Photodynamic Therapy in Primary Cutaneous Skin Lymphoma—Systematic Review
Adam Zalewski, Witold Musiał, Alina Jankowska-Konsur

TL;DR
This review evaluates how well photodynamic therapy works for treating early-stage skin lymphomas, finding it effective and safe with some room for improvement.
Contribution
The paper systematically reviews clinical evidence for photodynamic therapy in primary cutaneous lymphomas, highlighting its efficacy and safety profile.
Findings
PDT showed notable efficacy in early-stage mycosis fungoides using MAL or 5-ALA.
Adjunctive techniques like microneedling improved PDT outcomes.
PDT was well tolerated with mild side effects but rare complications like neuropathy.
Abstract
Background/Objectives: Primary cutaneous lymphomas (CLs) are a group of skin-limited lymphoproliferative disorders, including cutaneous T-cell (CTCLs) and B-cell lymphomas (CBCLs). Photodynamic therapy (PDT), a non-invasive, light-activated treatment, has gained attention as a skin-directed therapy for early-stage CLs due to its selectivity and favorable safety profile. This systematic review evaluates the current evidence on the clinical use of PDT in managing CLs. Methods: A systematic literature search was conducted in PubMed, Scopus, and Embase through 1 September 2024 following PRISMA guidelines. Search terms included “primary cutaneous skin lymphoma”, “CTCL”, “CBCL”, “mycosis fungoides”, “lymphomatoid papulosis”, and “photodynamic therapy”. After screening 1033 records, 30 studies were included. Data were extracted and categorized by lymphoma subtype and clinical outcomes.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
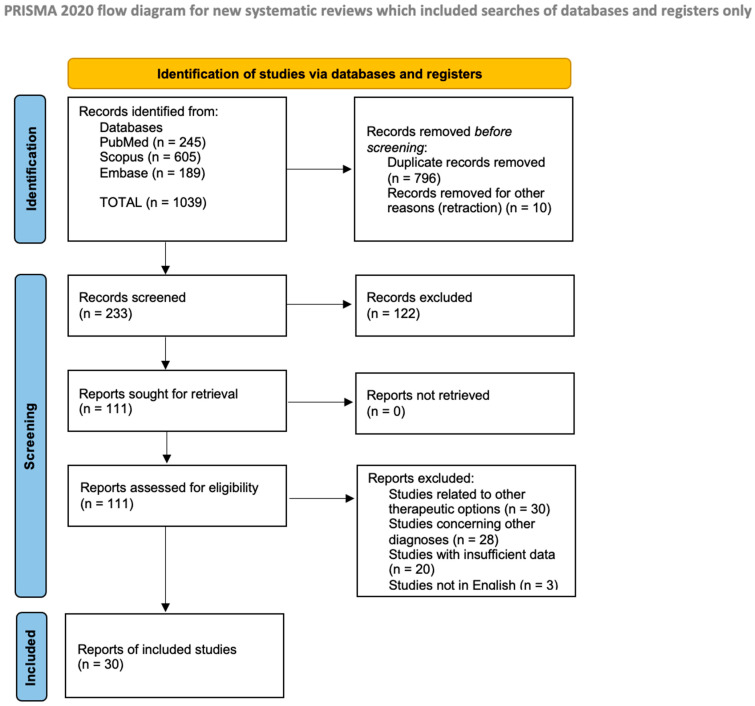 Figure 1
Figure 1- —Wroclaw Medical University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous lymphoproliferative disorders research · Nail Diseases and Treatments · Fungal Infections and Studies
1. Introduction
Primary cutaneous lymphomas (CLs) are a heterogeneous group of lymphoproliferative malignancies, with lymphatic proliferation limited to the skin at the time of diagnosis. According to the World Health Organization (WHO) and the European Organization for Research and Treatment of Cancer (EORTC) classification, CLs are divided into cutaneous T/NK-cell lymphomas (CTCLs) and cutaneous B-cell lymphomas (CBCLs) [1,2]. Of them, CTCLs account for approximately 80% and CBCLs represents 20–25% of all CLs. The CL group is characterized by considerable diversity in terms of clinical presentation, prognosis, and treatment methods. In a significant proportion of cases, with only skin involvement and a good prognosis, the treatment of choice is skin-directed therapy (SDT) due to its favorable benefit-to-risk ratio. One of the emerging SDTs is photodynamic phototherapy.
Photodynamic therapy (PDT) has emerged as a novel, non-invasive treatment modality in dermatology, particularly for superficial skin cancers and other non-oncological dermatological conditions. It involves the local or systemic administration of a photosensitizer, a light-sensitive agent that accumulates in affected tissues. When exposed to light of a specific wavelength, the photosensitizer activates, triggering processes that selectively destroy the abnormal cells. These photocytotoxic reactions only occur within the pathological tissues where the photosensitizer is distributed, ensuring targeted cell destruction [3].
The efficacy of PDT in CLs remains an area of active investigation. While some studies have reported promising results, showing PDT to be a viable option for early-stage disease with minimal side effects, its role in the broader treatment landscape remains underexplored. As the current reports are scattered and heterogeneous, a systematic review of the available literature is warranted. This paper aims to evaluate the current evidence on the use of PDT in treating CLs, highlighting its potential benefits, limitations, and future directions.
1.1. Cutaneous Skin Lymphomas
1.1.1. Cutaneous T-Cell Lymphoma
Cutaneous T-cell lymphomas (CTCLs) represent a rare group of non-Hodgkin lymphomas deriving from the T lymphocytes, with mycosis fungoides (MF) being the most prevalent entity, representing nearly 50% of cases and an overall incidence of approximately 5.6 per million persons [1,2]. The disease stages range from localized skin patches and plaques in early stages to advanced forms involving skin tumors, lymph nodes, or blood involvement [4]. In Table S1, basing on the WHO–EORTC classification criteria [1,2], the authors describe the TNM system used for MF staging.
The management of MF is highly stage-dependent. Early-stage disease (IA–IIA) generally has a favorable prognosis, with 5-year survival rates exceeding 80% for many patients and a median overall survival exceeding 20 years, comparable to the general population. It responds well to skin-directed therapies (SDTs), such as topical corticosteroids, phototherapy, and topical retinoids, to control symptoms like itching and lesions [5]. These approaches can provide significant quality-of-life improvements but do not typically result in a cure. Advanced-stage disease (IIB–IV) is associated with much lower survival rates and often requires systemic treatment such as chemotherapy, targeted biologics, and immunomodulatory therapies. Despite the emergence of new therapeutic options, data indicate that the median survival for stage IIB is approximately 5.96 years. In contrast, in more advanced cases, particularly stage IV, it decreases to 2.5–5 years in patients with extensive blood, lymph nodes, or visceral involvement [6,7,8].
1.1.2. Cutaneous B-Cell Lymphomas
According to the WHO–EORTC classification, a group of cutaneous B-cell lymphomas comprises distinct subtypes: primary cutaneous marginal zone B-cell lymphoma (PCMZL), primary cutaneous follicle center lymphoma (PCFCL), and primary cutaneous diffuse large B-cell lymphoma, leg type (PCDLBCL-LT). PCMZL and PCFCL are indolent, with good prognosis and low relapse rates, while PCDLBCL-LT is more aggressive with poorer outcomes. The diagnostic process involves a combination of clinical evaluation, histopathological examination, and immunophenotyping [9]. Treatment strategies are based on the lymphoma subtype and extent of skin involvement, with localized therapies such as radiotherapy, PDT, or excision being effective for early-stage PCMZL and PCFCL. More aggressive CBCL types, like PCDLBCL-LT, often require systemic therapies, including chemotherapy and rituximab, especially in advanced stages [9,10].
1.2. Photodynamic Therapy
First discovered in 1904 by von Tappeiner, PDT has found a permanent position among dermatological therapeutic strategies. Descriptions of PDT for skin cancer treatment date back to the 1970s when it was used at the Roswell Park Cancer Institute. These trials ultimately resulted in the FDA approval of the procedure [11]. PDT relies on three crucial components for the procedure: a non-toxic dye called a photosensitizer (PS), low-intensity visible light, and oxygen within the target diseased tissue or cell [12]. Light activates the PS, causing it to form a triplet state. This can trigger two types of reactions—Type 1, producing ROS through substrate interaction, and Type 2, generating singlet oxygen by energy transfer to molecular oxygen. Type 2 is considered the main mechanism of the PDT method [13]. Once activated, PSs accumulate in cancer cells due to tumor-specific characteristics, allowing for selective targeting. ROS cause oxidative damage, mainly via mitochondria, leading to apoptosis [12,13,14]. PSs can be delivered topically, orally, or intravenously. A major advancement is the topical use of 5-aminolevulinic acid (5-ALA), converted to protoporphyrin IX (PPIX) in the heme biosynthetic pathway. Due to ferrochelatase limitations, PPIX accumulates, producing ROS upon light exposure. 5-ALA effectively penetrates the skin and accumulates in diseased tissue, especially in lesions with impaired stratum corneum, enhancing selectivity [15,16].
Methyl aminolevulinate (MAL), a lipophilic ester of 5-ALA, penetrates deeper and is effective for actinic keratosis and superficial BCC, often combined with red light. 5-ALA and MAL are approved for topical use in various formulations in Europe and North America [13,15,17]. In North America, a 20% formulation of 5-ALA is approved for actinic keratosis treatment using blue light [13]. Hemoporfin (HMME) is a newer PS with strong PDT activity and lower phototoxicity [15]. Research is exploring multifunctional PSs activated by stimuli like pH or enzymes. Electroporation and metal complexes (e.g., ruthenium (Ru(II)) and iridium (Ir(III))) enhance delivery and allow for real-time monitoring [18,19]. These compounds offer promising features like strong spin–orbit coupling, which facilitates better interactions with oxygen, as well as low toxicity, good biocompatibility, and the ability to monitor PDT in real time via fluorescence. Such advances point toward more effective and targeted PDT approaches, with the potential for broader clinical applications in cancer and other conditions [18]. Light source choice affects PDT efficacy. Options include lasers, broad-spectrum lamps, IPL, and LEDs [15,20]. LEDs are preferred for being affordable, non-heating, and adaptable [13,21]. The effectiveness of PDT is also determined by the wavelength of light used, as light penetration into tissue is highly dependent on tissue type and wavelength. The absorption spectrum of PPIX peaks at 410 nm (Soret band) and has additional absorption peaks at 505, 540, 580, and 635 nm [15,20,22]. Shorter wavelengths (below 600 nm) penetrate less effectively, while longer wavelengths (above 850 nm) lack sufficient energy to generate reactive oxygen species (ROS) in the target tissue [3,23].
A recent trend in PDT is the use of natural daylight, known as daylight PDT (dPDT). Daylight provides a convenient and less painful alternative to artificial light sources [24]. Though slower, it is effective and less painful for conditions like actinic keratosis [22,24,25]. Light fluence and fluence rate influence PDT results. Lower rates preserve oxygen and favor apoptosis over necrosis [26,27]. A proper light setup optimizes results and reduces discomfort [28].
2. Materials and Methods
In this study, we conducted a literature review on the clinical cases concerning PDT use in CL patients, following PRISMA guidelines [29]. We searched three electronic databases—PubMed, Scopus, and Embase—on 1 September 2024 for articles published since 1990. The search utilized the following medical subject heading (MeSH) terms: “primary cutaneous skin lymphoma” OR “mycosis fungoides” OR “lymphomatoid papulosis” OR “CTCL” OR “CBCL” AND “photodynamic therapy”. Our initial search yielded 1033 articles. After removing duplicates, we were left with 227 papers. Two independent reviewers screened the studies in two phases: first based on titles and abstracts and then through full-text review. The first screening identified 105 records; however, upon a thorough review of titles and abstracts to assess eligibility—during which non-English articles and those lacking sufficient data or related to other hematological conditions were excluded—we included a total of 30 articles in our review. A PRISMA flow diagram was created to illustrate this process (Figure 1). All articles were managed using Zotero 5.0 under an AGPL license. Given the observational nature of most included studies, the certainty of evidence was rated low to moderate. A formal GRADE assessment was not performed, but limitations such as a lack of randomization or protocol heterogeneity were acknowledged. Another important limitation of this review is the relatively small sample size, with only 30 studies meeting the inclusion criteria, most of which involved limited patient numbers and case-based evidence. The absence of large-scale, randomized controlled trials (RCTs) restricts the generalizability of the findings and prevents firm conclusions regarding the comparative efficacy and long-term outcomes of photodynamic therapy in primary cutaneous lymphomas.
The review was not registered in PROSPERO or any other registry, and no separate protocol was prepared.
3. Results
Of all collected articles, 5 studies concerned patients with lymphomatoid papulosis, 23 records provided data about PDT therapy among patients with MF, and 2 reports related to CBCL. The analysis of the data revealed that photodynamic therapy (PDT) demonstrates significant clinical efficacy, particularly in early-stage and localized cases, with both methyl aminolevulinate (MAL) and 5-aminolevulinic acid (5-ALA) used as effective photosensitizers. The results of our research are presented in Table 1, Table 2 and Table 3.
4. Discussion
4.1. PDT in Skin Lymphomas
Photodynamic therapy (PDT) has emerged as a promising treatment option in lymphomatoid papulosis (LyP), early-stage mycosis fungoides (MF) and cutaneous B-cell lymphomas (CBCLs), including marginal-zone lymphoma (MZL)-type CBCL [58,60]. It differs in several aspects from its application in other malignancies, especially due to the hematologic origin and unique pathophysiology of the disease. Unlike epithelial tumors, CLs consist of malignant T-cells infiltrating the epidermis and superficial dermis, which may affect the uptake and distribution of topically applied photosensitizers [61]. Furthermore, due to the chronic and multifocal nature of CLs, PDT is typically used for localized, early-stage lesions, rather than as a definitive curative therapy as in actinic keratoses or basal cell carcinomas [62,63]. The precise mechanism by which PDT exerts its therapeutic effects in CLs remains not fully understood. While PDT is known to induce direct cytotoxicity through the generation of reactive oxygen species (ROS), leading to the apoptosis or necrosis of malignant cells, the relative contributions of direct tumor cell death versus immune-mediated effects are still under investigation [23]. Studies suggest that PDT may also trigger immunogenic cell death (ICD), characterized by the release of damage-associated molecular patterns (DAMPs) such as calreticulin, heat shock proteins, and high mobility group box 1 protein (HMGB1), which can enhance dendritic cell maturation and subsequent T-cell activation [61]. Immune-mediated mechanisms therefore appear to play a more prominent role in CLs than in solid tumors, with PDT-induced inflammation and cytokine release potentially enhancing antitumor immunity. The typically ill-defined and diffuse morphology of CL lesions can also complicate treatment planning, requiring individualized light delivery approaches. These differences underscore the need for disease-specific protocols and further research to elucidate the complex interplay between cytotoxic and immunomodulatory effects in PDT-treated CLs [61,63].
4.1.1. PDT in Lymphomatoid Papulosis (LyP)
PDT has shown potential as a treatment for refractory LyP, particularly in cases resistant to conventional therapies. Case studies have illustrated its effectiveness across diverse patient profiles. For example, a pediatric case involving a 13-year-old boy with extensive LyP lesions, unresponsive to other therapies, achieved complete resolution in the affected area after two months of PDT in conjunction with narrowband UVB treatment, demonstrating the potential of PDT in pediatric cases due to its minimal toxicity and non-invasive nature [32].
For adult patients with treatment-resistant LyP, PDT has provided effective, localized control of lesions. A case report by Rodrigues et al. [30] described a 40-year-old woman with LyP whose persistent lesions on the abdomen were cleared after two PDT sessions, remaining in remission for 11 months post-treatment [30]. The mechanism behind PDT’s efficacy may involve immunogenic cell death, where PDT stimulates the release of DAMPs, like HMGB1 and calreticulin, which can enhance immune response and prevent recurrence [31]. However, PDT is not without risks; a rare but serious side effect was reported in a 38-year-old patient who experienced transient leg paralysis after treatment on lesions near the thoracic spine, possibly due to nerve inflammation caused by free radicals generated during PDT [33].
Collectively, these cases suggest that while PDT offers a promising option for managing LyP, especially for localized, symptomatic, and therapy-resistant lesions, careful consideration regarding treatment areas and potential side effects is required.
4.1.2. PDT in Cutaneous T-Cell Lymphomas (CTCLs)
PDT has been successfully used for early-stage MF, with various studies reporting complete response rates ranging from 20–100% depending on the stage and the photosensitizer used [64,65]. The first report of beneficial ALA PDT for MF was published in 1994 [66], and since then, various studies have confirmed its efficacy. Between 1994 and 2001, several small studies and case reports demonstrated that topical 5-ALA PDT could induce both clinical and histological remission in patients with unilesional or early-stage MF [51,52,53,54,55,56,57]. For instance, Wolf et al. [52] and Stables et al. [54] noted the complete clearance of treated lesions, histologically confirmed with durable remission, while Markham et al. [57] documented the effective treatment of tumor-stage MF. Although these studies involved small numbers of patients, they offered compelling early evidence for the feasibility and therapeutic potential of PDT in CTCL and established the base for future trials. Another notable example of PDT efficacy in MF is the work by Hooper et al. [67], who observed a 67% complete response rate in patients with stage IA MF. Similarly, the use of silicon phthalocyanine (Pc 4) in PDT has been tested in various studies, including those targeting MF. Pc 4, a second-generation photosensitizer, has shown partial response rates of around 40% in stage I–II MF when used in conjunction with red light (675 nm) [60,68]. Although the results from clinical trials are promising, further studies are needed to better understand the optimal dosages, light fluence, and mechanisms underlying PDT’s effects on lymphoma cells, as well as its long-term impact on disease recurrence.
A retrospective study of Barrachin et al. [35] focused on the efficacy and safety of using MAL as a photosensitizer for PDT in patients with early-stage MF. The results showed significant clinical improvements in lesion appearance, with a high tolerance among patients. The study concluded that MAL PDT could be a viable non-invasive treatment option, reducing the need for more aggressive therapies and offering a favorable safety profile [35]. It may also be an option for treating cervical and facial lesions associated with folliculotropic MF as well as uni- or paucilesional MF [41,42,43,47,50,69]. There are also studies demonstrating effective results, supporting the application of PDT in sensitive facial areas with erosive lesions where conventional treatments might be inadequate [49]. In another study concerning PDT use in MF patients, the authors presented two case studies where patients diagnosed with follicular mucinosis—a distinct variant of MF—were treated with PDT [36]. The treatment resulted in notable clinical improvement, suggesting that PDT is effective for this less common presentation of MF. This study underscores the versatility of PDT beyond typical MF cases, indicating its potential application in treating related skin conditions [36]. In the study by Dairi et al. [37], the authors utilized an ablative fractional CO2 laser (AFL) in conjunction with PDT to treat localized MF. This approach aimed to enhance the penetration of the photosensitizer and improve treatment efficacy, particularly for resistant lesions. The combination therapy demonstrated promising results, showing both clinical and histological improvements in treated patients, indicating that an AFL can significantly improve the effectiveness of PDT for localized MF [37].
Kim et al. [38] addressed a letter concerning a specific case where a patient with MF exhibited an incomplete response to topical 5-ALA therapy. The authors emphasized the variability in patient responses to topical treatments and advocated for alternative therapies, such as PDT, to achieve better outcomes for patients who do not adequately respond to standard treatments [38]. In 2016, Han et al. [39] reported on three patients with refractory-plaque-stage MF who underwent PDT. They highlighted PDT’s potential as an effective option for patients who have not responded to traditional therapies, demonstrating its efficacy in more resistant forms of MF [39]. Moreover, results of 5-ALA use in PDT showed significant improvements in both the clinical symptoms and histological features of the disease [44,48].
The way of administering the photosensitizer was evaluated through the intradermal application of 5-ALA in PDT for treating tumor lesions in MF patients [40]. The findings revealed notable reductions in lesion size and improved appearance, indicating that the intradermal method enhances the penetration of the photosensitizer, resulting in superior clinical outcomes compared with topical applications alone [40].
A case report by Paech et al. [45] described a patient with advanced HIV and MF who achieved remission after receiving topical 5-ALA and PDT. Results suggest that PDT can be effective even in immunocompromised patients, thus broadening the applicability of this therapy in complex cases of MF [45].
Not only conventional but also daylight PDT can bring satisfactory results in treating palmoplantar lesions in MF patients [46]. The findings of a study from 2021 indicated that PDT effectively managed challenging skin lesions, providing a non-invasive treatment alternative that was well received by patients [46].
Overall, the expanding role of photodynamic therapy in managing mycosis fungoides has been illustrated, providing evidence for its efficacy across different forms and stages of the disease. The findings underscore the versatility of PDT as a non-invasive option, particularly for localized or less common presentations of MF, thereby enhancing treatment options for patients.
4.1.3. PDT in Cutaneous B-Cell Lymphomas (CBCLs)
While PDT has shown more established results in treating CTCLs, its application in CBCLs, such as marginal-zone lymphoma (MZL), is relatively novel but promising. The first successful ALA PDT treatment of early-stage CBCL was reported in 2006 [59]. More recently, Toulemonde et al. [58] conducted a case series of MZL-type CBCL patients treated with PDT, yielding favorable outcomes. PDT in CBCL works similarly to CTCL by using photosensitizers like 5-ALA or MAL, which accumulate in the lymphoma cells and are activated by light to induce apoptosis. One challenge in treating CBCL with PDT is the deeper localization of atypical lymphocytes, which can make it harder for photosensitizers to penetrate the skin’s deeper layers [58]. To overcome this, some studies have incorporated microneedling before PDT, which enhances the skin’s permeability and boosts photosensitizer uptake, leading to improved therapeutic outcomes [58,70,71].
In a study of four patients with MZL-type CBCL, all were treated with MAL PDT after presenting with multiple skin lesions, making PDT a preferred option over surgery or radiotherapy [58]. The patients, aged 27 to 64, underwent skin biopsies to confirm diagnosis, and two had previously received rituximab. A dermaroller was used to enhance MAL penetration, followed by illumination using an AKTILITE device. Each patient underwent multiple PDT sessions, and the results showed varying degrees of effectiveness. Two patients achieved complete clinical and histological remission, one showed clinical improvement but had histologically persistent disease, and one had a mixed response with partial lesion resolution. No new lesions developed during treatment, and the average pain reported was moderate, with one patient discontinuing two sessions due to pain. This approach has the potential to reduce PDT dosage and side effects by allowing for lower concentrations of photosensitizers and light exposure. However, recurrence remains a concern, as PDT, like other localized treatments (e.g., corticosteroids or topical imiquimod), primarily targets visible lesions and does not prevent distant relapse [58].
4.1.4. Clinical Trials
As PDT has found more and more applications in general dermatology, the following trials were conducted to underscore the potential of PDT in treating early-stage and refractory CTCL, highlighting a range of response rates depending on the stage and treatment approach.
NCT01800838: This study examined the safety and efficacy of topical silicon phthalocyanine (Pc 4) for treating IA–IIA mycosis fungoides by evaluating a protocol of dosage acceleration. All participants (n = 11) completed the trial without experiencing any serious adverse effects. The maximum tolerated dose (MTD) for photodynamic therapy (PDT) was established at 150 J/cm^2^, while for Pc 4, it was 0.1 mg/mL [72].
NCT03281811: This trial investigated the effects of ALA PDT on refractory tumors and plaques in patients with mycosis fungoides, demonstrating a moderate response rate of 36.4% (measured with PGA). Treatment was repeated every 4 weeks. Up to six cycles were performed. At week 24, patients started radiation therapy and continued it daily for 4 weeks [73,74].
NCT00103246: This study focused on the safety profile and tolerability of Pc4 administered topically before red light PDT in subjects with various non-melanoma skin neoplasms and pre-neoplastic conditions. Particularly beneficial results were observed among MF patients where 14 of 35 (40%; 95% CI: 0.26–0.56) subjects showed a clinical response, with a good treatment tolerability [75].
NCT00023790: The aim of this study was to determine the maximum tolerated dose of Pc4 with a fixed dose of light and the dose of light when administered with a fixed dose of the drug. Unfortunately, the trial was terminated due to slow patients’ accrual [76].
NCT00054171: This study was constructed to evaluate the effectiveness of PDT with short (1–2.5 h), medium (4–6 h), and long (18–24 h) applications of 20% ALA in CTCL/CBCL and early chronic leukemia with the skin involvement. Determining the maximal irradiance and corresponding exposure among multiple treatments as well as the number of sessions needed to complete treatment were one of the study’s objectives. Nevertheless, no results have yet been posted [77].
NCT02448381: This trial centered on the efficacy of synthetic hypericin, with response rates increasing with additional treatment cycles, particularly for early-stage CTCL. After three cycles of the therapy, the response rate was assessed at 49% of the study participants. Together with a low rate of AEs, the efficacy of this treatment modality may indicate that synthetic hypericin PDT may be an effective option for MF/CTCL management [78].
NCT05380635: This study investigated the safety of 0.25% hypericin topical ointment used twice a week for 8 weeks, followed by visible light radiation. It was found that 25.9% (n = 7) of patients achieved ≥50% improvement in disease severity, and 14.8% (n = 4) reached 100% improvement. Mild local reactions but no severe adverse effects were reported [79].
These trials underscore the potential of PDT in treating early-stage and refractory CTCL, highlighting a range of response rates depending on the stage and treatment approach.
4.1.5. Adverse Effects Associated with PDT
While generally well tolerated, PDT can be associated with several adverse effects [80,81]. Below in Table 4, the authors summarize the potential side effects of PDT treatment.
4.1.6. Treatment Limitations
Despite encouraging results from small-sample studies, no comparative data currently exist evaluating the efficacy of PDT against other well-established skin-directed therapies for early-stage cutaneous lymphomas. Standard topical treatments such as corticosteroids, chlormethine (mechlorethamine), calcineurin inhibitors (e.g., tacrolimus), imiquimod, ingenol mebutate, and localized radiotherapy including electron beam therapy have been used with varying success in early-stage MF, yet head-to-head studies comparing these modalities with PDT are lacking [1,6,9,82]. The absence of comparative trials limits the ability to position PDT in the current therapeutic algorithm and underlines the need for randomized studies to determine its effectiveness, safety profile, and long-term outcomes compared with existing topical treatments [80,83].
Moreover, PDT is an office- or hospital-based procedure. The administration of photosensitizers and the use of controlled light sources require a clinical setting equipped with an appropriate devices and trained personnel [83]. Additionally, patient monitoring during and after illumination is essential due to the possibility of side effects such as pain or erythema [33]. These requirements are in line with current dermatological guidelines, which recommend that PDT be performed in specialized healthcare facilities to ensure safety and treatment efficacy [80].
5. Conclusions
In conclusion, PDT represents a promising, non-invasive treatment option for both CTCLs and CBCLs, particularly in early-stage disease. While PDT for MF and MZL-type CBCL has shown encouraging results, further studies are needed to refine treatment protocols, optimize photosensitizer use, and address challenges like disease recurrence. The development of new photosensitizers, combined with innovative techniques like microneedling, could enhance the efficacy of PDT and offer an alternative or adjunctive therapy for patients with localized cutaneous lymphoma. Direct comparative studies between PDT and other skin-directed therapies are limited. As of our current knowledge, there are also no direct comparative studies evaluating the effectiveness of 5-ALA versus MAL in PDT specifically for CSLs. It would be of special importance to conduct head-to-head studies to improve clinical outcomes of therapeutic management. As clinical trials continue to explore these options, PDT may become an increasingly integral part of the therapeutic landscape for cutaneous lymphomas.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Willemze R. Jaffe E.S. Burg G. Cerroni L. Berti E. Swerdlow S.H. Ralfkiaer E. Chimenti S. Diaz-Perez J.L. Duncan L.M. WHO-EORTC classification for cutaneous lymphomas Blood 20051053768378510.1182/blood-2004-09-350215692063 · doi ↗ · pubmed ↗
- 2Willemze R. Cerroni L. Kempf W. Berti E. Facchetti F. Swerdlow S.H. Jaffe E.S. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas Blood 20191331703171410.1182/blood-2018-11-88126830635287 PMC 6473500 · doi ↗ · pubmed ↗
- 3Kwiatkowski S. Knap B. Przystupski D. Saczko J. Kędzierska E. Knap-Czop K. Kotlińska J. Michel O. Kotowski K. Kulbacka J. Photodynamic therapy—Mechanisms, photosensitizers and combinations Biomed. Pharmacother.20181061098110710.1016/j.biopha.2018.07.04930119176 · doi ↗ · pubmed ↗
- 4Larocca C. Kupper T. Mycosis Fungoides and Sézary Syndrome Hematol. Oncol. Clin. N. Am.20193310312010.1016/j.hoc.2018.09.001PMC 714724430497668 · doi ↗ · pubmed ↗
- 5Morgenroth S. Roggo A. Pawlik L. Dummer R. Ramelyte E. What Is New in Cutaneous T Cell Lymphoma?Curr. Oncol. Rep.2023251397140810.1007/s 11912-023-01464-837874473 PMC 10640416 · doi ↗ · pubmed ↗
- 6Brunner P.M. Jonak C. Knobler R. Recent advances in understanding and managing cutaneous T-cell lymphomas F 1000 Research 2020933110.12688/f 1000 research.21922.1PMC 720208632419924 · doi ↗ · pubmed ↗
- 7Dobos G. Miladi M. Michel L. Ram-Wolff C. Battistella M. Bagot M. de Masson A. Recent advances on cutaneous lymphoma epidemiology Presse Med.20225110410810.1016/j.lpm.2022.10410835026392 · doi ↗ · pubmed ↗
- 8Talpur R. Singh L. Daulat S. Liu P. Seyfer S. Trynosky T. Wei W. Duvic M. Long-term outcomes of 1263 patients with mycosis fungoides and Sézary syndrome from 1982 to 2009 Clin. Cancer Res.2012185051506010.1158/1078-0432.CCR-12-060422850569 PMC 3857608 · doi ↗ · pubmed ↗