidence level of 95%; the minimum sample size required was 610 participants, as computed by G-power software. The total sample size comprised 777 participants; additional responses were accepted to account for potential incomplete responses and ensure robust statistical analysis across different subgroups.
Study survey
2.2
The study employed a self-administered questionnaire modified from previous studies in alignment with the study’s objectives (2, 10–12). All data were obtained and managed using Google Forms electronic tool. The questionnaire was reviewed first by a clinical expert on the subject and an emergency consultant then was piloted on a cohort of non-medical people. Data was collected from participants using a questionnaire consisting of two sections. (1) Sociodemographic data questions included age, nationality, current residency, marital status, highest educational level, occupation status, Household Income (HHI), number of children, and the age of the oldest and youngest child. (2) Parents’ literacy toward epistaxis first aid and its prevention.
Statistical analysis
2.3
A comprehensive statistical analysis was conducted on the dataset, encompassing both descriptive and inferential methodologies. Firstly, a descriptive analysis was conducted to summarize the demographic characteristics of the participants, which included age, gender, and other features. This provided an overview of the study population. Subsequently, the Binary Logistic Regression Model was employed to determine the predictors of high literacy of Epistaxis First Aid and Prevention in Saudi Arabia. Statistical significance was established at a p-value of 0.05 or lower and a 95% Confidence Interval (CI). All statistical analyses were executed using IBM’s SPSS Software, version 29.0.
Results
3
Seven hundred seventy-seven parents residing in Saudi Arabia enrolled themselves electively and completed the study questionnaire. The participants’ sociodemographic characteristics are displayed in Table 1. Notably, the majority were mothers (85.6%, n = 665), while fathers constituted 14.4% (n = 112). The average age was 37.2 years (SD = 8.4), with a range of 19 to 67 years. Our sample predominantly comprised Saudi parents (91.4%, n = 710) and married participants (93.7%, n = 728). Geographically, the Western Region had the highest representation (31.1%, n = 242). Educationally, 65.0% (n = 505) held a bachelor’s degree, and most were employed (48.8%, n = 379). Monthly income varied, with 52.3% (n = 406) earning 5,000–10,000 SAR. The median number of children was 3, with an average age of 12.4 years (SD = 7.4) for the oldest child and 5.1 years (SD = 3.5) for the youngest.
Table 2 shows the assessment of parents’ literacy toward epistaxis first aid. The majority (79%, n = 614) had heard, witnessed, or experienced nosebleeds. A significant portion (72.7%, n = 565) considered nosebleeds emergencies. Regarding training, 47% (n = 365) had received first-aid management awareness. While 96.3% (n = 748) correctly identified epistaxis as bleeding from the nose. Among the types of nosebleeds, 15.8% (n = 123) recognized posterior bleeds as potentially life-threatening, while a significant portion (69.1%, n = 537) admitted uncertainty. Concerning the duration of nose pinching, 30.1% (n = 234) recommended at least 10–15 min. In the context of children, 55% (n = 427) advocated pinching for at least 5 min. The understanding of the nose’s anatomical regions to be pinched varied, with 33.6% (n = 261) answered with bony part, 33.7% (n = 262) of the participants choose the cartilage part, and 17.4% (n = 135) of both. Notably, 71.4% (n = 555) recognized that breathing should be allowed through the mouth during nose pinching. Regarding the patient’s position, 54.8% (n = 426) recommended sitting with the head tilted forward, while 24.1% (n = 187) suggested sitting with the head tilted backward. Notably, 10.8% (n = 84) were uncertain about the proper position. Regarding the use of ice cubes 29.7% (n = 231) believed that sucking an ice cube could help reduce nose bleeding. Similarly, there was uncertainty about the efficacy of icing on the neck region, with 14.9% (n = 116) believing it could help. In contrast, a majority (59.3%, n = 461) believed that cooling or icing on the nose could indeed slow blood flow. In the context of managing a child’s nosebleed, 64% (n = 497) recommended pinching the nose, while various alternative methods were suggested by 10.9% (n = 85) of participants.
Figure 1 shows the sources of information about epistaxis first aid among the participants. The majority (33.3%) reported obtaining knowledge from the Internet or social media. Friends and relatives accounted for 23.1%, indicating a significant influence from personal networks. First aid courses played a role in 18.3% of respondents’ knowledge acquisition, while self-teaching was a source for 15.8%. A smaller percentage (4.5%) mentioned the Ministry of Health as a source. Books contributed to the understanding of epistaxis first aid for 2.4%, and an equal percentage (2.4%) admitted not knowing the source of their information.
Knowledge about the source of information of epistaxis first aid.
Figure 2 shows participants’ knowledge about the risk factors of epistaxis. Local injury was identified by the majority, with 74.1% recognizing it as a risk factor. Hypertension was well-acknowledged, with 66.3% recognizing its association with epistaxis. Anti-coagulant medications were identified by 37.7% as a potential risk factor, and 34.4% recognized non-steroidal anti-inflammatory drugs (NSAIDs) or steroidal nasal sprays as contributing factors. Vitamin D deficiency was acknowledged by 15.2% of participants. Traditional drugs or supplements were recognized by 12.5%, while gastrointestinal (GIT) problems were identified by 9.1%.
Knowledge about the risk factors of epistaxis.
Table 3 shows the knowledge hierarchy concerning when individuals perceive it necessary to seek emergency room (ER) care for epistaxis, or nosebleeds, based on their assigned ranks and corresponding mean scores. At the forefront is the recognition that severe bleeding causing breathing difficulty (dyspnea) demands the utmost urgency, securing the top position with a mean score of 4.54 and ranking first. Subsequently, respondents emphasize the significance of persistent bleeding even after performing initial first aid (mean 4.44, 2nd rank) and nosebleeds accompanied by chest pain or dizziness (mean 4.42, 3rd rank). The fourth position is assigned to situations where the person appears pale or fatigued (mean 4.38), indicating a perceived level of urgency. The fifth and sixth ranks pertain to scenarios involving frequent nosebleeds alongside bruises or bleeding from other places (mean 4.33) and bleeding after surgery close to the nose or in the presence of a nasal tumor (mean 4.32), respectively. Following these, the seventh and eighth ranks focus on situations where individuals taking anticoagulant medications experience unstoppable nosebleeds (mean 4.23) and bleeding occurs after a facial injury (mean 4.21), respectively.
Figure 3 shows participants’ awareness regarding the appropriate times for consulting an Ear, Nose, and Throat (ENT) physician. Notably, 50.4% are aware that recurrent nosebleeds warrant consultation, suggesting a recognition of the importance of seeking medical advice for persistent issues. For severe nosebleeds, 36.1% of participants acknowledged the need for ENT consultation, indicating a reasonable understanding of the severity threshold. Only 8.4% recognized the importance of consulting an ENT physician if nose bleeding occurs for the first time, suggesting that a smaller proportion is aware of the significance of initial occurrences. Additionally, 5.1% expressed uncertainty about when to consult an ENT physician.
Participants’ awareness about the time of ENT physician consultation.
Table 4 shows parents’ literacy toward various preventive measures for epistaxis following an episode. Notably, 20.2% (n = 157) strongly agreed or agreed with the local application of bacitracin or petrolatum ointment, while 25.7% (n = 200) expressed agreement with the use of the nasal saline spray. A substantial 44.0% (n = 342) strongly agreed or agreed with humidifying the air with a cool mist vaporizer. The practice of sneezing gently with the mouth open received agreement from 41.3% (n = 321) of participants. The highest agreement was observed for avoiding digital trauma by keeping the child’s nails well-trimmed, with a significant 67.7% (n = 526) expressing approval. Avoiding strenuous activities garnered agreement from 58.3% (n = 453), while 47.4% (n = 368) agreed with avoiding hot showers. Additionally, 57.3% (n = 445) agreed with avoiding nose blowing and excessive sneezing, and 45.3% (n = 352) expressed agreement with avoiding hot and spicy foods while encouraging fluid intake.
Table 5 shows the results of a Binary Logistics Regression analysis assessing the adjusted predictors of high parents’ literacy toward epistaxis first aid management. The variables considered include Gender, Age of Parents, Nationality, Current Residency, Marital Status, Highest Educational Level, Occupation Status, Household Income, Number of Children, Age of Oldest Child, and Age of Youngest Child. Among the significant predictors, the Current Residency region plays a notable role. Parents residing in the South (B = −0.961, p = 0.001), East (B = −0.488, p = 0.153), and North (B = −0.750, p = 0.027) regions exhibited diminished odds of possessing high literacy compared to their counterparts in the Western region. This geographical discrepancy underscores the influence of regional dynamics on parental knowledge in epistaxis first aid.
Contrastingly, the occupation status of being a student (B = 0.395, p = 0.463) demonstrated a positive association with high literacy, although the lack of statistical significance suggests a need for cautious interpretation. The absence of a significant association may stem from various factors, including the diverse nature of student roles and responsibilities.
Moreover, intriguingly, several variables such as Gender, Age of Parents, Nationality, Marital Status, Highest Educational Level, Household Income, Number of Children, Age of Oldest Child, and Age of Youngest Child did not exhibit significant associations with high parents’ literacy in epistaxis first aid management. This implies that within this specific context, these factors may not be predominant influencers of parental literacy. In essence, this thorough examination sheds light on the multifaceted determinants of parental literacy in epistaxis first aid management, providing valuable insights for targeted interventions and educational initiatives.
Table 6 shows the outcomes of a Binary Logistics Regression examining adjusted predictors of high parents’ literacy regarding epistaxis prevention post-episode. Among the discerned predictors, several factors significantly impact parental literacy. Gender plays a pivotal role, with male parents demonstrating lower odds of exhibiting high literacy (p = 0.039, aOR = 0.626). This suggests a potential gender-based discrepancy in awareness and knowledge related to epistaxis prevention.
Nationality also emerges as a significant factor, with non-Saudi nationals exhibiting reduced odds of high literacy (p = 0.044, aOR = 0.571). This finding implies that cultural or contextual differences may influence the level of awareness and understanding among parents from different national backgrounds. Highest Educational Level proves to be another influential predictor, where parents with post-graduate education display lower odds of high literacy (p = 0.046, aOR = 0.743). This unexpected result challenges conventional assumptions and warrants further exploration into the dynamics of education and health literacy.
Interestingly, being unemployed is associated with increased odds of high literacy (p = 0.012), offering a unique perspective on the correlation between occupation status and epistaxis prevention knowledge. Other examined factors, including age, residency, marital status, occupation, income, and the number/ages of children, show no significant associations. These findings underscore the importance of considering diverse sociodemographic factors in tailoring educational interventions to enhance epistaxis prevention awareness among parents.
Discussion
4
To our knowledge, this is the first nationwide study in Saudi Arabia to assess parental knowledge of epistaxis first aid across all five major regions. Previous studies focused on specific cities or maternal knowledge, whereas our study provides a broader perspective by analyzing sociodemographic factors affecting first-aid literacy. Our study found that while 79% of parents had encountered epistaxis, significant knowledge gaps remained. Only 54.8% correctly identified the proper head position for nosebleed management, and just 15.8% recognized posterior bleeds as potentially life-threatening. Parental literacy varied by region, with lower knowledge levels in the South, East, and North. Additionally, non-Saudi parents and those with postgraduate education demonstrated reduced awareness of epistaxis prevention. These findings highlight the need for targeted educational programs to improve first-aid knowledge.
Epistaxis is one of the most common acute otorhinolaryngology emergencies. The incidence of epistaxis is rare during the first 2 years of life, but it increases rapidly afterward (1). Elsayed Elboraei et al. (13) reported a 47.4% occurrence rate. Controlling epistaxis and its complications, including blood loss, can severely impact a family’s quality of life (14). Merdad et al. (15) found that healthcare workers’ understanding of managing epistaxis was deficient, consequently affecting parental education. They observed a discrepancy between providers’ confidence and competence, which calls for better educational interventions. Consequently, this study assessed the literacy of first-aid management regarding epistaxis and the factors that could affect it among parents in Saudi Arabia.
In order to gain insight into the current state of knowledge regarding epistaxis first aid and to identify any gaps in the literature, an assessment of Saudi parents’ literacy regarding epistaxis first aid was conducted. In the present study, the high prevalence of reported hearing, witnessing, or experiencing epistaxis among participants (79%) may suggest a higher level of familiarity with first-aid management. However, the observed variability in understanding the correct location for applying pressure during nosebleeds and the fact that only 15.8% of participating parents correctly identified posterior nosebleeds as potentially life-threatening, in addition to over half of participants (54.8%) recommended an incorrect head position highlights a knowledge gap and contradicts our initial assumption. A thorough review of the literature by Alkhalifah et al. (16) identified 17 studies reporting 12,057 participants’ knowledge and attitudes regarding epistaxis in Saudi Arabia. According to this systematic review and meta-analysis, there are significant differences in epistaxis awareness levels based on factors such as age, gender, and geographical location. It was found that general Saudi populations and self-administered questionnaires had higher awareness levels. An estimated 63% of Saudi residents are aware of epistaxis and its management. Regarding parents’ knowledge of the risk factors of epistaxis, the majority correctly identified local injury as a primary risk factor, with 74.1% of respondents acknowledging its relevance, which was consistent with the literature (17). Hypertension was also widely recognized, with 66.3% understanding its potential association with epistaxis, aligning with established medical knowledge linking high blood pressure to an increased risk of nosebleeds (18).
While the present study identified some deficiencies of epistaxis awareness, it is crucial to acknowledge that there is some evidence of good epistaxis awareness in some aspects. According to the existing literature, the general public considers epistaxis to be a minor health concern (2, 16, 19). In contrast to our study, 72.7% of the participants considered epistaxis an emergency, which suggests a general awareness of the potential seriousness of epistaxis. This aligns with findings reported in another study (20). Furthermore, the studied sample suggests an acceptable level of parental preventative measures against epistaxis (e.g., local application of bacitracin or petrolatum ointment, digital trauma avoidance, and humidifying). Binary Logistics Regression was utilized to assess predictors of high parental literacy regarding epistaxis prevention strategies. A lower likelihood of demonstrating high literacy was observed in male parents, non-Saudi parents, and parents with higher educational attainment. These warrant further exploration and more comprehensive research is needed to investigate the association of predictive factors better.
According to our findings, only 47% of participants reported receiving first-aid training or awareness programs, which is consistent with other studies conducted in other cultural contexts as in Spain, approximately half of the respondents indicated they had received some first-aid training (21), a proportion similar to that found in a study carried out in Belgium (22), however, greater than that found in studies conducted in Turkey (23) and Greece (24). Therefore, it is imperative to disseminate first-aid knowledge widely through expanding access to first-aid training programs and incorporating basic first-aid information into public health campaigns to bridge the existing knowledge gap effectively. Our findings reveal varying levels of awareness among parents when asked about the appropriate time to consult an ENT specialist for epistaxis. Half of the participants correctly have recurrent nosebleeds that need prompt consultation. This suggests that many participants recognize the need for medical intervention when nosebleeds become a repeated concern, which is aligned with best practices in managing persistent symptoms (25).
Overall, these findings highlight the need for multifaceted educational interventions to address knowledge gaps, provide parents with accurate information regarding the management of epistaxis, and inform effective prevention strategies. Nora et al. conducted a quasi-experimental study to determine the effectiveness of epistaxis education guidelines in improving mothers’ performance in caring for children with epistaxis (9). The study concluded that, compared to the implementation level of the pre-educational guideline, mothers demonstrated significant improvement in their knowledge and attitude and reported practice scores in caring for epistaxis-affected children. Furthermore, by increasing parents’ awareness of basic management strategies, stress and intensity of this condition could be significantly reduced. Information sources vary in accuracy, completeness, and depth of coverage. Suboptimal information and outdated knowledge regarding epistaxis first aid can result in inappropriate interventions, potentially exacerbating the condition or hindering timely professional care. In order to determine the credibility and reliability of the information parents rely on to manage epistaxis, we surveyed parents about their sources of information about epistaxis first aid. Our findings indicate that the internet and social media were the predominant sources, followed by advice from friends and relatives and first aid courses, and a minority of respondents reported using Ministry of Health materials and books as their primary sources. These patterns align with those observed in studies by Saleem et al. (26) which aimed to investigate Saudi Arabians’ current understanding of epistaxis first-aid management and misconceptions, and Alam et al.’s (11) on parental knowledge of first-aid management of epistaxis in Taif, Saudi Arabia, in addition to Al-Shehri et al.’s (27) which explored the knowledge, attitude, and practice associated with first-aid management of epistaxis among the general population of Aseer, Saudi Arabia.
The limitations of the study include the self-reported nature of the research that presents as a significant limitation for the study since some parents may deliberately share inaccurate information due to looking up answers for their own questions from unreliable resources. Additionally, it might be necessary to assess their awareness by conducting interviews instead of distributing questionnaires for more cooperation and accuracy. It is recommended that a mixed-method approach should be utilized in future studies by quantitatively assessing parents’ knowledge using simulated scenarios, thus enhancing the accuracy of the results. To raise parents’ knowledge and awareness, we must focus on online initiatives and social campaigns so they can benefit from them.
Conclusion
5
This study highlights considerable knowledge gaps in epistaxis first aid among Saudi parents, emphasizing the need for targeted educational interventions. Despite a high exposure rate to epistaxis, misconceptions persist about crucial management steps, such as positioning and timing of nose pinching. Addressing these deficiencies through accessible training and standardized resources, especially in underserved regions and for demographic groups with lower literacy, can equip parents with accurate first-aid skills. Expanding community-based awareness campaigns, particularly on social media, could further enhance parental literacy and improve emergency responses to pediatric epistaxis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Intosh N Mok JYQ Margerison A. Epidemiology of oronasal hemorrhage in the first 2 years of life: implications for child protection. Pediatrics. (2007) 120:1074–8. doi: 10.1542/peds.2007-2097, PMID: 17893187 · doi ↗ · pubmed ↗
- 2Mohammad S Alsharidah A Alshehri M Asim F Alotaibi A Alghamdi E. Knowledge and practice of epistaxis first aid among adult population in Riyadh, Saudi Arabia. Int J Med Dev Count. (2020) 4:2215–21. doi: 10.24911/IJMDC.51-1603305886 · doi ↗
- 3Alqarni Z Alajmi T Alhumaidi U Alhussain A Alotaibi Y Alzahrani H. Prevalence, causes, treatment, and outcome of epistaxis. Int J Med Dev Counts. (2019) 3:446–9. doi: 10.24911/IJMDC.51-1546952315 · doi ↗
- 4Singletary EM Charlton NP Epstein JL Ferguson JD Jensen JL Mac Pherson AI. Part 15: first aid: 2015 American Heart Association and American red Cross guidelines update for first aid. Circulation. (2015) 132:S 574–89. doi: 10.1161/CIR.0000000000000269, PMID: 26473003 · doi ↗ · pubmed ↗
- 5First Aid - Epistaxis (Nosebleed). Available online at: https://www.moh.gov.sa/en/Health Awareness/Educational Content/Firstaid/Pages/014.aspx (accessed February 27, 2023)
- 6Alhajjaj F Alseleem H Alghebaiwi R Alqutaymi A Almatrouk G Alshamikh W. Knowledge, misconceptions, and practice about first aid measures among mothers in Al Qassim. Int J Med Dev Count. (2021) 5:309–17. doi: 10.24911/IJMDC.51-1607865492 · doi ↗
- 7Al-Johani AAS Sabor S Aldubai SAR. Knowledge and practice of first aid among parents attending primary health care centers in Madinah City, Saudi Arabia, a cross sectional study. J Family Med Prim Care. (2018) 7:380–8. doi: 10.4103/jfmpc.jfmpc_64_18, PMID: 30090781 PMC 6060932 · doi ↗ · pubmed ↗
- 8Bassam SEA. Evaluate maternal knowledge and attitude regarding first aid among their children in Buraidah City, Saudi Arabia kingdom (KSA). Med Arch. (2022) 76:164–9. doi: 10.5455/medarh.2022.76.164-169, PMID: 36200120 PMC 9478825 · doi ↗ · pubmed ↗