[68Ga]-DOTATOC PET/CT Volumetric Parameters Reflect Metastatic Potential in Pancreatic Neuroendocrine Tumors
So Jeong Kim, Jongtae Cha, Hee Seung Lee, Moon Jae Chung, Jeong Youp Park, Seungmin Bang, Seung Woo Park, Si Young Song, Arthur Cho, Jung Hyun Jo

TL;DR
This study shows that [68Ga]-DOTATOC PET/CT can predict metastasis risk in pancreatic neuroendocrine tumors based on tumor volume and metabolic activity.
Contribution
The study demonstrates that volumetric PET/CT parameters correlate with metastatic potential in well-differentiated pancreatic neuroendocrine tumors.
Findings
Larger metabolically active tumors showed a higher incidence of metastasis.
Somatostatin receptor-expressing tumor volume and total lesion expression strongly correlate with metastasis (p < 0.001).
The findings may improve treatment decisions for patients with pancreatic neuroendocrine tumors.
Abstract
Determining the risk of metastasis in pancreatic neuroendocrine tumors is critical for guiding the most appropriate therapeutic approach. [68Ga]-DOTATOC PET/CT is a valuable technique for identifying pancreatic neuroendocrine tumors overexpressing somatostatin receptors and may provide insights into the biological behavior of pancreatic neuroendocrine tumors. We aimed to evaluate [68Ga]-DOTATOC uptake in well-differentiated pancreatic neuroendocrine tumors and determined its predictive capability for metastasis. Data from 48 patients with well-differentiated, non-functional pancreatic neuroendocrine tumors without accompanying genetic syndromes were analysed. A higher incidence of metastasis was observed in larger metabolically active tumors. Our findings may help clinicians make more precise treatment decisions, ultimately benefiting patients with pancreatic neuroendocrine tumors.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
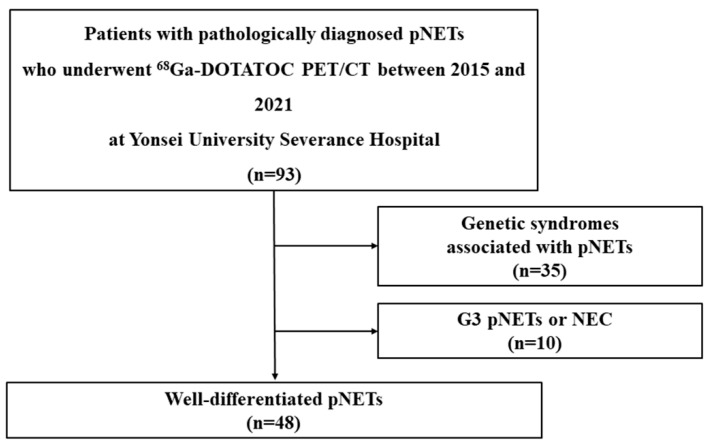 Figure 1
Figure 1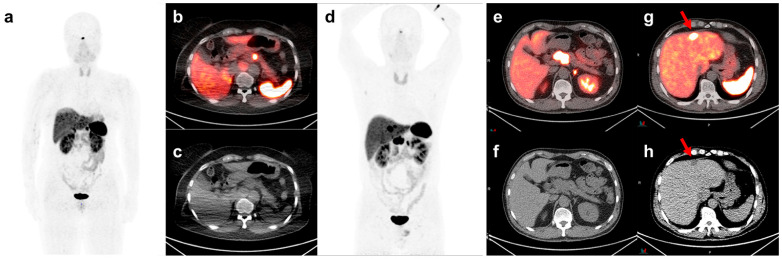 Figure 2
Figure 2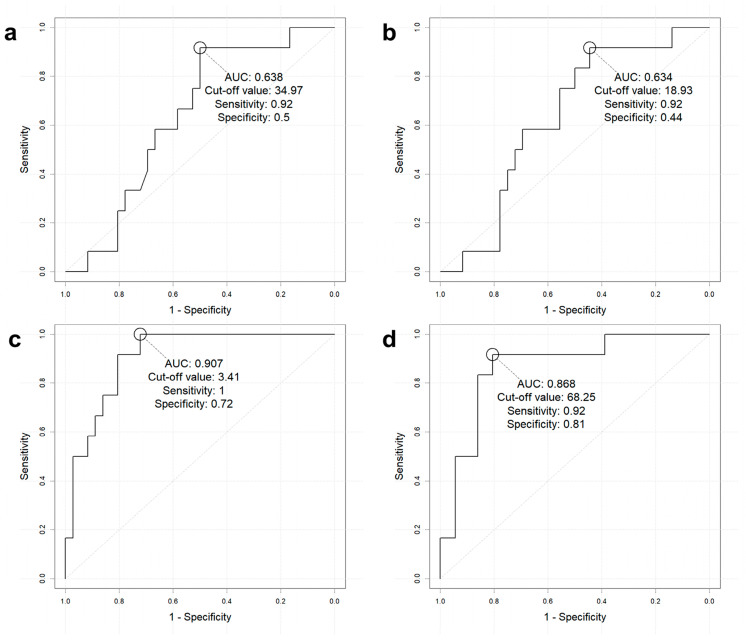 Figure 3
Figure 3- —National Research Foundation of Korea
- —Ministry of Education, Science and Technology
- —Yonsei University College of Medicine
- —Korea Health Industry Development Institute
- —Ministry of Health & Welfare, Republic of Korea
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroendocrine Tumor Research Advances · Medical Imaging Techniques and Applications · Neuroblastoma Research and Treatments
1. Introduction
Neuroendocrine tumors (NETs) are characterized by the overexpression of somatostatin receptors (SSTRs). Among the identified SSTRs, SSTR2, SSTR3, and SSTR5 are considered the most clinically relevant, given that most available SSTR analogs bind to these receptor subtypes [1,2,3]. This characteristic allows the use of radiolabeled somatostatin analogs in functional imaging of NETs [4,5,6]. Positron emission tomography/computed tomography (PET/CT) using [^68^gallium] labeled somatostatin analogues are replacing traditional ^111^indium pentetreotide scintigraphy owing to more favorable imaging characteristics for staging NETs, with the added advantage of evaluating therapeutic responses [7,8,9,10]. These PET somatostatin analogues have different affinities for SSTR and should be taken into account during radiotracer selection ([^68^Ga]-DOTATOC (SSTR 5), [^68^Ga]-DOTA-NOC (SSTR 3 and 5), and [^68^Ga]-DOTA-TATE (SSTR 2)) [11,12]. To determine the prognosis of patients with NETs, current semiquantitative methods used to estimate [^68^Ga]-DOTATOC uptake in primary tumors include maximum standard uptake value (SUVmax), mean standard uptake value (SUVmean), SSTR-expressing tumor volume (SRETV), and total lesion SSTR expression (TLSRE = SRETV × SUVmean), which have been found to effectively reflect NET characteristics and patient prognosis [13,14,15,16,17,18,19].
Pancreatic NET (pNET) has an exceptionally high risk of metastasis, with small lesions exhibiting a metastasis rate of approximately 15% [20,21,22]. Thus, predicting metastasis at diagnosis is crucial to improve patient prognosis. However, no known clinicopathologic or imaging indices can consistently identify the risk of metastasis in pNETs. Consequently, establishing a metastasis prediction system using [^68^Ga]-DOTATOC PET/CT imaging indices may be of clinical value. However, previous studies on pNETs and [^68^Ga]-DOTATOC PET/CT have predominantly focused on classifying tumors into World Health Organization (WHO) grades 1 (G1), 2 (G2), or 3 (G3). Given that discrepancies primarily occur in intermediate-grade cases, there is a need to further subdivide and assess tumor grades in [^68^Ga]-DOTATOC PET/CT imaging [10,13]. Despite these clinical needs, only a few studies have predicted the clinicopathological characteristics of subgroup pNETs using solely [^68^Ga]-DOTATOC PET/CT indices. Therefore, we aimed to determine whether [^68^Ga]-DOTATOC PET/CT indices correlate with the clinicopathologic factors in well-differentiated (WD) non-functional pNETs as classified according to the 2017 WHO classification of neuroendocrine neoplasms (NENs).
2. Materials and Methods
2.1. Patients and Study Design
The study protocol adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of Severance Hospital (IRB number: 4-2022-1331). Owing to the retrospective study design, the IRB waived the requirement for informed patient consent.
Patients with pathologically confirmed WD and non-functional pNET who underwent [^68^Ga]-DOTATOC PET/CT at Yonsei University Severance Hospital between 2015 and 2021 were included. Patients diagnosed with WHO G3, neuroendocrine carcinoma (NEC), and accompanying syndromes, such as multiple endocrine neoplasia type 1 and von Hippel-Lindau syndrome, were excluded.
We conducted a retrospective review of medical records and imaging data, focusing on clinicopathological factors and [^68^Ga]-DOTATOC PET/CT indices. Subsequently, we identified factors that exhibited a significant correlation between clinicopathological factors and imaging indices of [^68^Ga]-DOTATOC PET/CT.
2.2. Clinicopathologic Factors
We reviewed data from clinical records, including age and sex, as well as laboratory data, including serum chromogranin A and cancer antigen (CA 19-9) levels, when available. Tumor size was determined through surgical tissue and imaging analysis, including contrast-enhanced CT. Histopathological characteristics, including the 2017 WHO classification of NENs based on mitotic count and Ki-67 index, were confirmed, along with immunohistochemistry markers such as chromogranin A, cluster of differentiation 56 (CD56), and synaptophysin. Imaging studies, including contrast-enhanced CT, magnetic resonance imaging, and PET/CT, were performed to detect the presence of metastases.
2.3. PET/CT Imaging Protocol
PET/CT was performed using a PET/CT scanner (Discovery 710; GE Healthcare, Milwaukee, WI, USA) equipped with 128-slice CT. Prior to imaging, patients fasted for at least 8 h, and clinical charts were reviewed, confirming that no patient had received somatostatin treatment before PET/CT. One hour before image acquisition, [^68^Ga]-DOTATOC was administered intravenously at a dose of approximately 5.5 MBq/kg of body weight. After the initial low-dose CT study (60 mA, 120 kVp), a standard PET protocol was used for scanning from the neck to the proximal thighs, with an acquisition time of 3 min per bed per position in the three-dimensional mode. Images were reconstructed using ordered subset expectation maximization (2 iterations, 16 subsets), and a Gaussian filter of 5-mm FWHM was applied.
2.4. [68Ga]-DOTATOC PET/CT Analysis
Two experienced nuclear medicine physicians reviewed all PET/CT images using MIM version 7.08 (MIM Software Inc., Cleveland, OH, USA). A spherical volume of interest (VOI) encasing the entire primary tumor was drawn, and a relative threshold of 41% of the SUVmax of the primary tumor was used to define the SRETV. This approach followed the recommendations of the EANM guidelines [23], and the resulting VOIs were considered to reasonably approximate the actual tumor volume. TLSRE was calculated as follows: SRETV × SUVmean.
2.5. Statistical Analysis
Normality was checked by the Shapiro–Wilk test for the continuous variables. Descriptive statistics were represented as mean ± SD for the normality-passed variables or median (interquartile range) for the other variables. Variables with normal distributions were analyzed using the Student’s t-test, while non-normally distributed variables were analyzed using the Mann–Whitney U test. Clinical data from patients’ samples were analyzed using the χ^2^ and Fisher’s exact tests for categorical data. Spearman’s rank correlation was performed to evaluate the relationship between [^68^Ga]-DOTATOC PET/CT indices and clinicopathologic factors. Receiver operating characteristic (ROC) curve analysis was performed to determine the best cut-off value for predicting metastasis. The Youden index (J) was used to determine the cut-off point. All statistical analyses were performed using IBM SPSS Statistics for Windows, version 26.0 (IBM Corp., Armonk, NY, USA). p < 0.05 was considered statistically significant.
3. Results
3.1. Patient Demographics
In total, 93 patients with pathologically diagnosed pNETs who underwent [^68^Ga]-DOTATOC PET/CT at our institution between 2015 and 2021 were identified. Among these patients, those with genetic syndromes associated with pNETs (n = 35) and G3 pNETs or NEC (n = 10) were excluded. Finally, 48 patients with WD pNETs were enrolled in our study (Figure 1).
3.2. Clinicopathologic Factors and [68Ga]-DOTATOC PET/CT Indices According to the Initial Metastasis of pNETs
A total of 48 patients with WD pNETs were enrolled (mean age, 54.81 ± 12.19 years; 27 male patients [56.3%]). Initial metastases were detected in 12 patients (25%) (Table 1). In the non-metastatic group, tumors in most patients (94.4%) were confirmed histologically via surgery, whereas in the metastatic group, tumors in most patients (75.0%) were confirmed via endoscopic ultrasonography fine needle biopsy (p < 0.001). Based on laboratory assessments, the metastatic group had higher levels of chromogranin A and CA 19-9 than those in the non-metastatic group, although the difference was non-significant. The metastatic group had significantly larger tumors than the non-metastatic group (34.50 (27.00–40.00) vs. 14.50 (11.00–20.00) mm, p < 0.001). Importantly, the metastatic group had a significantly higher proportion of patients with a tumor size of ˃20 mm than the non-metastatic group (91.7% vs. 19.4%, p < 0.001). The proportion of G2 tumors and the Ki-67 index, reflecting the tumor grade, were higher in the metastatic group than in the non-metastatic group (75% vs. 25%, p = 0.002; 4.90 (2.36–12.00) vs. 1.49 (0.92–2.43), p = 0.002). The immunohistochemistry findings, including chromogranin A, CD56, and synaptophysin staining, did not differ significantly between groups (all p > 0.05).
To evaluate the difference in SSTR expression between the metastatic and non-metastatic groups, we compared the mean values of SUVmax and SUVmean, which are linked to the concentration of SSTR-bound [^68^Ga]-DOTATOC, along with SRETV and TLSRE, which are conventionally used to evaluate SSTR-expressing tumor volume. Although no significant differences in SUVmax and SUVmean were detected, the metastasis group exhibited higher SRETV and TLSRE values than the non-metastasis group (11.80 (6.02–16.01) vs. 1.50 (0.84–3.78), p < 0.001; 357.14 (290.16–538.25) vs. 41.29 (16.94–67.10), p < 0.001, respectively). A representative case is presented in Figure 2.
3.3. Diagnostic Performance of [68Ga]-DOTATOC PET/CT Indices to Predict Initial Metastasis
To evaluate the clinical usefulness of [^68^Ga]-DOTATOC PET/CT indices in predicting initial metastasis, an ROC curve analysis was performed (Figure 3). ROC-generated cut-offs of SUVmax > 34.97, SUVmean > 18.93, SRETV > 3.41, and TLSRE > 68.25 were used to evaluate diagnostic performance in predicting initial metastasis.
Overall, SUVmax and SUVmean showed a similar area under the curve (AUC), high sensitivity (both 91.7% (11/12)), and negative predictive value (NPV) (94.7% (18/19), 94.1% (16/17), respectively; Table 2). Conversely, PET metrics incorporating volume showed a higher AUC than SUVmax and SUVmean (SRETV: AUC 90.7%, TLSRE: 86.8%), along with higher sensitivity (SRETV: 100%, TLSRE: 91.7%, respectively) and higher NPV (SRETV: 100%, TLSRE: 96.7%).
3.4. Subgroup Analysis of [68Ga]-DOTATOC PET/CT Indices to Predict Metastasis in pNETs Measuring > 20 mm
In our patient population, CT-measured tumor size with a cut-off value of >20 mm showed high sensitivity (91.7%) and high specificity (80.6%) in predicting metastasis (Table 1). However, 7 out of 18 patients (38.9%) with tumors ˃20 mm did not have metastasis, indicating the clinical limitations of using surgical resection based on size criteria alone. Moreover, PET indices showed comparable sensitivity (91.7%) to the CT-measured tumor size in predicting metastasis. Importantly, we found that the accuracy of all PET indices ranged between 72.2% and 77.8% in terms of predicting metastasis of tumors ˃20 mm (Table 2). In tumors ˃20 mm, SRETV presented the highest accuracy (77.8%; 14/18) in predicting metastasis, accompanied by a sensitivity of 100% (11/11) when using the same cut-off of 3.41 cm^3^. Compared to SRETV, TLSRE miscategorized one metastasis (Table 2). Other PET indices revealed similar accuracy but lower sensitivity than SRETV.
3.5. Clinicopathologic Factors and [68Ga]-DOTATOC Indices According to pNET WHO Grades
Among the 48 patients, the tumors in 30 (62.5%) and 18 (37.5%) were categorized as WHO G1 and G2, respectively (Table 3). The G1 pNET group comprised a higher proportion of male individuals than the G2 pNET group (G1 vs. G2: 70.0% vs. 33.3%, p = 0.013). Additionally, a higher proportion of patients in the G1 pNET group underwent surgery for histologic confirmation than that in the G2 pNET group (G1 vs. G2: 90.0% vs. 55.6%, p = 0.006). The G2 pNET group had larger tumors (13.00 [11.00–20.00] vs. 23.50 (18.00–35.00), p = 0.002) and exhibited metastasis more frequently than the G1 pNET group (10.0% vs. 50.0%, p = 0.005). There were no differences between the G1 and G2 pNET groups in laboratory test results or immunohistochemistry findings (serum levels of chromogranin A, CA 19-9, CD56, and synaptophysin, all p > 0.05). Upon evaluating [^68^Ga]-DOTATOC PET/CT indices, no significant differences in SUVmax, SUVmean, SRETV, and TLSRE were detected between the G1 and G2 pNET groups.
3.6. Relationship Between [68Ga]-DOTATOC PET/CT Indices, Proliferative Index, and Serum Markers
Considering that [^68^Ga]-DOTATOC targets somatostatin expression, a higher uptake should reflect more functional tumors. Therefore, to evaluate which [^68^Ga]-DOTATOC indices best reflect tumor function, we performed a Spearman’s rank correlation analysis of known clinicopathological variables that reflect pNET function (Table 4). As summarized in Table 4, none of the [^68^Ga]-DOTATOC-derived indices demonstrated a statistically significant correlation with mitotic count, Ki-67 index, chromogranin A level, or CA 19-9. Although SRETV showed a weak positive correlation with Ki-67 (rho = 0.263, p = 0.071), this did not reach statistical significance.
4. Discussion
To the best of our knowledge, this is the first study to evaluate the relationship between volumetric [^68^Ga]-DOTATOC PET/CT indices and the presence of initial metastasis in patients with pNETs. Initial metastasis was more accurately predicted by the volume of SSTR-expressing tumors than by the degree of SSTR expression alone. Unlike SUVmax and SUVmean, which reflect only peak or average uptake in localized regions, PET indices such as SRETV and TLSRE reflect both tumor size and function, and has the added advantage of summation of multiple lesions. This allows for a more comprehensive assessment of total tumor burden and is in line with previous reports indicating that only volumetric PET/CT parameters were significantly associated with prognosis [19,24].
We obtained evidence to support the application of non-invasive methods such as [^68^Ga]-DOTATOC PET/CT in patients with WD pNETs to predict initial metastasis. Detecting the presence of metastasis is crucial in determining the treatment strategy for pNETs. A higher rate of metastasis is generally associated with unfavorable pathological characteristics, such as higher grades and larger tumors. However, in the present study, we observed that 25% of patients with WD pNETs had metastasis at diagnosis. Although patients with WHO G2 tumors showed higher rates of metastasis than those with G1, approximately 10% of patients with G1 pNETs also had metastatic lesions, including one patient (8.3%) with a tumor size of ≤20 mm. These findings are concordant with those of previous studies [25,26], where 20–40% of all patients with pNETs were found to present with metastases at diagnosis, including those with WD pNETs < 20 mm [25,26]. Thus, there is a clinical unmet need to predict metastasis in pNETs, especially WD tumors. We demonstrated that the accuracy of SRETV is comparable to that of size criteria in predicting metastasis but with higher sensitivity (100% vs. 91.7%) and lower specificity (72.2% vs. 80.6%). However, more importantly, we found that in tumors ˃20 mm, the accuracy and sensitivity of SRETV were as high as 77.8% and 100%, respectively, in predicting metastasis, potentially suggesting an additional role of [^68^Ga]-DOTATOC PET/CT in predicting metastasis of lesions ˃20 mm. Current guidelines suggest that pNETs > 20 mm should be resected owing to the higher metastatic potential, regardless of the tumor grade [27]; therefore, this approach is valuable in identifying advanced cases because the current consensus for treatment is based solely on size criteria in localized pNETs. Further prospective studies are needed to validate the findings of the present study.
Tirosh et al. reported that the [^68^Ga]-DOTA-avid tumor volume positively correlated with NET biomarker levels [28]. [^68^Ga]-DOTATOC PET/CT may be a valuable technique for estimating the functional tumor burden, given the lack of clinical indices that correlate with elevated serum chromogranin A level in patients with pNETs. However, in our study, no significant correlations were observed. This discrepancy may be attributed to differences in patient population and the limited sample size. Further studies with larger cohorts would be encouraged.
This study has some limitations. First, this was a retrospective study conducted in a single institution; hence, selection bias is inevitable. However, we included a relatively homogenous patient population encompassing those who had pathologically confirmed G1/G2 WD pNETs. In the future, investigations comprising a larger patient cohort need to be undertaken. Second, owing to the retrospective nature of this study, some patients had missing measurement data, such as the proliferative index and serum marker levels, which may have led to limited outcomes. Lastly, although a higher proportion of male patients was observed in the G1 group, this likely reflects a sampling imbalance given the limited number of G2 patients. Previous studies have not demonstrated a consistent association between patient gender and [^68^Ga]-DOTATOC uptake in tumor lesions, suggesting this difference does not confound our imaging-based findings [23].
5. Conclusions
Volumetric [^68^Ga]-DOTATOC PET/CT indices, such are SRETV and TLSRE, have added value in predicting initial metastasis in WD pNETs, whereas SUVmax and SUVmean did not. Our findings suggest that patients with larger WD pNETs tumors will benefit from PET/CT in metastasis detection and have an additional role for functional imaging biomarkers in guiding treatment decisions beyond size-based criteria alone.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Oda Y. Tanaka Y. Naruse T. Sasanabe R. Tsubamoto M. Funahashi H. Expression of somatostatin receptor and effects of somatostatin analog on pancreatic endocrine tumors Surg. Today 20023269069410.1007/s 00595020012812181718 · doi ↗ · pubmed ↗
- 2Papotti M. Bongiovanni M. Volante M. Allìa E. Landolfi S. Helboe L. Schindler M. Cole S.L. Bussolati G. Expression of somatostatin receptor types 1–5 in 81 cases of gastrointestinal and pancreatic endocrine tumors. A correlative immunohistochemical and reverse-transcriptase polymerase chain reaction analysis Virchows Arch.200244046147510.1007/s 00428-002-0609-x 12021920 · doi ↗ · pubmed ↗
- 3Zilli A. Fanetti I. Conte D. Massironi S. A case of positive (68)Ga-DOTATOC-PET/CT pancreatic heterotopia mimicking an intestinal neuroendocrine tumor Clin. Imaging 20184915615810.1016/j.clinimag.2018.03.00129529451 · doi ↗ · pubmed ↗
- 4Reubi J.C. Neuropeptide receptors in health and disease: The molecular basis for in vivo imaging J. Nucl. Med.199536182518357562050 · pubmed ↗
- 5Reubi J.C. Schär J.C. Waser B. Wenger S. Heppeler A. Schmitt J.S. Mäcke H.R. Affinity profiles for human somatostatin receptor subtypes SST 1-SST 5 of somatostatin radiotracers selected for scintigraphic and radiotherapeutic use Eur. J. Nucl. Med.20002727328210.1007/s 00259005003410774879 · doi ↗ · pubmed ↗
- 6Miederer M. Seidl S. Buck A. Scheidhauer K. Wester H.J. Schwaiger M. Perren A. Correlation of immunohistopathological expression of somatostatin receptor 2 with standardised uptake values in 68Ga-DOTATOC PET/CT Eur. J. Nucl. Med. Mol. Imaging 200936485210.1007/s 00259-008-0944-518807033 · doi ↗ · pubmed ↗
- 7Tamm E.P. Bhosale P. Lee J.H. Rohren E.M. State-of-the-art Imaging of Pancreatic Neuroendocrine Tumors Surg. Oncol. Clin. N. Am.20162537540010.1016/j.soc.2015.11.00727013371 PMC 4808582 · doi ↗ · pubmed ↗
- 8Ambrosini V. Campana D. Polverari G. Peterle C. Diodato S. Ricci C. Allegri V. Casadei R. Tomassetti P. Fanti S. Prognostic Value of 68Ga-DOTANOC PET/CT SU Vmax in Patients with Neuroendocrine Tumors of the Pancreas J. Nucl. Med.2015561843184810.2967/jnumed.115.16271926405169 · doi ↗ · pubmed ↗