The Impact of Omicron-related Stress on Mental Health in the General Population of China
WenYan Zhao, YuLiang Zhou, YingYing Hu, Jing Wang, Hong Zhu, YaHong Li, ZhiPeng Xu

TL;DR
This study found that Omicron-related stress significantly worsened mental health in China's general population, especially among those infected and with low resilience.
Contribution
The study identifies specific demographic and Omicron-related risk factors for mental health issues during the Omicron wave in China.
Findings
High prevalence of anxiety (52%), depression (58.3%), insomnia (45.2%), and acute stress disorder (34.8%) was observed.
Infection during Omicron increased risks for anxiety, depression, insomnia, and acute stress disorder.
Lower resilience was strongly linked to higher mental health symptom risks.
Abstract
Outbreaks of infectious disease represent unique stressors for the general population. In this study, we investigated the prevalence of mental health symptoms and associated risk factors in the general population of China during the Omicron wave. We conducted a cross-sectional and large sample online survey during the surge of Omicron cases between 17 December 2022 and 8 January 2023 among Chinese citizens. Then we assessed the prevalence of symptoms of anxiety, depression, insomnia, acute stress disorder, and resilience levels, in the general population of China during the Omicron pandemic by utilizing the coronavirus disease 2019 (COVID-19) anxiety scale (CAS), the Center for Epidemiologic Studies Depression Scale (CES-D), the Insomnia Severity Index scale (ISI), the Stanford Acute Stress Reaction Questionnaire (SASRQ), and the Connor-Davidson Resilience Scale (CD-RISC). Multivariate…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
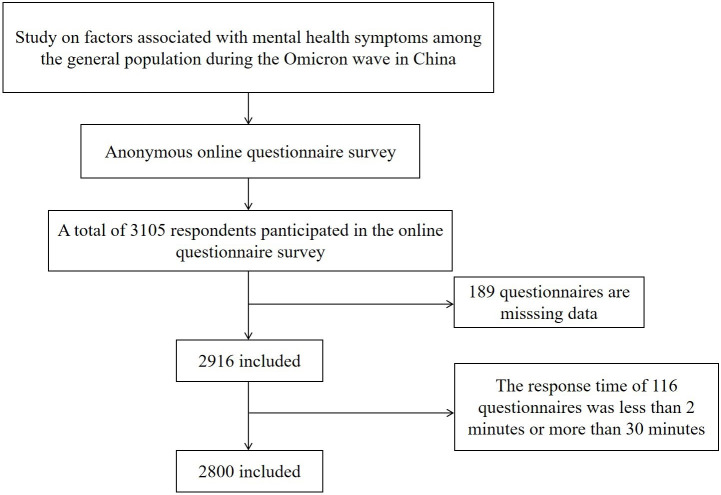 Fig. 1
Fig. 1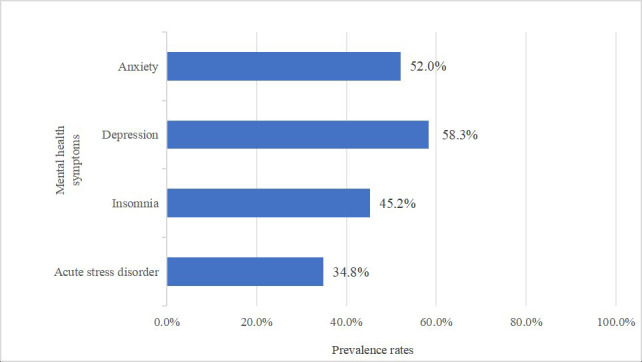 Fig. 2
Fig. 2| Factors | Respondents, number (%) | |
| Overall | 2800 (100.0) | |
| Gender | ||
| Male | 1133 (40.5) | |
| Female | 1667 (59.5) | |
| Age | ||
| 1860 (66.4) | ||
| 940 (33.6) | ||
| Marital status | ||
| Unmarried | 887 (31.7) | |
| Married | 1913 (68.3) | |
| Level of education | ||
| Lower than bachelor’s degree | 497 (17.8) | |
| Bachelor’s degree | 1480 (52.9) | |
| Master’s degree or above | 823 (29.4) | |
| Occupation | ||
| Medical workers | 1401 (50.0) | |
| Public institutions or administrative personnel | 293 (10.5) | |
| Commerce occupations | 251 (9.0) | |
| Students | 314 (11.2) | |
| Others | 541 (19.3) | |
| Annual income, CNY | ||
| 50,000 or less | 662 (23.6) | |
| 50,000–100,000 | 900 (32.1) | |
| 110,000–200,000 | 809 (28.9) | |
| 200,000 or more | 429 (15.3) | |
| History of chronic diseases | ||
| Yes | 301 (10.8) | |
| No | 2499 (89.3) | |
| What is your current status with COVID-19? | ||
| Uninfected | 672 (24.0) | |
| In the course of an infection | 1230 (43.9) | |
| Recovered | 898 (32.1) | |
| What are your symptoms after COVID-19 infection? | ||
| Fever | 1799 (64.3) | |
| Headache | 1564 (55.9) | |
| General pain and weakness | 1597 (57.0) | |
| Sore throat | 1544 (55.1) | |
| Nasal congestion and runny nose | 1488 (53.1) | |
| Cough | 1817 (64.9) | |
| Expectoration | 1462 (52.2) | |
| Dyspnea | 252 (9.0) | |
| Diminished or lost sense of taste | 853 (30.5) | |
| Reduced or lost sense of smell | 634 (22.6) | |
| Have any of your family members recently been infected with COVID-19? | ||
| Yes | 2205 (78.8) | |
| No | 595 (21.3) | |
| Are there COVID-19 patients in your work environment? | ||
| Yes | 2607 (93.1) | |
| No | 193 (6.9) | |
| How many doses of COVID-19 vaccine have you received? | ||
| 0 | 66 (2.4) | |
| 1 | 36 (1.3) | |
| 2 | 465 (16.6) | |
| 3 | 2089 (74.6) | |
| 4 | 144 (5.1) | |
| Anxiety | ||
| CAS | 1344 (48.0) | |
| CAS | 1456 (52.0) | |
| Depression | ||
| CES-D | 1169 (41.8) | |
| CES-D | 1631 (58.3) | |
| Insomnia | ||
| ISI | 1534 (54.8) | |
| ISI | 1266 (45.2) | |
| Acute stress disorder (ASD) | ||
| SASRQ | 1825 (65.2) | |
| SASRQ | 975 (34.8) | |
| Resilience | ||
| Low resilience ( | 914 (32.6) | |
| Medium resilience (2nd to 4th quartile) | 775 (27.7) | |
| High resilience ( | 1111 (39.7) | |
| Dependent variables | Independent variables | Reference |
| S.E. | Wald | OR | 95% CI |
|
| Anxiety | Gender | Male | 0.50 | 0.08 | 35.23 | 1.64 | 1.39–1.94 | |
| Age | 0.13 | 0.09 | 1.84 | 1.13 | 0.95–1.36 | 0.175 | ||
| Level of education | Master degree or above | |||||||
| Lower than bachelor’s degree | 0.11 | 0.14 | 0.68 | 1.12 | 0.86–1.47 | 0.410 | ||
| Bachelor’s degree | 0.04 | 0.10 | 0.14 | 1.04 | 0.86–1.25 | 0.713 | ||
| Occupation | Medical workers | |||||||
| Public institutions or administrative personnel | 0.37 | 0.14 | 7.13 | 1.44 | 1.10–1.88 | 0.008 | ||
| Commerce occupations | 0.58 | 0.16 | 14.02 | 1.79 | 1.32–2.43 | |||
| Students | −0.09 | 0.17 | 0.29 | 0.91 | 0.66–1.27 | 0.593 | ||
| Others | 0.17 | 0.11 | 2.02 | 1.18 | 0.94–1.47 | 0.156 | ||
| Annual income, CNY | 200,000 or more | |||||||
| 50,000 or less | 0.59 | 0.17 | 12.22 | 1.80 | 1.30–2.50 | |||
| 50,000–100,000 | 0.57 | 0.14 | 16.87 | 1.76 | 1.34–2.30 | |||
| 110,000–200,000 | 0.49 | 0.13 | 14.08 | 1.64 | 1.27–2.11 | |||
| What is your current status with COVID-19? | Uninfected | |||||||
| In the course of an infection | 0.24 | 0.11 | 4.83 | 1.27 | 1.03–1.57 | 0.028 | ||
| Recovered | 0.15 | 0.12 | 1.61 | 1.16 | 0.92–1.46 | 0.204 | ||
| Have any of your family members recently been infected with COVID-19? | No | 0.13 | 0.17 | 0.65 | 1.14 | 0.83–1.58 | 0.420 | |
| How many doses of COVID-19 vaccine have you received? | 4 | |||||||
| 0 | 0.03 | 0.31 | 0.01 | 1.03 | 0.56–1.91 | 0.922 | ||
| 1 | 0.30 | 0.40 | 0.55 | 1.34 | 0.62–2.94 | 0.459 | ||
| 2 | 0.15 | 0.21 | 0.54 | 1.16 | 0.78–1.73 | 0.464 | ||
| 3 | 0.12 | 0.19 | 0.40 | 1.12 | 0.78–1.62 | 0.530 | ||
| Resilience | High resilience ( | |||||||
| Low resilience ( | 0.85 | 0.10 | 78.89 | 2.33 | 1.94–2.81 | |||
| Medium resilience (2nd to 4th quartile) | 0.66 | 0.10 | 45.70 | 1.94 | 1.60–2.35 |
| Dependent variables | Independent variables | Reference |
| S.E. | Wald | OR | 95% CI |
|
| Depression | Gender | Male | 0.24 | 0.09 | 7.59 | 1.27 | 1.07–1.50 | 0.006 |
| Age | 0.40 | 0.10 | 16.26 | 1.49 | 1.23–1.82 | |||
| Marital status | Married | −0.26 | 0.12 | 5.14 | 1.30 | 1.04–1.64 | 0.023 | |
| Occupation | Medical workers | |||||||
| Public institutions or administrative personnel | 0.49 | 0.14 | 12.19 | 1.64 | 1.24–2.16 | |||
| Commerce occupations | 0.54 | 0.15 | 12.34 | 1.72 | 1.27–2.32 | |||
| Students | 0.34 | 0.18 | 3.83 | 1.43 | 1.00–2.05 | 0.050 | ||
| Others | 0.09 | 0.11 | 0.71 | 1.10 | 0.88–1.36 | 0.399 | ||
| Annual income, CNY | 200,000 or more | |||||||
| 50,000 or less | −0.11 | 0.17 | 0.44 | 0.89 | 0.64–1.25 | 0.507 | ||
| 50,000–100,000 | −0.17 | 0.13 | 1.60 | 0.85 | 0.65–1.10 | 0.205 | ||
| 110,000–200,000 | −0.04 | 0.13 | 0.07 | 0.97 | 0.75–1.25 | 0.789 | ||
| What is your current status with COVID-19? | Uninfected | |||||||
| In the course of an infection | 0.57 | 0.10 | 29.74 | 1.76 | 1.44–2.16 | |||
| Recovered | 0.15 | 0.11 | 1.88 | 1.16 | 0.94–1.45 | 0.171 | ||
| How many doses of COVID-19 vaccine have you received? | 4 | |||||||
| 0 | 0.22 | 0.32 | 0.49 | 1.25 | 0.67–2.34 | 0.483 | ||
| 1 | 1.11 | 0.46 | 6.01 | 3.05 | 1.25–7.43 | 0.014 | ||
| 2 | 0.21 | 0.21 | 1.05 | 1.24 | 0.83–1.85 | 0.305 | ||
| 3 | 0.19 | 0.19 | 1.04 | 1.21 | 0.84–1.74 | 0.308 | ||
| Resilience | High resilience ( | |||||||
| Low resilience ( | 1.19 | 0.10 | 143.41 | 3.28 | 2.70–3.98 | |||
| Medium resilience (2nd to 4th quartile) | 0.79 | 0.10 | 63.87 | 2.21 | 1.82–2.67 |
| Dependent variables | Independent variables | Reference |
| S.E. | Wald | OR | 95% CI |
|
| Insomnia | Age | 0.05 | 0.10 | 0.22 | 1.05 | 0.86–1.28 | 0.636 | |
| Marital status | Married | 0.25 | 0.11 | 4.67 | 1.28 | 1.02–1.60 | 0.031 | |
| Level of education | Master degree or above | |||||||
| Lower than bachelor’s degree | 0.21 | 0.14 | 2.19 | 1.23 | 0.94–1.61 | 0.139 | ||
| Bachelor degree | 0.29 | 0.10 | 8.74 | 1.33 | 1.10–1.62 | 0.003 | ||
| Occupation | Medical workers | |||||||
| Public institutions or administrative personnel | 0.36 | 0.14 | 6.95 | 1.44 | 1.10–1.88 | 0.008 | ||
| Commerce occupations | 0.42 | 0.15 | 7.44 | 1.52 | 1.13–2.05 | 0.006 | ||
| Students | −0.34 | 0.18 | 3.68 | 0.72 | 0.51–1.01 | 0.055 | ||
| Others | 0.05 | 0.11 | 0.20 | 1.05 | 0.84–1.32 | 0.652 | ||
| Annual income, CNY | 200,000 or more | |||||||
| 50,000 or less | 0.08 | 0.17 | 0.24 | 1.09 | 0.78–1.52 | 0.626 | ||
| 50,000–100,000 | 0.02 | 0.14 | 0.03 | 1.02 | 0.78–1.34 | 0.872 | ||
| 110,000–200,000 | −0.10 | 0.13 | 0.02 | 0.98 | 0.76–1.27 | 0.888 | ||
| What is your current status with COVID-19? | Uninfected | |||||||
| In the course of an infection | 0.67 | 0.11 | 36.49 | 1.95 | 1.57–2.42 | |||
| Recovered | −0.00 | 0.12 | 0.00 | 1.00 | 0.79–1.26 | 0.962 | ||
| Have any of your family members recently been infected with COVID-19? | No | 0.10 | 0.11 | 0.86 | 1.11 | 0.89–1.37 | 0.354 | |
| Resilience | High resilience ( | |||||||
| Low resilience ( | 1.22 | 0.10 | 155.54 | 3.38 | 2.79–4.09 | |||
| Medium resilience (2nd to 4th quartile) | 0.70 | 0.10 | 48.80 | 2.00 | 1.65–2.44 |
| Dependent variables | Independent variables | Reference |
| S.E. | Wald | OR | 95% CI |
|
| Acute stress disorder | Gender | Male | 0.10 | 0.09 | 1.19 | 1.11 | 0.92–1.32 | 0.276 |
| Age | 0.08 | 0.11 | 0.48 | 1.08 | 0.87–1.33 | 0.487 | ||
| Marital status | Married | 0.05 | 0.12 | 0.21 | 1.06 | 0.84–1.33 | 0.651 | |
| Level of education | Master degree or above | |||||||
| Lower than bachelor’s degree | −0.14 | 0.15 | 0.88 | 0.87 | 0.65–1.16 | 0.347 | ||
| Bachelor’s degree | 0.04 | 0.11 | 0.15 | 1.04 | 0.85–1.28 | 0.697 | ||
| Occupation | Medical workers | |||||||
| Public institutions or administrative personnel | 0.36 | 0.15 | 5.84 | 1.43 | 1.07–1.91 | 0.016 | ||
| Commerce occupations | 0.79 | 0.16 | 23.40 | 2.20 | 1.60–3.02 | |||
| Students | 0.09 | 0.18 | 0.26 | 1.10 | 0.77–1.56 | 0.609 | ||
| Others | 0.20 | 0.12 | 2.72 | 1.22 | 0.96–1.56 | 0.099 | ||
| Annual income, CNY | 200,000 or more | |||||||
| 50,000 or less | 0.66 | 0.19 | 12.55 | 1.94 | 1.34–2.79 | |||
| 50,000–100,000 | 0.36 | 0.15 | 5.62 | 1.44 | 1.07–1.94 | 0.018 | ||
| 110,000–200,000 | 0.26 | 0.15 | 3.05 | 1.30 | 0.97–1.73 | 0.081 | ||
| What is your current status with COVID-19? | Uninfected | |||||||
| In the course of an infection | 0.44 | 0.11 | 15.97 | 1.56 | 1.25–1.93 | 0.001 | ||
| Recovered | 0.00 | 0.12 | 0.00 | 1.00 | 0.79–1.27 | 0.986 | ||
| Resilience | High resilience ( | |||||||
| Low resilience ( | 1.73 | 0.11 | 262.57 | 5.64 | 4.58–6.96 | |||
| Medium resilience (2nd to 4th quartile) | 0.96 | 0.09 | 74.09 | 2.61 | 2.10–3.24 |
- —key research and development program of Hubei Province
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and Mental Health · Long-Term Effects of COVID-19 · Mental Health Research Topics
Introduction
Coronavirus disease 2019 (COVID-19) was a pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [1]. According to the World Health Organization (WHO), more than 656 million confirmed cases and more than 6.6 million deaths had been reported worldwide as of 1 January 2019 (WHO). This public health emergency considerably impacted the mental health of the population, resulting in varying degrees of anxiety, depression, insomnia, and other aspects of psychological distress [2, 3]. The mental health issues caused by COVID-19 have gained increasing attention. Early in the pandemic, a study of the general population in China found that patients with COVID-19 had a higher prevalence of mental health symptoms—such as anxiety, depression, suicidal ideation, and insomnia—compared to those who were not infected [4].
Over the past three years, new mutant strains of COVID-19 have emerged. The Omicron variant was first discovered in South Africa in November 2021 [5]. As of 2024, Omicron remains one of the most dominant variants of COVID-19 globally [6]. During the third year of the COVID-19 pandemic, the National Health Commission of China gradually changed the COVID-19 testing strategy in response to the specific epidemiological trend. It is not surprising that the general population is experiencing severe psychological distress in response to this major public health infection [7]. However, there is significant variation in how subjects respond to challenges and difficulties; furthermore, not all infected subjects develop symptoms of anxiety, depression, insomnia, and acute stress disorder. Psychological resilience represents a protective mechanism that can help subjects to maintain a good mental state following traumatic events [8]. However, there has been no specific investigation of how Omicron can result in mental health problems and the resilience of these subjects in the Chinese general population. Therefore, in the present study we conducted an online survey to investigate the psychological distress and factors influencing mental health in the Chinese general population during the Omicron pandemic. Our aim was to provide a theoretical basis and direction for targeted mental health guidance and interventions within the health sector. Our findings highlight the importance of Omicron as a relevant stressor on the psychological status of the general population and will help to understand the complexity of mental health in the context of an epidemic.
Methods
Study Design
This cross-sectional online study was conducted between 17 December 2022 and 8 January 2023. Data were collected anonymously through “Survey Star”, an online survey platform managed by Shanghai Changsha Science & Technology. This study was approved by the Ethics Committee of Zhongnan Hospital of Wuhan University (Ref. Number: 2022116K).
Participants and Data Collection
A total of 3105 respondents participated in the online psychological questionnaire-based survey and provided measures of socio-demographic information and psychological distress (anxiety, depression, sleep state, acute stress disorder, and mental resilience). The inclusion criteria were as follows: (1) Chinese residents living in mainland China during the Omicron epidemic; (2) 16 to 80 years-of-age. Participants who responded for 2 minutes or 30 minutes were excluded to ensure that the questionnaires were good quality. After excluding invalid questionnaires, 2800 participants were included in the analysis.
Demographic Information
A socio-demographic questionnaire was designed to collect a range of important data from each respondent, including age, gender, marital status, educational level, annual income, residence, chronic medical history, personal and family COVID-19 infection status, post-infection symptoms, working environment, and vaccination status.
Mental Health Status Scales
The COVID-19 anxiety scale (CAS) was developed to evaluate the specific COVID-19 anxiety caused by the pandemic scenario. Each item is rated on a 4-point scale to reflect the frequency of the symptom, ranging from 0 (not applicable to me) to 3 (very applicable to me) over the past few days. The higher the total score, the higher the level of anxiety relating to COVID-19. Previous studies showed that the seven items of the CAS represent a rapidly administered, valid, and reliable instrument that can be used to measure COVID‑19‑related anxiety [9]. According to the five points of the Generalized Anxiety Disorder-7 (GAD-7) scale (mild degree), the cutoff score is 10 points for the CAS-7 [10].
The Center for Epidemiologic Studies Depression Scale (CES-D) is a widely used instrument for measuring depressive symptoms. This is a self-rating scale that is used to investigate the frequency of depressive symptoms experienced by a subject during the previous week. A total of 10 items were scored on a scale of 0 (little or no) to 3 (most or all of the time) (items 5 and 8 were reverse scores). The suggested cutoff score for clinically probable depression is 10 [11].
The Insomnia Severity Index scale (ISI) is a 7-item self-report assessment for the severity of insomnia symptoms, the impact of sleep interference on daily activities, and the concern caused by sleep problems. Scores of 0–7 are classified as non-clinical insomnia, 8–14 as subclinical insomnia, 15–21 as clinical insomnia (moderate), and 22–28 as clinical insomnia (severe) [12].
The Stanford Acute Stress Reaction Questionnaire (SASRQ) was developed by Cardeña et al. [13] to evaluate mental health symptoms in the aftermath of traumatic events. The 30 items of the SASRQ included dissociative symptoms (10 items), continuous re-experience of traumatic events (6 items), avoidance of traumatic events (6 items), high alertness symptoms (6 items), and social function impairment (2 items). Each item is rated on a scale of 6 from 0 to 5. A score of 0 represents “no experience” while a score of 5 represents “always experience” on a scale of 150. A total SASRQ score of 40 was used as a criterion for the occurrence of acute stress disorder (ASD); the higher the score, the more severe the ASD symptoms [14]. This study was conducted by psychiatrists specializing in neurology and psychiatry, who diagnosed ASD based on the clinical presentation of a given patient and scoring criteria.
The Connor-Davidson Resilience Scale (CD-RISC) has been widely used and has good reliability and validity in different populations. The 10-item Connor-Davidson Resilience Scale-10 (CD-RISC-10) is an abbreviated CD-RISC version that is used to efficiently measure resilience that yielded excellent psychometric properties when applied in the original English version. Each item is scored on a 5-point scale of 0–4 points (never = 0, rarely = 1, sometimes = 2, often = 3, almost always = 4). The higher the total score, the better the psychological resilience of the subject [15, 16]. This scale lacks a cutoff point; therefore, we divided this scale into three sub-groups: high resilience (score 4th quartile), medium resilience (2nd to 4th quartile), and low resilience (score 1st quartile) [17].
Statistical Analysis
Descriptive statistics were used to represent demographic data, with bars showing the prevalence of anxiety, depression, insomnia, and ASD. Univariate analysis of anxiety, depression, insomnia, and ASD using logistic regression model. After controlling for covariates, multivariate logistic regression analysis was used to explain the influencing factors of anxiety, depression, insomnia, and ASD. A two-tailed *p * 0.05 was considered statistically significant. All statistical analyses were performed using SPSS 25.0 software (IBM, Armonk, NY, USA).
Results
Demographic Characteristics
A total of 3105 subjects participated in this survey. In total, 189 were excluded due to missing data; of these, 116 subjects were excluded due to having a response time 2 minutes or 30 minutes. Therefore, 2800 eligible subjects were included in our final analysis, with a valid response rate of 90.2%. Fig. 1 shows a flowchart describing how the final respondents were recruited.
Flowchart showing how respondents were selected.
The socio-demographic characteristics are shown in Table 1. Of the 2800 participants, 1667 (59.5%) were female, 940 (33.6%) were over 40 years-of-age, and 1913 (68.3%) were married. Of the 2800 participants, 1480 (52.9%) had a bachelor’s degree, 823 (29.4%) had a master’s degree or above, and 497 (17.8%) had achieved less than a bachelor’s degree. Of the total number of respondents, 1401 (50%) were medical workers and 301 (10.8%) had a history of chronic diseases. In terms of annual income, 662 (23.6%) had an income CNY 50,000 (1 EUR = 7.6760 CNY), 900 (32.1 %) had an income between CNY 50,000 and 100,000, 809 (28.9%) had an income between CNY 110,000 and 200,000, and 429 (15.3%) had an income above CNY 200,000. According to our analyses, the two most common symptoms of COVID-19 infection were fever and cough; other symptoms included headache, general pain and weakness, and sore throat. In total, 2205 (78.8%) of the respondents had at least one family member infected with COVID-19. Overall, 2607 (93.1%) respondents indicated that there were confirmed or suspected cases in their work environment. The majority of participants (2089 [74.6%]) received three doses of vaccine. Additionally, 672 (24%) were not infected with COVID-19, 1230 (43.9%) were confirmed to be in the course of COVID-19, and 898 (32.1%) had recovered from COVID-19.
Table 1.: Demographic characteristics and epidemic-related information from all respondents.
Prevalence and Risk Factors for Mental Health Symptoms
Fig. 2 shows the prevalence of psychological problems in the Chinese population during the epidemic in China. Of the respondents, 52.0% had symptoms of anxiety, 58.3% had symptoms of depression, 45.2% suffered from insomnia, and the prevalence of ASDs was 34.8%.
Prevalence of mental health symptoms in the general population of China during the Omicron pandemic.
Supplementary Tables 1,2,3,4 present the results of our unadjusted analysis for demographic and epidemiological variables among the supplementary data. In multivariate analyses (Tables 2,3,4,5), females (odds ratio [OR]: 1.64; 95% confidence interval [CI]: 1.39–1.94; *p * 0.001), being a commerce occupations (OR: 1.79; 95% CI: 1.32–2.43; *p * 0.001), lower income level (OR: 1.80; 95% CI: 1.30–2.50; *p * 0.001), being in the course of infection (OR: 1.27; 95% CI: 1.03–1.57, p = 0.028), and low resilience (OR: 2.33; 95% CI: 1.94–2.81; *p * 0.001) were identified as risk factors for anxiety. Females (OR: 1.27; 95% CI: 1.07–1.50; p = 0.006), aged 40 years (OR: 1.49; 95% CI: 1.23–1.82; *p * 0.001), being unmarried (OR: 1.30; 95% CI: 1.04–1.64; p = 0.023), being a commerce occupations (OR: 1.72; 95% CI: 1.27–2.32; *p * 0.001), being in the course of infection (OR: 1.76: 95% CI: 1.44–2.16; *p * 0.001), and low resilience (OR: 3.28; 95% CI: 2.70–3.98, *p * 0.001) were identified as risk factors for depression. Being unmarried (OR: 1.28; 95% CI: 1.02–1.60; p = 0.031), having a bachelor’s degree (OR: 1.33; 95% CI: 1.10–1.62; p = 0.003), being a commerce occupations (OR: 1.52; 95% CI: 1.13–2.05; p = 0.006), being in the course of infection (OR: 1.95; 95% CI: 1.57–2.42; *p * 0.001), and low resilience (OR: 3.38; 95% CI: 2.79–4.09; *p * 0.001) were identified as risk factors for insomnia. The risk of ASD was significantly higher among commerce occupations (OR: 2.20; 95% CI: 1.60–3.02; *p * 0.001), lower income levels (OR: 1.94; 95% CI: 1.34–2.79; *p * 0.001), being in the course of infection (OR: 1.56; 95% CI: 1.25–1.93; p = 0.001), and low resilience (OR: 5.64; 95% CI: 4.58–6.96; *p * 0.001).
Table 2.: Multivariate logistic regression analysis of factors related to anxiety during the Omicron variant pandemic.
Table 3.: Multivariate logistic regression analysis of factors related to depression during the Omicron variant pandemic.
Table 4.: Multivariate logistic regression analysis of factors related to insomnia during the Omicron variant pandemic.
Table 5.: Multivariate logistic regression analysis of factors related to acute stress disorder during the Omicron variant pandemic.
Discussion
Although being diagnosed with COVID-19 may no longer be viewed as life-threatening, the general population faces multiple stressors during Omicron outbreak. Previous research showed that the COVID-19 pandemic has had a negative impact on mental health in many countries, thus attracting widespread research attention [18, 19]. In the present study, we identified major demographic risk factors associated with mental disorders during the Omicron pandemic. These included being female, younger than 40 years-of-age, unmarried, and having a low income. These findings were consistent with previous findings [20, 21]. As a vulnerable group, medical workers bore a high level of psychological stress due to their occupational exposure risk during the early stages of the COVID-19 epidemic [22, 23, 24]. Furthermore, the prevalence rate of mental disorders was higher than that of non-medical workers [25]. However, opposite trends were observed for occupation; in the present study, we found that public institutions, administrative personnel, and commercial personnel had a higher susceptibility to mental disorders than medical workers during the Omicron epidemic. Our findings were supported by a previous study which confirmed that medical workers presented with lower levels of anxiety, depression, and acute stress than non-medical workers, as determined by assessing mental health of medical workers after one year of the COVID-19 pandemic [26]. This may be attributable to the experience accumulated by the early epidemic prevention work for medical staff, the development of effective coping strategies, and the popularization of vaccination. However, the general public have less social psychological support, personal protection knowledge, and protective equipment [7].
In the context of the Omicron strain, we found that more than half of the respondents exhibited symptoms of anxiety (52.0%) and depression (58.3%), approximately half of the respondents experienced insomnia (45.2%), and one-third had ASD (34.8%); these data were higher than the prevalence reported during the initial outbreak of COVID-19 [27]. Network analysis conducted in February 2020 evaluated the mental health symptoms of the general population in China and found that the prevalence of anxiety, depression, insomnia, and acute stress symptoms was 27.9%, 31.6%, 29.2% and 24.4%, respectively [28]. According to a report by the Chinese Center for Disease Control and Prevention on 25 Jan 2023, the number of COVID-19 infections in China first increased and then decreased from 9 Dec 2022. Our research was undertaken at a stage when the number of COVID-19 infections in China was skyrocketing, and 76% of cases had been artificially confirmed or suspected cases, thus increasing the risk of infection for the whole population and increasing psychological pressure. As a result, more people are suffering from mental health concerns. A meta-analysis previously showed that the prevalence of post-recovery anxiety, depression, and post-traumatic stress disorder was 19%, 20%, and 28%, respectively, among survivors of a 2002–2003 outbreak of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [29, 30]. The long-term psychological disorders observed in the survivors of SARS highlight the potential long-term mental health complications in patients with COVID-19 [31]. The global public health crisis caused by COVID-19 has lasted longer than many of us expected. It is vital that public health authorities should be prepared to prevent the long-term psychological disorders associated with COVID-19 infection.
The respondents in this study who were in the course of COVID-19 infection were more vulnerable to the negative effects of the pandemic. Early in the outbreak, previous studies reported that COVID-19 patients had higher levels of psychological distress than uninfected patients [4, 32]. We consider that these results were mainly due to the fear of death caused by a new mutated strain, various physical discomforts post-infection, uncertainties such as the lack of effective treatment drugs and epidemic prevention materials, as well as a fear of spreading the virus to family members. Therefore, it is important that we pay more attention to this body of subjects in the course of infection, and to provide timely psychological guidance.
Resilience is considered to be an individual’s ability to cope effectively with adversity and defend against the psychological stress caused by traumatic events [33, 34]. The lower the psychological resilience, the higher the risk of anxiety, depression, insomnia, and ASD. A previous study showed that the prevalence of psychological distress was negatively correlated with mental resilience at the peak of the COVID-19 epidemic [35]. Psychological resilience is essential to the ability to cope effectively with difficulty, uncertainty, and change. Previous studies have shown that people who go out more often, exercise more, receive more social support from their family, friends and significant others, and sleep better have higher levels of resilience [36]. Therefore, enhancing the mental resilience of the public during epidemics should be a public health priority to help the population cope more effectively with stress and distress.
Limitations
There are several limitations to the present study that should be considered. First, the sample size of patients collected was limited, and the survey predominantly targeted Internet users; thus, the sample was not fully representative. Second, the survey did not account for respondents’ prior history of mental disorders. Third, the results reflect only short-term mental health outcomes during the Omicron pandemic. Further studies are now needed to determine the mental health outcomes associated with Omicron infection.
Conclusion
In the present study, we found that the prevalence of anxiety, depression, insomnia, and acute stress disorder associated with the Omicron strain in China was notable, especially among confirmed or suspected patients during the course of infection. Furthermore, psychological resilience was associated with the risk of psychological disorders. Even three years after the COVID-19 outbreak, its negative impact on people’s mental health remains crucial, suggesting that the long-term effects of stressful events cannot be ignored. Stressful events, such as epidemics, natural disasters, or social upheavals, often subject individuals to considerable psychological stress. Increasing psychological resilience in the public to enable them to cope effectively with these stressors is critical to mitigating the occurrence of mental health problems. Future studies should focus on longitudinal follow-ups to investigate the long-term mental health outcomes associated with COVID-19 and other stressful events. This will help better understand the ongoing effects of such events on individuals’ psychological states and develop strategies to address stress and emotional distress more effectively.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wang C Horby PW Hayden FG Gao GF A novel coronavirus outbreak of global health concern Lancet (London, England) 20203954704733198625710.1016/S 0140-6736(20)30185-9PMC 7135038 · doi ↗ · pubmed ↗
- 2Liu S Yang L Zhang C Xiang YT Liu Z Hu S et al Online mental health services in China during the COVID-19 outbreak The Lancet. Psychiatry 20207 e 17e 183208584110.1016/S 2215-0366(20)30077-8PMC 7129099 · doi ↗ · pubmed ↗
- 3Daly M Robinson E Depression and anxiety during COVID-19 Lancet (London, England) 202239951810.1016/S 0140-6736(22)00187-8PMC 881306035123689 · doi ↗ · pubmed ↗
- 4Lu X Xie Y Feng H Liu Z Ouyang K Hou B et al Psychological impact on COVID-19 patients during the outbreak in China: A case-control study Psychiatry Research 20213051141803446135710.1016/j.psychres.2021.114180 PMC 8381686 · doi ↗ · pubmed ↗
- 5Meo SA Meo AS Al-Jassir FF Klonoff DC Omicron SARS-Co V-2 new variant: global prevalence and biological and clinical characteristics European Review for Medical and Pharmacological Sciences 202125801280183498246510.26355/eurrev_202112_27652 · doi ↗ · pubmed ↗
- 6Nutalai R Zhou D Tuekprakhon A Ginn HM Supasa P Liu C et al Potent cross-reactive antibodies following Omicron breakthrough in vaccinees Cell 202218521162131.e 183566241210.1016/j.cell.2022.05.014PMC 9120130 · doi ↗ · pubmed ↗
- 7Tan BYQ Chew NWS Lee GKH Jing M Goh Y Yeo LLL et al Psychological Impact of the COVID-19 Pandemic on Health Care Workers in Singapore Annals of Internal Medicine 20201733173203225151310.7326/M 20-1083 PMC 7143149 · doi ↗ · pubmed ↗
- 8Agaibi CE Wilson JP Trauma, PTSD, and resilience: a review of the literature Trauma, Violence & Abuse 2005619521610.1177/152483800527743816237155 · doi ↗ · pubmed ↗