Articulating Materials Are Determinants of Survivorship of Hip Arthroplasties Performed for Nontraumatic Osteonecrosis of the Femoral Head
Seneki Kobayashi, Nobuhiko Sugano, Wataru Ando, Wakaba Fukushima, Kyoko Kondo, Takashi Sakai

TL;DR
This study identifies specific risk factors for hip arthroplasty reoperation in patients with nontraumatic osteonecrosis of the femoral head.
Contribution
The study provides new insights into risk factors specific to different types of hip arthroplasties in ONFH patients.
Findings
Conventional polyethylene and metal acetabular-articulating materials increase reoperation risk in THAs.
Minimum-incision surgery and alumina BPs increase reoperation risk in BPs.
ONFH-associated factors like steroid use and alcohol consumption are significant risk factors.
Abstract
A nationwide multicenter follow-up cohort study of hip-replacement arthroplasties performed for nontraumatic osteonecrosis of the femoral head (ONFH) was conducted to clarify factors associated with need for reoperation. We analyzed 7393 arthroplasties including 6284 total hip arthroplasties (THAs), 886 bipolar hemiarthroplasties (BPs), 188 total resurfacing arthroplasties, and 35 hemi-resurfacing arthroplasties (hRSs). The identified risk factors were combined systemic steroid use and excessive alcohol consumption (both ONFH-associated factors), a lateral approach, alumina BPs (aBPs), and hRSs, which were reported previously. The present study performed further analyses separately for THAs and BPs to clarify risk factors in each surgical group. A Cox proportional-hazard model identified the following risk factors: the acetabular-articulating materials of conventional polyethylene (cPE)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
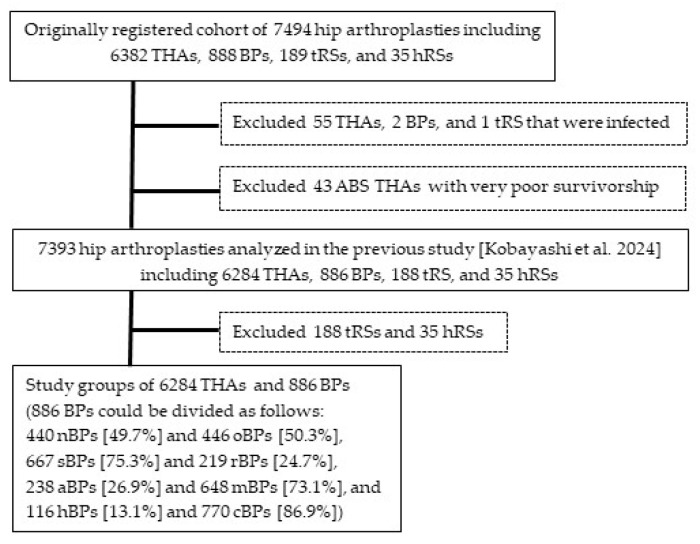 Figure 1
Figure 1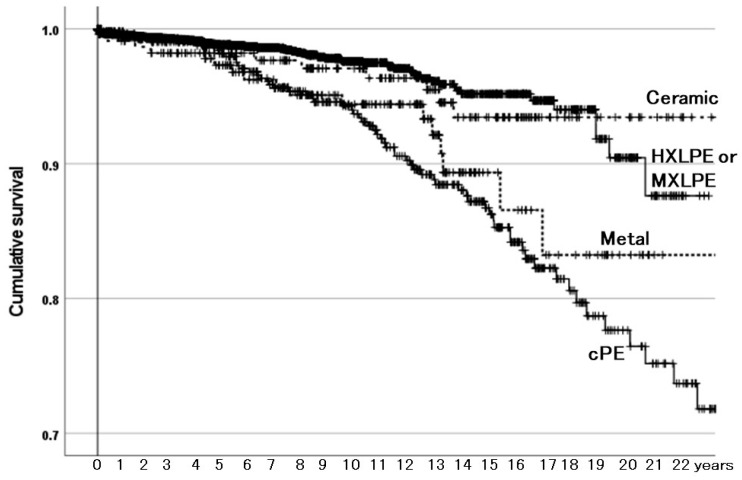 Figure 2
Figure 2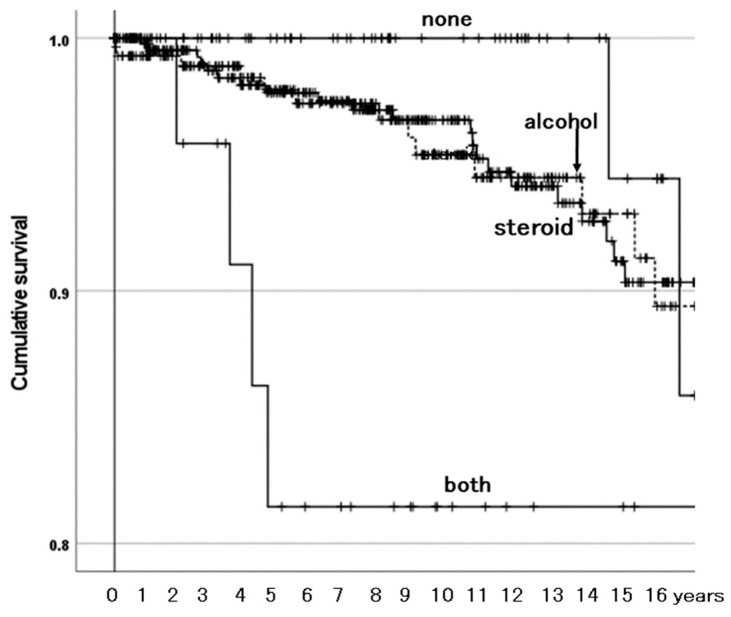 Figure 3
Figure 3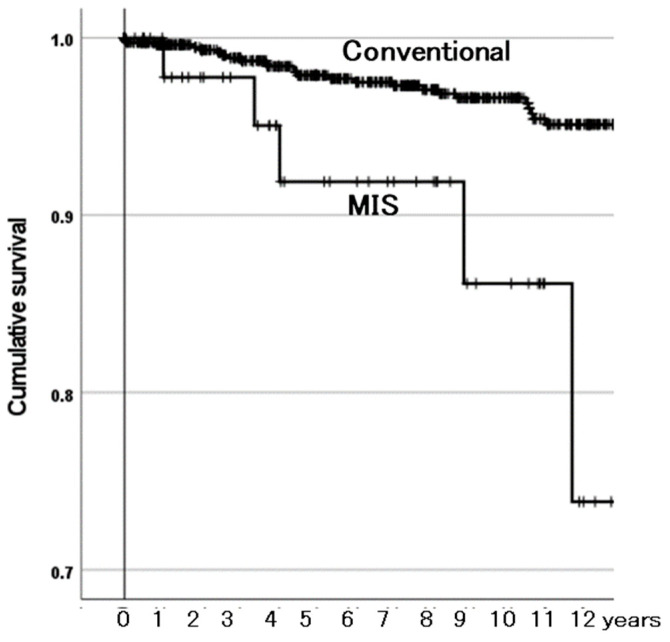 Figure 4
Figure 4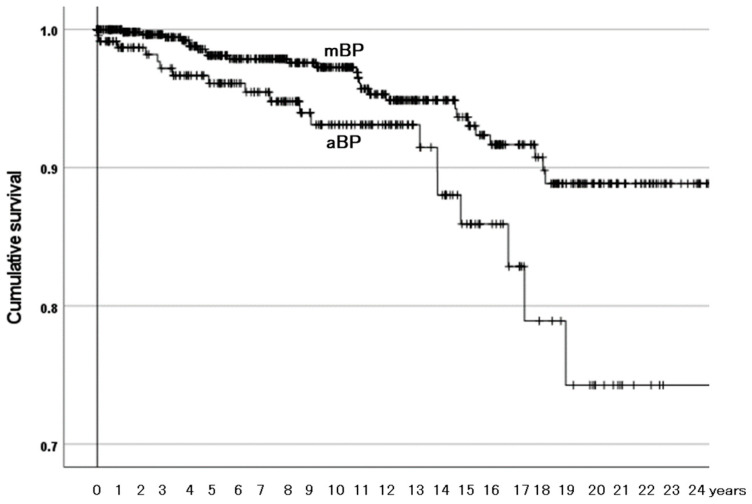 Figure 5
Figure 5- —Health Labour Sciences Research Grant, the Ministry of Health, Labour and Welfare, Japan
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone and Joint Diseases · Orthopaedic implants and arthroplasty · Orthopedic Infections and Treatments
1. Introduction
Nontraumatic osteonecrosis of the femoral head (ONFH) patients undergoing hip-replacement arthroplasties are generally younger, more often of the male gender [1], and at higher risks of postoperative dislocation [2,3] and a need for reoperation [4,5,6,7,8], compared with patients undergoing the procedures mainly for osteoarthrosis (OA). Hip arthroplasty practice has changed noticeably. In total hip arthroplasty (THA), acetabular liners made of highly (approximately 10 Mrad) cross-linked polyethylene (HXLPE) and larger prosthetic heads have increasingly been used. In bipolar hemiarthroplasties (BPs), usually performed for ONFH before the development of OA, many modifications have been made to improve their poor results [9,10]. To reduce osteolysis due to polyethylene debris generated by neck–outer head impingement in BP [11,12], a new type of BPs (nBPs) with a smooth, small-diameter (approximately 10 mm) neck without any sharp corners began to replace other BPs (oBPs) [1]. As contemporary femoral prostheses tended to have a neck with a larger diameter, ‘small-diameter’ was excluded from the definition, which described BPs with a smooth neck (sBPs) and the others with a rough-surfaced neck (rBPs). Alumina BPs (aBPs, with the outer surface of the outer head made of alumina ceramic) were developed to surpass the durability of metal BPs (mBPs). BPs with HXLPE in the outer head (hBPs) were also developed to improve the survivorship of BPs with conventional polyethylene (cPE) (cBPs). However, their efficacy has not been clinically proven. Therefore, hip-replacement arthroplasties performed for OFNH should be monitored; this was conducted in a nationwide multicenter follow-up cohort study.
In a survey conducted in 2023, we analyzed arthroplasties including THAs, BPs, total resurfacing arthroplasties (tRSs), and hemi-resurfacing arthroplasties (hRSs). The identified risk factors were combined systemic steroid use and excessive alcohol consumption (both ONFH-associated factors), a lateral approach, aBPs, and hRSs, which were reported previously [13]. However, it was not clear which risk factors were applicable to which surgical treatments. Our hypothesis was that risk factors could be specific to each surgical treatment. Therefore, the present study performed further analyses separately for THAs and BPs to clarify risk factors in each surgical group.
2. Materials and Methods
2.1. THAs and BPs Analyzed for Factors Related to Need for Reoperation
The previous study [13] described the method of the nationwide multicenter follow-up cohort study of hip-replacement arthroplasties performed for ONFH and the demographic and operative details of the 7393 arthroplasties (after exclusion of 58 infected hips and 43 ABS THAs with very poor survivorship from the entire cohort of 7494 arthroplasties observed in the 2023 survey) that were analyzed for factors related to need for reoperation. They included 6284 THAs (85.0%), 886 BPs (12.0%), 188 tRSs (2.5%), and 35 hRSs (0.5%) (Figure 1). THAs and tRSs were performed in all ONFH stages, while BPs and hRSs were performed mainly before stage 4 (OA). The 886 BPs could be divided into two in four ways. As for hip prostheses and their providers, 81 types of acetabular components were provided by 15 companies and 137 types of femoral components by 18 companies.
2.2. Statistical Analyses
Factors related to need for reoperation were analyzed with a Cox proportional-hazard model using IBM SPSS statistics version 29 (IBM Corp, Armonk, NY, USA). Univariate analyses were first performed by applying the model to each of the demographic and operative variables with a significance level of p < 0.1. Variables with p < 0.1 were then examined together using the model with a significance level of p < 0.05 (multivariate analysis). Effects of the identified risk factors on the survivorship of hip arthroplasties were illustrated with the Kaplan–Meier estimator (with log-rank tests) with a significance level of p < 0.05. A χ^2^ test was used to compare the prevalence of categorical data and a t-test was used to compare means with a significance level of p < 0.05.
2.3. Ethical Approvals
Ethical approvals for this study were comprehensively obtained at three representative institutions: Shinshu University School of Medicine (8 January 2008, No. 1043), Suwa Red Cross Hospital (27 November 2014, No. 26–23 and 26 March 2019, No. 30–19), and Osaka University Graduate School of Medicine (29 January 2021, No. 20461). This study was carried out in accordance with the World Medical Association Declaration of Helsinki. All participants included in the study gave informed consent and agreed to participate in this study and to have their data published in a journal.
3. Results
3.1. Comparison of Demographic and Surgical Variables Between THAs and BPs
The demographic and operative features of the 6284 THAs and the 886 BPs and their comparisons are listed in Table 1. They were different between the two surgical groups except for patient weight.
3.2. Analyses of the 6284 THAs
3.2.1. Cox Proportional-Hazard Model Analyses
The follow-up of the 6284 THAs ranged from 0.1 to 27 (mean of 6.5) years, during which 189 hips (3.0%) needed reoperation. The univariate analyses identified five of the variables listed in Table 1 with p < 0.1 (Table 2). However, in the χ^2^ tests, incision length, femoral head material, and head diameter were strongly related (p < 0.001). THAs with a 22 mm prosthetic head were performed with conventional incision in 92.2% of cases, and the 22 mm heads were made of metal in 78.2% of cases. Therefore, incision length and head material were not included in the next multivariate analyses. As the remaining three variables had been reported concerning the survivorship of THAs and without a strong relationship between them, they were examined together with the model.
The multivariate survivorship analysis identified only acetabular-articulating material as a risk factor with p < 0.05 (Table 3). Compared with HXLPE or MXLPE, cPE and metal (cobalt–chrome or metal-on-metal THA) had inferior survivorship (p < 0.001 and p = 0.028, respectively), whereas that of ceramic (ceramic-on-ceramic THA) did not differ (p = 0.765).
3.2.2. Survivorship Illustrated with Kaplan–Meier Estimator
The Kaplan–Meier estimator illustrated the effects of the acetabular-articulating materials on the survivorship of THAs with need for reoperation as the endpoint (Figure 2). Compared with the HXLPE or MXLPH group, the cPE and metal (metal-on-metal THA) groups had inferior survivorship, but the ceramic (ceramic-on-ceramic THA) group did not. The rates of need for reoperation were also different among them in a χ^2^-test (p < 0.001): 1.8% in the HXLPE or MXLPE group, 11.6% in the cPE group, 6.6% in the metal group, and 4.3% in the ceramic group.
Regarding reasons for need for reoperation, in the HXLPE or MXLPE group, recurrent dislocation was at the top, followed by periprosthetic femoral fracture (Table 4). In the cPE group, the most frequent three reasons were osteolysis, polyethylene wear and/or breakage, and recurrent dislocation. The top reason was adverse reaction to metal debris (ARMD) in the metal (metal-on-metal THA) group and recurrent dislocation in the ceramic (ceramic-on-ceramic THA) group.
3.3. Analyses of the 886 BPs
3.3.1. Cox Proportional-Hazard Model Analyses
The follow-up of the 886 BPs ranged from 0.1 to 27 (mean, 9.6) years, during which 47 hips (5.3%) needed reoperation. The univariate analyses identified three of the variables listed in Table 1 with p < 0.1, i.e., ONFH-associated factors, incision length, and aBPs (Table 5). Without strong relationship among them, they were examined together with the model.
In the multivariate survivorship analysis, all the three variables were confirmed as risk factors with p < 0.05 (Table 6). Combined systemic steroid use and excessive alcohol consumption (both ONFH-associated factors) had a higher risk, with no associated factors as a reference (p = 0.008). Compared with conventional incision, minimal-incision surgery (MIS, defined as the use of a ≤ 10 cm incision to complete a hip arthroplasty) had a higher risk (p < 0.001). The aBPs had a higher risk than the mBPs (p = 0.004).
3.3.2. Survivorship Illustrated with Kaplan–Meier Estimator
The Kaplan–Meier estimator illustrated the effects of the three identified risk factors on the survivorship of BPs with need for reoperation as the endpoint. Among the ONFH-associated factor groups, the group with both factors was at a higher risk than the other groups (Figure 3). The other groups were not different from one another in survivorship. The MIS group had lower survivorship than the conventional incision group (Figure 4). The aBPs had lower survivorship than the mBPs (Figure 5). The rates of need for reoperation were also different between them in a χ^2^-test (p = 0.014): 4.2% in the mBPs and 8.4% in the aBPs. In both groups, the proximal migration of the outer head was the main reason for need for reoperation in 17 of 27 (63.0%) of the mBPs and 13 of 20 (65.0%) of the aBPs (Table 7).
4. Discussion
In the previous report, regarding need for reoperation, analyses of 7393 arthroplasties including 6284 THAs, 886 BPs, 188 tRSs, and 35 hRSs identified the following risk factors: both ONFH-associated factors, a lateral approach, aBPs, and hRSs [13]. However, it was not clear which risk factors were applicable to which surgical treatments. In the present study, further analyses performed separately for the 6284 THAs and 886 BPs revealed that risk factors were specific to each surgical group: acetabular-articulating material in the THAs and having both ONFH-associated factors, MIS, and aBPs in the BPs.
4.1. Acetabular-Articulating Material Is a Determinant of Survivorship of THAs
In the Australian registry, the cumulative percent revision of primary THAs performed for OA was higher with cPE than with HXLPE, and it was higher with metal-on-metal bearing than with metal-on-HXLPE bearing, but it was not different between ceramic-on-ceramic and metal-on-HXLPE bearings [4]. In a cohort study of 253 metal-on-metal THAs with a median follow-up of 11.5 years, 34 hips were revised, with survival rates of 89.6% at 10 years and 82.9% at 14.6 years, and 19 of them (55.9%) were revised due to ARMD [14]. In the present study, compared with the HXLPE or MXLPH group, the cPE and the metal groups had inferior survivorship; survival rates with HXLPE or MXLPH, cPE, and metal were 90%, 78%, and 83% at 20 years, respectively, whereas that of the ceramic group did not differ (Figure 2). Reasons for need for reoperation in the HXLPE or MXLPE group included recurrent dislocation at the top, followed by periprosthetic femoral fracture (Table 4). In the ceramic group, recurrent dislocation was also at the top. In the cPE group, the most frequent three reasons were osteolysis, polyethylene wear and/or breakage, and recurrent dislocation, which could be related, to some extent, to the inferior properties of cPE compared with those of HXLPE or MXLPE. In the metal group, ARMD was the top reason. Therefore, acetabular-articulating material was an important determinant of the survivorship of the THAs.
4.2. Combined Existence of Both ONFH-Associated Factors Affects Survivorship of BPs
Systemic steroid use [6] and excessive alcohol consumption [15,16] were risk factors associated with reoperation in THAs for ONFH. In the present study, the combined existence of both factors was a risk factor related to need for reoperation not in the THAs but in the BPs. This is reported for the first time to our knowledge.
4.3. MIS Affects Survivorship of BPs
As for MIS, in a report based on data from the Norwegian Arthroplasty Register, the revision rates associated with the MIS anterior and anterolateral approaches were not increased compared with those of the conventional posterior and direct lateral approaches [17]. We could not find any study that analyzed influence of MIS on the reoperation risk of BPs. However, the reoperation risk of the BPs performed with MIS was higher than that of the PBs performed using conventional incisions.
4.4. The Material of the Outer Head Articulating with Cartilage Is a Determinant of Survivorship of BPs
The patho-mechanism of the inferior durability of the aBPs was discussed in the previous report [13]. In short, articulation with the BP outer head could be harmful to the acetabular cartilage, and the better lubrication of cartilage with aBP than with mBP could increase articulation in aBP, leading to the proximal migration of the outer head and pain, resulting in a higher risk of reoperation in aBPs than in mBPs.
4.5. Little Difference Based on Component Fixation in Survivorship of THAs
Component fixation has been many hip surgeons’ interest in relation to the durability of hip prostheses. In the Australian registry, in the cumulative percent revision of primary THAs performed for OA, there was little difference in outcomes based on fixation (cemented, hybrid, or cementless), except for patients aged ≥ 75 years, where the revision rate was lower when either hybrid or cemented fixation was used [4]. As for younger patients, in a study analyzing the most commonly used uncemented, hybrid, and fully cemented implant combinations in the New Zealand registry, in 40–55-year-old patients, revision rates were comparable between the uncemented and the hybrid implant combinations, whereas the cemented implant combination exhibited a higher revision rate. In <40-year-old patients, the revision rate for the hybrid implant combination was significantly lower than that for the uncemented implant combination [18]. In the present study of THAs and BPs performed for ONFH, fixation (uncemented/cement and surface finish of femoral stem) was not associated with need for reoperation.
4.6. Limitations
Some patient-related and operative data were lacking, e.g., surgical experience. Hip arthroplasty practice changed over the observation period in surgical approach, component fixation, acetabular-articulating material, and the material and diameter of the femoral head, although all of them were analyzed in the present study. Information on complications unrelated to reoperation could not be obtained, given the constraints involving the 31 institutions. THAs and BPs performed only for Japanese ONFH patients were analyzed. All of them warrant further research.
5. Conclusions
The present further analyses performed separately for the 6284 THAs and 886 BPs revealed that risk factors associated with need for reoperation were specific to each surgical group: acetabular-articulating material in the THAs and both ONFH-associated factors, MIS, and aBPs in the BPs. The articulating materials, i.e., the acetabular-articulating material in the THAs and the alumina outer surface of the outer head in the BPs, were important determinants in the survivorship of hip prostheses in ONFH patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kobayashi S. Kubo T. Iwamoto Y. Fukushima W. Sugano N. Nationwide multicenter follow-up cohort study of hip arthro-plasties performed for osteonecrosis of the femoral head Int. Orthop.2018421661166810.1007/s 00264-018-3980-129754187 · doi ↗ · pubmed ↗
- 2Kunutsor S.K. Barrett M.C. Beswick A.D. Judge A. Blom A.W. Wylde V. Whitehouse M.R. Risk factors for dislocation after primary total hip replacement: A systematic review and meta-analysis of 125 studies involving approximately five million hip re-placements Lancet Rheumatol.20191 e 111e 12110.1016/S 2665-9913(19)30045-138229338 · doi ↗ · pubmed ↗
- 3Zhang Z. Chi J. Driskill E. Mont M. Jones L.C. Cui Q. Effect of patient age on total hip arthroplasty outcomes in patients who have osteonecrosis of the femoral head compared to patients who have hip osteoarthritis J. Arthroplast.2024391535154410.1016/j.arth.2023.12.02938135166 · doi ↗ · pubmed ↗
- 4Australian Orthopaedic Association National Joint Replacement Registry AOANJRR 2024 Annual Report Available online: https://aoanjrr.sahmri.com/annual-reports-2024(accessed on 9 April 2025)
- 5Bergh C. Fenstad A.M. Furnes O. Garellick G. Havelin L.I. Overgaard S. Pedersen A.B. MäkeläK.T. Pulkkinen P. Mohaddes M. Increased risk of revision in patients with non-traumatic femoral head necrosis Acta Orthop.201485111710.3109/17453674.2013.87492724359026 PMC 3940986 · doi ↗ · pubmed ↗
- 6Hart A. Janz V. Trousdale R.T. Sierra R.J. Berry D.J. Abdel M.P. Long-term survivorship of total hip arthroplasty with highly cross-linked polyethylene for osteonecrosis J. Bone Joint Surg. Am.20191011563156810.2106/JBJS.18.0121831483399 · doi ↗ · pubmed ↗
- 7Radl R. Hungerford M. Materna W. Rehak P. Windhager R. Higher failure rate and stem migration of an uncemented femoral component in patients with femoral head osteonecrosis than in patients with osteoarthrosis Acta Orthop.200576495510.1080/0001647051003031915788307 · doi ↗ · pubmed ↗
- 8Salman L.A. Hantouly A.T. Khatkar H. Al-Ani A. Abudalou A. Al-Juboori M. Ahmed G. The outcomes of total hip replacement in osteonecrosis versus osteoarthritis: A systematic review and meta-analysis Int. Orthop.2023473043305210.1007/s 00264-023-05761-636905418 PMC 10673986 · doi ↗ · pubmed ↗