Treatment-Resistant Fulminant Septic Shock: A Case of Multidrug-Resistant Streptococcus pneumoniae Bacteremia in an Unvaccinated Intravenous Drug User
Elene Saribekovi, Elene Pachkoria, Tamar Didbaridze, Tamar Megrelishvili, Nino Gogokhia, Ia Mikadze, Levan Ratiani

TL;DR
A drug user with a severe, antibiotic-resistant Streptococcus pneumoniae infection developed fatal septic shock and ARDS, highlighting the dangers of antibiotic resistance and lack of vaccination.
Contribution
This case highlights the clinical challenges of multidrug-resistant Streptococcus pneumoniae in intravenous drug users and the importance of vaccination.
Findings
The patient had a multidrug-resistant Streptococcus pneumoniae infection resistant to ceftriaxone, azithromycin, and levofloxacin.
Despite appropriate antibiotic treatment, the patient's condition rapidly deteriorated to multi-organ failure and death.
The case emphasizes the role of vaccination in preventing severe infections in intravenous drug users.
Abstract
This case report presents Streptococcus pneumoniae bacteremia in a 60-year-old male with a history of intravenous drug use (IDU), presenting with acute respiratory distress syndrome (ARDS). The patient experienced fever, malaise and myalgia for about a week. Chest imaging revealed diffuse bilateral infiltrates, and laboratory tests showed elevated inflammatory markers. His condition deteriorated abruptly, rapidly progressing to respiratory failure, shock, and ultimately death. Both sputum and blood cultures confirmed Streptococcus pneumoniae infection and revealed resistance to commonly used antibiotics, including ceftriaxone, azithromycin, and levofloxacin. Despite appropriate antibiotic therapy, the infection could not be controlled, and the patient’s condition deteriorated rapidly; he died on the fifth day of hospitalization due to multi-organ failure. The case underscores the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
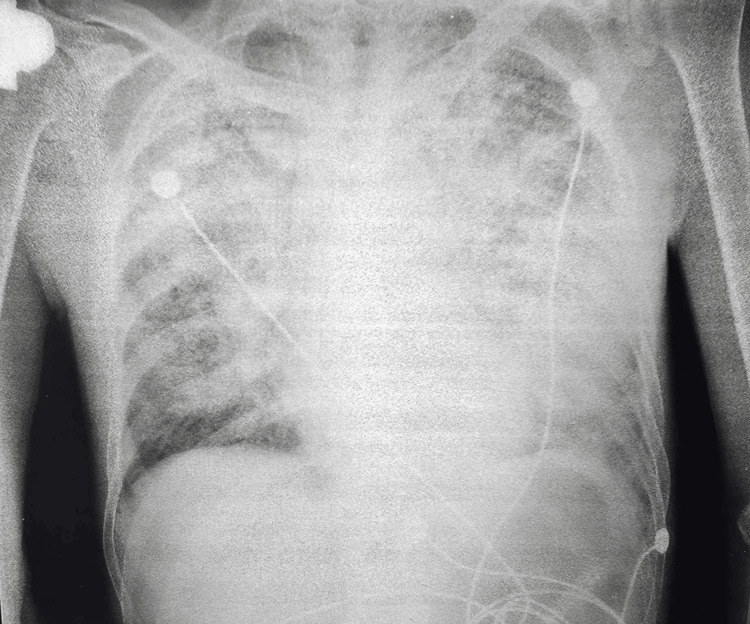 Figure 1
Figure 1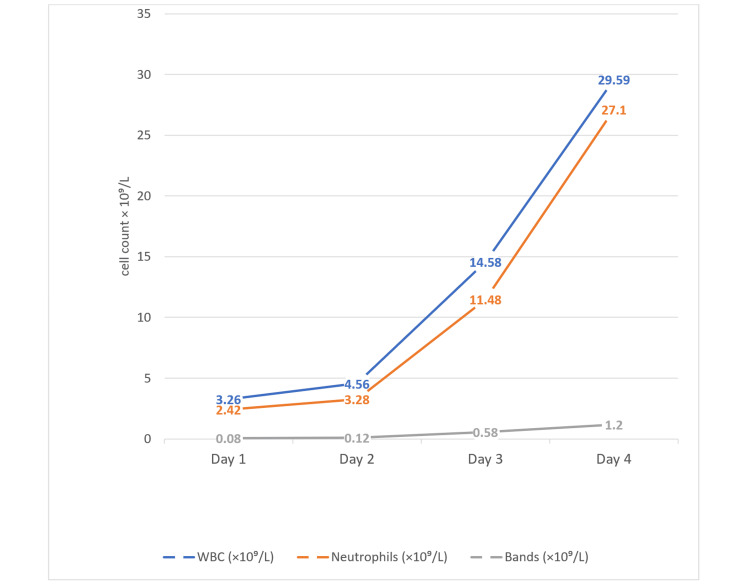 Figure 2
Figure 2| Day | SPO₂ (%) | Blood Pressure (mmHg) | Temperature (°C) | Ventilation |
| 1 | 85-88 | 142/82 | 37.5 | NIV/CPAP |
| 2 | 75 | 130/80 | 38 | P-SIMV |
| 3 | 80 | 115/75 | 39.2 | P-SIMV |
| 4 | 88 | 90/53 | 39.8 | P-SIMV |
| 5 | 75 | 85/50 | 40 | P-SIMV |
| Laboratory Parameter | Value | Reference Range |
| WBC (×10⁹/L) | 3.26 | 4.0–11.0 |
| Neu (×10⁹/L) | 2.42 | 2.0-7.0 |
| Lymph (×10⁹/L) | 0.76 | 1-5 |
| Bands (×10⁹/L) | 0.08 | 0.01-0.2 |
| CRP (mg/L) | >200 | <5 |
| CREA (µmol/L) | 62 | 54.00–104.00 |
| Antibiotic | Susceptibility |
| Piperacillin-tazobactam | Sensitive |
| Imipenem | Sensitive |
| Meropenem | Sensitive |
| Vancomycin | Sensitive |
| Cotrimoxazole | Sensitive |
| Oxacillin | Sensitive |
| Linezolid | Sensitive |
| Teicoplanin | Sensitive |
| Ceftriaxone | Resistant |
| Levofloxacin | Resistant |
| Moxifloxacin | Resistant |
| Azithromycin | Resistant |
| Clindamycin | Resistant |
| Tetracycline | Resistant |
| Laboratory Parameter | Value | Reference Range |
| WBC (×10⁹/L) | 29.59 | 4.0–11.0 |
| Neu (×10⁹/L) | 27.1 | 2.0-7.0 |
| Lymph (×10⁹/L) | 2.04 | 1-5 |
| Bands (×10⁹/L) | 1.2 | 0.01-0.2 |
| CRP (mg/L) | >200 | <5 |
| CREA (µmol/L) | 418 | 54.00–104.00 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPneumonia and Respiratory Infections · Antibiotics Pharmacokinetics and Efficacy · Nosocomial Infections in ICU
Introduction
Sepsis is a life-threatening condition that occurs when the body’s response to infection triggers widespread inflammation, leading to tissue damage, organ failure, and potentially death. It remains one of the leading causes of hospital morbidity and mortality worldwide, with the United States alone reporting approximately 1.7 million cases annually, resulting in approximately 350,000 deaths each year [1]. Sepsis is particularly dangerous in populations with underlying risk factors, such as intravenous drug use (IDU), which increases susceptibility to bacteremia, endocarditis, and other infectious diseases, often causing or contributing to the development of sepsis.
One of the primary causes of sepsis-related acute respiratory distress syndrome (ARDS) is pneumonia, with Streptococcus pneumoniae (pneumococcus) being the leading pathogen responsible for community-acquired pneumonia. Pneumococcal pneumonia can result in significant morbidity, and sepsis-associated ARDS carries a mortality rate of 30-40% [2].
A major global health concern is the increasing antibiotic resistance in Streptococcus pneumoniae, particularly against commonly used β-lactams and macrolides. This resistance is fueled by the overuse and misuse of antibiotics. The horizontal transmission of antibiotic resistance genes further complicates the clinical management of these infections [3].
Vaccination against *S. pneumoniae *is a preventive measure that can significantly reduce the incidence and severity of these infections. Currently, pneumococcal conjugate vaccines (PCVs), such as PCV13, PCV15, and PCV20, along with the Pneumococcal polysaccharide vaccine (PPSV23), are key strategies for prevention. Pneumococcal vaccination is recommended for infants and young children, adults aged 50 years or older, and individuals with specific risk factors such as chronic medical conditions, asplenia, and immunocompromised states [4].
This case underscores the critical importance of pneumococcal vaccination in high-risk groups, including individuals with a history of intravenous drug use. Moreover, the early symptoms of infections, particularly in this risk group, can often be nonspecific and unclear, which complicates timely diagnosis and intervention. The patient presented with a severe Streptococcus pneumoniae infection, which was resistant to commonly used antibiotics such as ceftriaxone and azithromycin, highlighting the growing challenge of treating pneumococcal infections. Despite sensitivity, there was no response to piperacillin-tazobactam and vancomycin, further complicating the treatment approach.
Case presentation
A 60-year-old male with a history of heavy alcohol and intravenous drug use, but no other known chronic medical conditions, was admitted to the emergency department with fever, myalgia, and malaise lasting for about a week. However, in the 24 hours prior to admission, his condition rapidly worsened, resulting in respiratory failure, which ultimately required hospitalization. Upon admission, the patient was tachypneic (respiratory rate 36 breaths per minute), with a blood pressure of 142/82 mmHg, heart rate of 144 beats per minute, and a temperature of 37.5°C. He appeared cyanotic with an oxygen saturation (SPO₂) of 41%, which improved to 85-88% on high-flow oxygen and non-invasive ventilation (NIV/CPAP) (Table 1).
On auscultation, the patient exhibited decreased breath sounds, fine crackles, and wheezing diffusely across both lungs. His clinical condition rapidly deteriorated, requiring orotracheal intubation and mechanical ventilation.
The initial laboratory investigations were significant for a slightly decreased white blood cell count and elevated C-reactive protein (Table 2).
Chest X-ray findings showed a significant decrease in lung aeration with confluent bilateral infiltrates affecting both lung fields, more pronounced on the left side, suggesting pneumonia with ARDS (Figure 1). The partial pressure of oxygen in arterial blood/fraction of inspired oxygen (P/F) ratio of 65 indicated severe impairment in oxygenation, consistent with severe ARDS. Echocardiography revealed moderate mitral valve regurgitation (+2/4), mild pulmonary hypertension, with a pulmonary artery systolic pressure (PASP) of 46 mmHg (normal range: 15-30 mmHg) and no vegetations were detected.
Chest X-ray findings: Significant reduction in lung aeration with extensive diffuse bilateral infiltrates involving both lung fields, more pronounced on the left side
Empirical antibiotic therapy with piperacillin-tazobactam and vancomycin, along with supportive care, was initiated. On day three of admission, blood and sputum cultures identified Streptococcus pneumoniae, which showed the same antibiotic susceptibility pattern in both samples (Table 3). Based on the antibiotic susceptibility profile, meropenem was added to the antibiotic therapy regimen.
Despite aggressive management, the patient's condition deteriorated on day four (Table 1), with a Glasgow Coma Scale of 4, and he remained hypoxic despite maximal mechanical ventilation. Laboratory findings showed significant decline, including creatinine level of 418.5 µmol/L (Table 4) and prominent neutrophilia with elevated bands (Figure 2). On day five, he died due to multi-organ failure resulting from septic shock.
Dynamics of white blood cell count, neutrophil count, and bands from admission to day four of hospitalization, exhibiting sudden escalating leukocytosisWBC: White Blood Cell
Discussion
This case describes a 60-year-old male with a history of IDU, who initially presented with sepsis and ARDS. Despite the use of appropriate empirical antibiotics and intensive care, the patient ultimately experienced multi-organ failure and died on the fifth day of admission.
One of the main factors contributing to the patient's rapid deterioration was the delayed admission. The patient reported symptoms for a week before seeking medical care, during which the infection likely progressed significantly. The positive sputum and blood cultures identified Streptococcus pneumoniae. While intravenous drug use raised concerns for a bloodstream infection, there were no signs of injection site infection or pneumococcal endocarditis (PE), which is rare, accounting for less than 3% of infective endocarditis cases [5]. Instead, the chest X-ray revealed bilateral diffuse infiltrates, more pronounced on the left side (Figure 1), suggesting pneumonia complicated by sepsis and ARDS. The identification of the same bacterium in both sputum and blood cultures, along with identical antibiotic susceptibility patterns, confirms this route of infection.
Heavy alcohol and intravenous drug use may have contributed to aspiration pneumonia, as altered consciousness in these patients can lead to aspiration of oropharyngeal flora. While aspiration was once thought to primarily involve oral anaerobes, both community- and hospital-acquired pneumonias are now recognized to result from aspiration of virulent pathogens, including S. pneumoniae [6]. Pneumonia should always be suspected in ARDS with sepsis, even in the absence of strong radiographic evidence, as the airspace opacities caused by ARDS on the chest X-ray can obscure the presence of associated pneumonia [7].
Another key concern highlighted by this case was the antibiotic resistance profile of the isolated Streptococcus pneumoniae strain. In the Intensive Care Unit, pneumonia is commonly treated empirically with a beta-lactam plus a macrolide [8]. The organism showed resistance to several commonly used antibiotics, including ceftriaxone, azithromycin, levofloxacin and moxifloxacin (Table 3). This resistance profile is concerning, particularly in the context of IDU, where frequent or inappropriate antibiotic use can increase the risk of developing resistant infections.
Although piperacillin-tazobactam and vancomycin were included in the initial treatment regimen, they did not yield a positive effect, as the infection process severely progressed. Considering the challenges of antibiotic resistance and the progression dynamics, vaccination against S. pneumoniae becomes increasingly important. Pneumococcal vaccination (PCVs and PPSV23) should be prioritized in IDUs, along with other recommended immunizations such as hepatitis A, hepatitis B, influenza, COVID-19, and Tdap, due to often incomplete or unknown immunization histories in this population. Prioritizing vaccination programs for IDUs can help reduce the incidence of severe infections and limit the need for antibiotics.
Conclusions
This case report highlights the critical challenges in managing treatment-resistant fulminant septic shock caused by Streptococcus pneumoniae in an unvaccinated IDU. This case underscores the alarming reality of the growing issue of multidrug resistance, which can significantly impair treatment effectiveness and contribute to poor outcomes. Rapid deterioration despite appropriate therapy highlights the need for primary prevention strategies. Therefore, this case reinforces the critical importance of vaccination as an essential measure to reduce the burden of severe pneumococcal infections, minimizing the need for intensive, and sometimes ineffective, antibiotic treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1About Sepsis 3 2025 2024 https://www.cdc.gov/sepsis/about/index.html
- 2Attributable mortality of ARDS among critically ill patients with sepsis: a multicenter, retrospective cohort study BMC Pulm Med Wang DH Jia HM Zheng X Xi XM Zheng Y Li WX 110242024 https://bmcpulmmed.biomedcentral.com/articles/10.1186/s 12890-024-02913-13843884910.1186/s 12890-024-02913-1PMC 10913263 · doi ↗ · pubmed ↗
- 3Antimicrobial resistance among Streptococcus pneumoniae Antimicrobial Resistance in the 21st Century Cillóniz C Garcia-Vidal C Ceccato A Torres A 1338 Cham Springer 2018
- 4Pneumococcal Vaccination 3 2025 2024 https://www.cdc.gov/pneumococcal/vaccines/index.html
- 5Infective endocarditis caused by Streptococcus pneumoniae from sinusitis: a case report J Cardiol Cases Yamazaki K Miura T Sunohara D 2792812520223558206810.1016/j.jccase.2021.11.003PMC 9091493 · doi ↗ · pubmed ↗
- 6Aspiration Pneumonitis and Pneumonia 3 2025 2024 https://emedicine.medscape.com/article/296198-overview#a 1?form=fpf
- 7Overview of current lung imaging in acute respiratory distress syndrome Eur Respir Rev Zompatori M Ciccarese F Fasano L 519530232014 https://publications.ersnet.org/content/errev/23/134/5192544595110.1183/09059180.00001314 PMC 9487404 · doi ↗ · pubmed ↗
- 8ERS/ESICM/ESCMID/ALAT guidelines for the management of severe community-acquired pneumonia Eur Respir J Martin-Loeches I Torres A Nagavci B 612023 https://publications.ersnet.org/content/erj/61/4/220073510.1183/13993003.00735-202237012080 · doi ↗ · pubmed ↗