Overnight Fasting and Body Weight: Emulated Target Trial Using Cancer Prevention Study-3 Data
Valeria Elahy, Ying Wang, W. Dana Flanders, Charlie Zhong, Marjorie L. McCullough

TL;DR
This study used data from a cancer prevention study to examine how different fasting periods overnight and around sleep affect body weight over two years.
Contribution
The study provides sex-specific insights into the effects of overnight fasting on body weight using a novel emulated target trial approach.
Findings
Overnight fasting ≥12 hours showed a higher weight in men but lower weight in women.
Fasting ≥4 hours before sleep was associated with a 1.9 kg lower weight compared to <4 hours.
Overall, overnight fasting alone may not significantly influence body weight.
Abstract
Background/Objectives: Intermittent fasting has gained attention in managing weight, yet its long-term effects remain unclear. We examined the impact of overnight, before-sleep, and after-sleep fasting on body weight over two years using data from the Cancer Prevention Study-3 Diet Assessment Substudy. Methods: We emulated three target trials in 457 adults without diabetes or cancer. Participants were assigned to fasting strategies of <12 vs. ≥12 h overnight, <4 vs. ≥4 h before sleep, and <1 vs. ≥1 h after sleep at baseline (2016). Mean body weight 2 years post baseline was estimated using marginal structural models with stabilized inverse probability weights, adjusting for pre-baseline covariates. Results: After two years (median [IQR]: 2.0 [1.8–2.0] years), the estimated mean body weight was 79.4 kg (≥12 h overnight) vs. 78.9 kg (<12 h overnight) (mean difference: 0.4 kg; 95% CI: −4.1…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
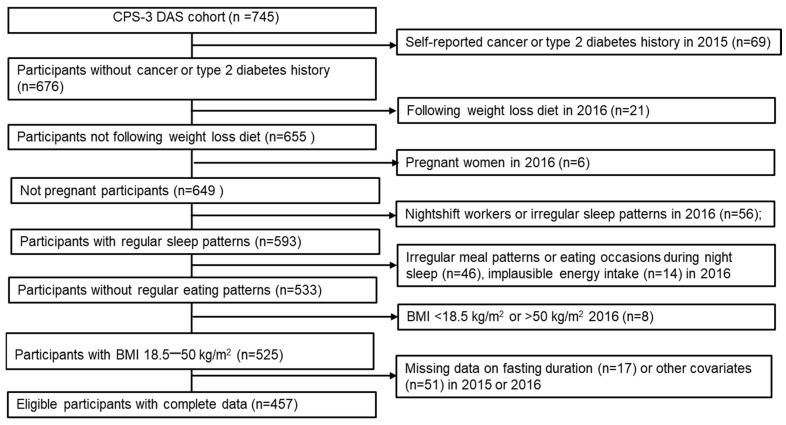 Figure 1
Figure 1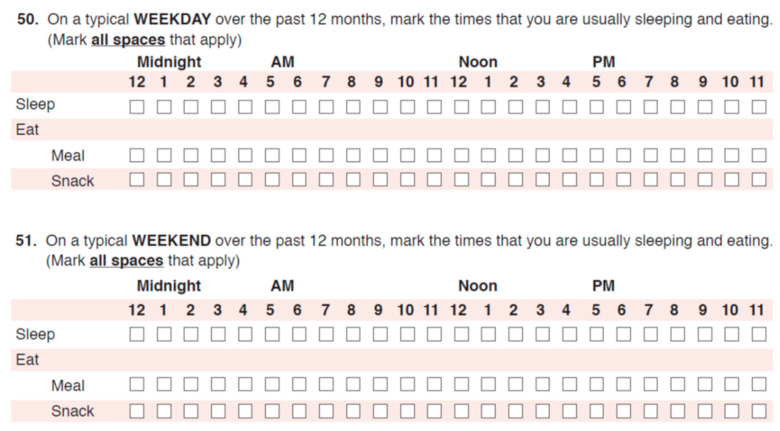 Figure 2
Figure 2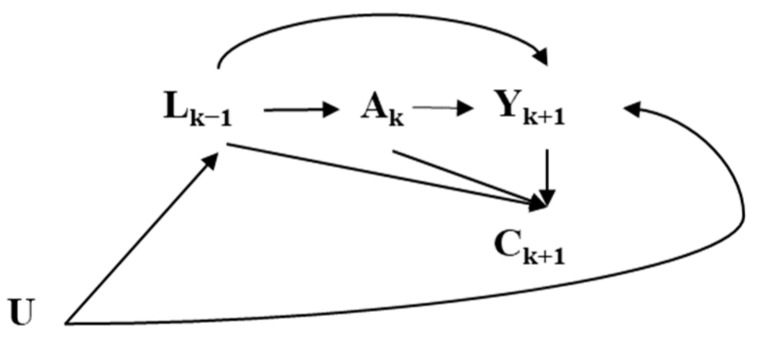 Figure 3
Figure 3- —American Cancer Society
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDietary Effects on Health · Diet and metabolism studies · Circadian rhythm and melatonin
1. Introduction
Intermittent fasting has gained considerable attention as a dietary strategy for managing body weight and metabolic health. Data from the 2015–2016 NHANES show that over half of Americans fast for at least 12 h overnight [1]. Despite this, obesity rates continue to rise, with one in five adults in every state living with obesity in 2023 [2,3].
While numerous randomized trials have investigated the effect of time-restricted eating (TRE), a specific form of intermittent fasting, on body weight, results remain inconsistent, highlighting several key limitations in current evidence [4,5,6]. Most trials target specific populations, such as athletes or individuals with metabolic conditions, with typically small sample sizes (16–174 participants) and limited durations (none exceeding 12 months) [5,7,8,9]. Additionally, these trials primarily focus on late TRE, leaving early TRE largely unexplored despite its potential for greater metabolic benefits [10]. This underscores the need for larger, longer-term randomized trials in diverse populations to evaluate the effects of fasting on body weight, which are not feasible [4].
To address these gaps, we emulated a target trial, leveraging data from 457 participants in the prospective Cancer Prevention Study-3 Diet Assessment Substudy (CPS-3 DAS). An emulated target trial is an analysis of observational data that can be viewed as an attempt to mimic a hypothetical pragmatic randomized trial to answer a causal question [11]. Several studies have successfully applied this framework to evaluate the effects of lifestyle exposures [12], including dietary ones [13,14], on mortality and chronic disease outcomes, demonstrating that, when properly implemented, effect estimates from an emulated target trial closely align with the results from an actual RCT [15]. In this study, we examined the effect of overnight fasting (<12 h vs. ≥12 h), before-sleep fasting (<4 h vs. ≥4 h), and after-sleep fasting (<1 h vs. ≥1 h) on body weight two years after treatment assignment. To emulate randomization and ensure exchangeability, we apply marginal structural models (MSMs) with inverse probability weighting (IPW), controlling for baseline and pre-baseline confounders [16]. By assuming positivity and consistency, we aim to estimate causal effects, closely mimicking the conditions of a randomized trial [17].
2. Materials and Methods
A target trial is a pragmatic, hypothetical, randomized controlled trial that we would like to conduct to answer a causal question of interest [11,18]. We designed this observational analysis as an attempt to emulate three target trials of overnight fasting strategies and body weight. Target trial emulation has two steps: (1) target trial specification (setting up of the study protocol, outcome definition, and causal contrasts; (2) emulation of the components of the target trial protocol using observational data.
2.1. Target Trial
The key protocol components of this target trial are outlined in Table 1 (left column). Eligibility criteria for all three trials include adults without a history of cancer or type 2 diabetes who are not following weight-loss diets at baseline. We would exclude pregnant women [19] (due to their special nutritional needs and pregnancy-related body weight and metabolic changes), night shift workers [20] (irregular sleep patterns and eating times among night shift workers can significantly impact their metabolic health, making it challenging to isolate the effects of fasting interventions), and those with irregular sleep patterns (night sleep <4 or >14 h, starting night sleep after 5:00 a.m. or before 5:00 p.m.), irregular eating patterns (≤1 or >8 meals/day or eating during night sleep), implausible energy intake (<800 or >4200 kcal/day for men and <500 or >3500 kcal/day for women), or extreme body mass index (<18.5 kg/m^2^ or >50 kg/m^2^).
Three independent target trials would assess the effect of the following fasting strategies of interest:
Overnight fasting trial: <12 h vs. ≥12 h;Before-sleep fasting trial: <4 h vs. ≥4 h;After-sleep fasting trial: <1 h vs. ≥1 h.
Each trial independently assesses the effects of overnight, before-sleep, and after-sleep fasting interventions on body weight [11].
These fasting intervention cutoff points were chosen based on several considerations. The ≥12 h overnight fasting duration aligns with common practices in intermittent fasting protocols and is often recommended for metabolic health benefits [21]. Several studies and reviews have shown that a 12-h fasting period aligns with common intermittent fasting protocols and offers potential metabolic health benefits and minimal negative outcomes [22]. The ≥4 h before-sleep fasting duration cutoff was selected to investigate the effects of avoiding food intake close to bedtime, based on studies showing that late-night eating is linked to poorer metabolic outcomes [23,24]. The ≥1 h after-sleep fasting duration was chosen to explore the potential impact of delaying the first meal of the day on weight management. These chosen cutoff points represent practical and achievable fasting durations for the general population, promoting adherence and real-world applicability. Time-restricted eating schedules like 12:12 and 16:8 are popular and considered flexible, making them suitable for various lifestyles and ensuring that fasting durations can be easily integrated into daily routines [25]. In addition, these cut-off points were the closest to the mean durations in the CPS-3 cohort eligible for this emulated trial.
Participants would be randomly assigned to longer or shorter strategies of each intervention and asked to follow them for two years. Follow-up would be from intervention assignment until death, loss to follow-up, or administrative end of follow-up two years after the treatment assignment. The primary outcome of interest would be the body weight self-reported two years after the assignment of treatment strategies, aiming to assess the intention-to-treat effects of intervention by comparing shorter to more extended fasting strategies for each intervention.
2.2. Target Trial Emulation Using Observational Data
We emulated the above target trial using observational prospective CPS-3 DAS data.
Between 2006 and 2013, the CPS-3 study enrolled over 300,000 adults across 36 states, Puerto Rico, and the District of Columbia to study cancer risk factors, focusing on lifestyle, genetic, and environmental influences [26]. The CPS-3 DAS, specifically designed to validate the cohort’s modified Food Frequency Questionnaire (FFQ), enrolled 866 participants and collected data on meal and sleep timing, diet, physical activity, alcohol consumption, and body weight in 2015 and 2016 [27,28]. Diet quality, energy intake, and alcohol consumption were ascertained from the FFQ data in 2015 and 2016 using the 2015 Healthy Eating Index score to assess diet quality [21]. Participants’ weight was self-reported in 2015, 2016, and 2018 [26], with self-reported measurements previously validated against in-person measurements in CPS-3 [29]. The 2015 and 2018 surveys collected demographic, behavioral, medical history, and anthropometric data [30].
In CPS-3 DAS, overnight, before-sleep, and after-sleep fasting durations were assessed using a validated CPS-3 24-h meal and sleep timing grid in 2015 and 2016 (Figure A1) [21]. Participants were asked: “On a typical weekday over the past 12 months, mark the times that you are usually sleeping and eating (Mark all spaces that apply)” and “On a typical weekend over the past 12 months, mark the times that you are usually sleeping and eating (Mark all spaces that apply)”. Separate rows corresponded to each hour from 12 midnight to 11 pm, and an eating occasion was defined as any instance of food intake, including meals or snacks. This grid was validated against up to six 24-h dietary recalls over a one-year period. As measured by sensitivity and specificity, the area under the receiver operating characteristic curve (AUC) for overnight fasting ≥12 h was 0.744 for weekdays and 0.718 for weekends; for ≥14 h fasting, AUCs were 0.776 and 0.640, respectively. Spearman correlations per hour of overnight fasting were 0.51 (95% CI: 0.45–0.56) for weekdays and 0.39 (95% CI: 0.31–0.46) for weekends [21].
Overnight fasting was defined as the longest interval of no eating surrounding the longest sleep period. For each grid (weekday and weekend), we calculated the time from the end of the last marked eating occasion before the onset of the longest sleeping period to the start of the first marked eating occasion after that sleep [31]. We used the end of the hour box for the last eating occasion and the start of the hour box for the first eating occasion when computing this interval. Before- and after-sleep fasting were each calculated per grid and then averaged over the week. For each grid (weekday and weekend), before-sleep fasting was defined as the interval from the end of the last eating occasion (end of that hour block) to the beginning of the longest sleep period, and after-sleep fasting as the interval from the end of the longest sleep period to the start of the first eating occasion the next day (start of that hour block). We computed a weighted 7-day average fasting duration as (5 × weekday + 2 × weekend)/7 and used this value to assign participants to <12 h or ≥12 h of overnight fasting, <4 h or ≥4 h of before-sleep fasting, and <1 h or ≥1 h for after-sleep fasting.
2.3. Modifications to the Target Trial Protocol
Several modifications had to be applied to the target trials to align these emulated trials with the CPS-3 DAS data (Table 1, right column).
Because meal and sleep timings were only assessed in 2015 and 2016, inquiring about the participants’ habits in the past 12 months before the assessments and not about their intended fasting durations, we assumed that the meal and sleep timing grid accurately represented both the average and the intended fasting durations for the following year. We used 2016 as the baseline, with adjustments made for fasting durations reported in 2015 as pre-baseline fasting exposure to emulate randomized treatment assignments.
We identified individuals who met all eligibility criteria for the target trial and excluded participants with missing baseline and pre-baseline fasting duration or other covariates. Eligible individuals were followed from their DAS 2016 questionnaire return to their CPS-3 2018 questionnaire return with a mean follow-up duration of 704.7 ± 82.8 days. Participants were censored (n = 29) if they did not participate in the CPS-3 2018 survey (n = 15), if they reported shiftwork in the 2018 survey (n = 12), or were pregnant (n = 2) in 2018.
Third, to emulate random assignment to fasting strategies and ensure exchangeability, we used stabilized inverse probability weighing, which estimates the probability of fasting strategies given pre-baseline confounders such as age, sex, race, education, income, employment status, diet quality, alcohol consumption, sleep duration, BMI, and pre-baseline exposure. We used direct acyclic graphs to visually present the assumed causal relationship among those confounders, treatment, censoring, and body weight. (Figure A2) [32]. Under the assumption that the measured covariates are sufficient to adjust for both confounding and selection bias due to loss to follow-up, this simulates the conditions of a randomized controlled trial, where treatment assignment is independent of confounders [16,33].
2.4. Statistical Analyses
The observational analog of the per-protocol effect in the target trials was estimated using marginal structural models with stabilized inverse probability weights by creating a pseudo-population where the distribution of confounders is balanced across different treatment groups [16]. For each individual, a weight was calculated based on the inverse probability of receiving the treatment they actually received, adjusting for pre-baseline confounders (race, sex, education, age, work status, income, BMI, diet quality, alcohol intake, pre-baseline overnight fasting duration [for overnight treatment], before-sleep fasting duration [for before-sleep treatment], pre-baseline after-sleep fasting duration, and baseline sleep duration [for after-sleep treatment]). To address censoring, we estimated stabilized inverse probability weights for censoring using a method similar to that used for treatment weights. The censoring weights were calculated as the ratio of the probability of remaining uncensored given the treatment assignment to the probability of remaining uncensored given both treatment and covariates [16,34]. The product of stabilized treatment and censoring weights was truncated at the 99th percentile to reduce the influence of extreme values. Differences between the mean body weight under each fasting duration were estimated using the shortest fasting duration as the reference within each intervention group. Then, 95% confidence intervals (CIs) were calculated using nonparametric bootstrapping with 500 samples.
To understand how different subgroups respond to interventions, we performed stratified analyses by sex [35], BMI [36] (<25 kg/m^2^ and ≥25 kg/m^2^), and the midpoint of sleep [37] (before and after the sample median).
In our analysis, we excluded 51 participants with missing data (income [n = 5], education [n = 16], work status [n = 14], diet quality [n = 14]). To assess the impact of excluding participants with missing covariates, we (1) performed multiple imputations of missing covariate values and undertook the sensitivity analysis to evaluate the potential bias introduced by excluding participants with missing data [38]. (2) To mitigate the influence of outliers, we truncated treatment weights at the 99th percentile. We performed the analysis without truncation to understand how extreme weights affect the estimates. (3) We assessed whether sex modifies the relationship between diet quality, fasting duration, and body weight by introducing the interaction term between sex and diet quality in estimating treatment weights [39]. To explore the potential impact of physical activity on individual fasting duration habits [40], (4) we further adjusted our estimates for physical activity. We (5) further adjusted for the other fasting intervals in the before- and after-sleep fasting models. Finally, (6) we adjusted for the number of meals and snacks to account for missed eating occasions if participants had longer fasting durations.
All analyses were performed using SAS 9.4 software (SAS Institute, Inc., Cary, NC, USA).
The study protocol was approved by the institutional review boards of Emory University.
3. Results
3.1. Study Population
In the CPS-3 DAS cohort, 457 participants were eligible for the target trial emulation (Figure 1). The mean age of the participants was 51.2 years, with 35.4% being male, 22.2% Black, 14.5% Hispanic, and 63.3% White (Table 2). Most participants had a college degree or higher (79.2%), and the mean BMI was 27.1 kg/m^2^. At baseline, 57.5% reported <12 h of overnight fasting, 58.2% reported <4 h of before-sleep fasting, and 54.9% reported <1 h of after-sleep fasting. The mean baseline body weight was 78.3 kg.
3.2. Emulated Target Trial Estimates
After two years (median [IQR]: 2.0 [1.8–2.0] years), the estimated mean body weight under overnight fasting for the ≥12 h strategy was 79.4 kg, compared with 78.9 kg under <12 h (mean difference: 0.4 kg; 95% CI: −4.1 to 4.7) (Table 3). For before-sleep fasting, under the ≥4 h strategy, estimated weight was 79.4 kg vs. 77.5 kg under <4 h (mean difference: 1.9 kg; 95% CI: −0.4 to 4.1). For after-sleep fasting, under the ≥1 h strategy, the mean weight was 79.8 kg vs. 78.9 kg under the <1 h strategy (mean difference: 0.9 kg; 95% CI: −4.3 to 4.4).
3.3. Subgroup Analyses
Subgroup analyses stratified by sex, sleep midpoint, and BMI are summarized in Table 4. Among men, under the overnight ≥12 h strategy, weight was 100.9 kg vs. 83.9 kg under the <12 h strategy (mean difference: 17.0 kg; 95% CI: 10.8, 23.1). Among women, under the overnight ≥12 h strategy, weight was 74.3 kg vs. 77.1 kg under the <12 h strategy (mean difference: −2.8 kg; 95% CI: −6.8, 1.2). For participants with an earlier sleep midpoint (before 3:17 a.m.), overnight fasting (≥12 h) resulted in an estimated mean weight of 78.5 kg vs. 79.0 kg for <12 h (mean difference: −0.5 kg; 95% CI: −5.2, 4.2). In those with a later sleep midpoint (3:17 a.m. or later), mean weights were similar between fasting durations (80.8 kg for ≥12 h vs. 80.6 kg for <12 h; mean difference: 0.2 kg; 95% CI: −5.0, 5.5). Among participants with BMI <25 kg/m^2^, overnight fasting (≥12 h) resulted in an estimated mean weight of 66.5 kg vs. 65.7 kg for <12 h (mean difference: 0.8 kg; 95% CI: −2.3, 3.8). Among those with BMI ≥25 kg/m^2^, the estimated mean weight was 88.2 kg for ≥12 h vs. 89.8 kg for <12 h (mean difference: −1.6 kg; 95% CI: −6.0, 2.8). Similar small and non-significant differences were observed for before-sleep and after-sleep fasting strategies across all subgroups. Stratification by pre-baseline fasting exposure showed minimal differences in estimated mean body weight across fasting strategies (Table A1).
3.4. Sensitivity Analysis
The sensitivity analysis (Table A2) suggested that the estimates from the primary analysis (excluding participants with missing data) were consistent with those obtained from the imputed datasets, suggesting that excluding participants with the missing data had minimal effect on the estimates [41]. The truncation of the extreme weights did not impact the estimates. The mean inverse probability weights were 1.1 ± 0.1 before truncation and 1.0 + 0.1 after the truncation at the 99th percentile. Including an interaction term between sex and diet quality as well as further adjustment for physical activity, other fasting duration, and number of eating occasions had no major effect on the estimates.
4. Discussion
This study prospectively examines the effects of various fasting periods, particularly overnight fasting, before-sleep fasting, and after-sleep fasting, on body weight in a modern multiethnic CPS-3 DAS cohort. While we found little indication that the longer overnight fasting (≥12 h) strategy substantially influences the body weight in this population, we detected some differences by sex, suggesting that, compared to shorter overnight fasting (<12 h), longer overnight fasting may be linked to higher weight in men but has no effect in women. We did not detect differences in body weight linked to longer before- (≥4 h) or after-sleep (≥1 h) fasting.
Interestingly, among men assigned to the ≥12 h overnight fasting strategy, estimated body weight was higher than in those with shorter fasting. One plausible mechanism is hormone-mediated: fasting has been shown to lower circulating testosterone in men, which in turn can reduce lean mass and basal metabolic rate and thereby predispose to weight gain over time [42]. For example, earlier studies reported significant declines in testosterone following a time-restricted eating protocol [22], and low androgen levels were associated with adverse shifts in body composition [43,44]. Moreover, a trial of prolonged fasting in healthy young adults found that females, but not males, experienced lower body weight and improved body composition under extended fasting [45]. Together, these findings support that prolonged overnight fasting may differentially impact men’s metabolic health and body weight, and further investigation of the gender-related difference in the effect of fasting is needed.
Our results align with previous research that has shown mixed findings regarding the effectiveness of intermittent fasting for weight management [46,47,48]. For instance, a 12-week randomized weight-loss trial in individuals with overweight and obesity demonstrated no significant difference in weight loss among participants eating from 12:00 p.m. to 8:00 p.m. compared to a control group who was instructed to eat three meals per day at any time [46]. Another 12-week intervention on 19 participants with metabolic syndrome found that 10 h of time-restricted eating (14 h of overnight fasting) promoted weight loss and helped to reduce waist circumference and body fat [47]. Our null findings for extended before-sleep and after-sleep fasting mirror mixed evidence from studies of early dinner and delayed breakfast. A five-week crossover trial with 11 participants found that early time-restricted eating, where participants consumed all meals between 8:00 a.m. and 2:00 p.m., improved insulin sensitivity and appetite regulation more than a delayed eating schedule (eating between 12:00 p.m. and 8:00 p.m.) but did not necessarily lead to weight loss [49]. Another randomized trial of TRE found that early TRE (8-h eating window between 7:00 a.m. and 3:00 p.m.) may be more effective for weight loss but not for improving body fat composition or other metabolic factors, compared to eating anytime during a self-selected ≥12-h window [50]. Together, these findings suggest that isolated shifts in the timing of the last or first meal may not substantially influence body weight without changes in total energy intake, meal composition, or circadian factors.
One of the strengths of our study is the use of an emulated target trial design with explicitly defined treatment strategies and stabilized inverse probability weighting, allowing for a rigorous comparison of different fasting strategies using observational data [51]. The large, diverse cohort from the CPS-3 DAS provides a robust sample larger than most randomized trials. We also assessed the effect of intervention in participants who did not self-report prolonged fasting before baseline for at least 12 months, allowing for reducing the prevalent user bias and ensuring a more accurate comparison between different fasting strategies [52].
There are several limitations to acknowledge. First, self-reported data on fasting durations and body weight may be subject to recall bias and measurement error. The self-reported body weight was validated against in-person measurements from previous studies, ensuring reliability [26]. Similarly, meal timing and sleep grid were shown to be reliable tools for the assessment of fasting duration [21]. Second, our study design assumes that fasting habits remained consistent over the follow-up, which may not accurately reflect participants’ actual behavior and may not allow us to distinguish between per-protocol and intention-to-treat effects. While more frequent, repeated data collection could enhance this study’s strengths; the reported data from the meal timing grid was confirmed to have a relatively high one-year reproducibility with ρ = 0.62, suggesting that it is reasonable to believe that most of the participants sustained their reported fasting durations for 12 months before the end of follow-up [21]. While we excluded the participants with diabetes and cancer from the analytic cohort, our analysis did not account for the change in diabetes status or other comorbidities during the follow-up. Although we adjusted for a comprehensive list of confounders, the emulated target trial relies on several assumptions and is unable to eliminate uncontrolled confounding of the variables not assessed in the CPS-3 cohort. To assess the effect of the analytic decision made in our study, we conducted an extensive sensitivity analysis, which produced results similar to those of our primary analysis. Although we have adjusted each IPW model for the other fasting intervals, and we found no correlation between baseline before and after-sleep fasting durations (Spearman ρ = –0.06), our ability to disentangle the independent effects of before- and after-sleep fasting durations may still be limited. Finally, although social jetlag [53] (the mismatch between sleep timing on workdays and weekends) may influence both fasting timing and body weight, our meal-and-sleep grid lacked the day-to-day resolution to quantify a valid social-jetlag metric, and our sample size is likely insufficient to robustly assess its confounding effect in IPW models.
5. Conclusions
In conclusion, our findings suggest that longer overnight fasting alone may not substantially influence body weight, but sex-specific differences need to be further investigated. Larger future studies and stronger methods to longitudinally document behavior in real time are needed to investigate the joint effect of overnight fasting and other dietary and behavioral factors, like physical activity and energy intake, on body weight.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wirth M.D. Zhao L. Turner-Mcgrievy G.M. Ortaglia A. Associations between fasting duration, timing of first and last meal, and cardiometabolic endpoints in the national health and nutrition examination survey Nutrients 202113268610.3390/nu 1308268634444846 PMC 8397975 · doi ↗ · pubmed ↗
- 2Centers for Disease Control and Prevention (CDC) Adult Obesity Prevalence Maps U.S. Dept of Health and Human Services Washington, DC, USA 2023
- 3Jakicic J.M. Powell K.E. Campbell W.W. Dipietro L. Pate R.R. Pescatello L.S. Collins K.A. Bloodgood B. Piercy K.L. Physical activity and the prevention of weight gain in adults: A systematic review Med. Sci. Sports Exerc.2019511262126910.1249/MSS.000000000000193831095083 PMC 6527311 · doi ↗ · pubmed ↗
- 4Cienfuegos S. Gabel K. Kalam F. Ezpeleta M. Wiseman E. Pavlou V. Lin S. Oliveira M.L. Varady K.A. Effects of 4-and 6-h time-restricted feeding on weight and cardiometabolic health: A randomized controlled trial in adults with obesity Cell Metab.202032366378.e 310.1016/j.cmet.2020.06.01832673591 PMC 9407646 · doi ↗ · pubmed ↗
- 5Tinsley G.M. Moore M.L. Graybeal A.J. Paoli A. Kim Y. Gonzales J.U. Harry J.R. Van Dusseldorp T.A. Kennedy D.N. Cruz M.R. Time-restricted feeding plus resistance training in active females: A randomized trial Am. J. Clin. Nutr.201911062864010.1093/ajcn/nqz 12631268131 PMC 6735806 · doi ↗ · pubmed ↗
- 6Chow L.S. Manoogian E.N. Alvear A. Fleischer J.G. Thor H. Dietsche K. Wang Q. Hodges J.S. Esch N. Malaeb S. Time-restricted eating effects on body composition and metabolic measures in humans who are overweight: A feasibility study Obesity 20202886086910.1002/oby.22756 PMC 718010732270927 · doi ↗ · pubmed ↗
- 7Moro T. Time-restricted eating effects on performance, immune function, and body composition in elite cyclists: A randomized controlled trial J. Int. Soc. Sports Nutr.2020176510.1186/s 12970-020-00396-z 33308259 PMC 7733258 · doi ↗ · pubmed ↗
- 8Brady A.J. Langton H.M. Mulligan M. Egan B. Effects of 8 wk of 16: 8 time-restricted eating in male middle-and long-distance runners Med. Sci. Sports Exerc.20215363364210.1249/MSS.000000000000248832796255 · doi ↗ · pubmed ↗