Scintigraphy for the diagnosis of primary unrecognised fractures in multiple trauma patients - a prospective, blinded, monocentric study
Arne Wilharm, Philipp Schenk, Kay Becker, Lina Van Nie, Joachim Hillmeier, Gunther Olaf Hofmann, Dominik Wilkens

TL;DR
This study shows that using whole-body skeletal scintigraphy can significantly reduce missed bone injuries in multiple trauma patients compared to standard methods.
Contribution
The study demonstrates the superior sensitivity of three-phase whole-body skeletal scintigraphy in detecting missed fractures in polytrauma patients.
Findings
Skeletal scintigraphy had a sensitivity of 98.8% compared to 75.4% for standard methods.
60 additional bony injuries were identified, with most requiring conservative treatment.
Scintigraphy is a low-risk, highly sensitive method for reducing missed injuries.
Abstract
After structured (S3 guideline, ATLS®) acute care of multiple trauma patients in trauma centers, post-acute missed injuries continue to occur with incidence rates ranging from 1.3 to 39% as described in literature. The aim of the tertiary survey was the reduction of these rates. However, high numbers of missed injuries continue to be reported. The aim of this prospective, single-center, blinded clinical diagnostic study was to determine whether the standardised use of 3-phase whole-body skeletal scintigraphy in severely injured patients can reduce the number of missed injuries compared with the established standard procedure for polytrauma diagnosis. 26 patients aged 18 years or older (median 53.5 years, 4 female, 22 male) with an ISS ≥ 9 were evaluated by an orthopaedic and trauma surgeon using skeletal scintigraphy after completion of standardised trauma room diagnostics and tertiary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
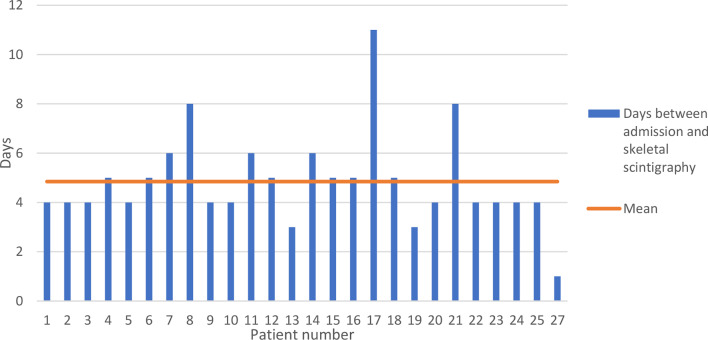 Figure 1
Figure 1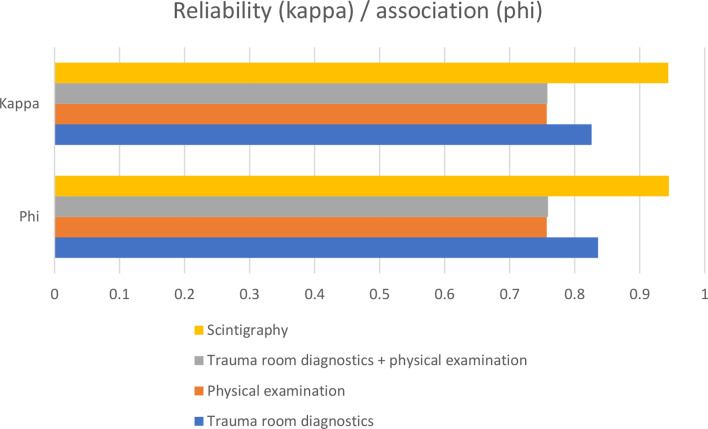 Figure 2
Figure 2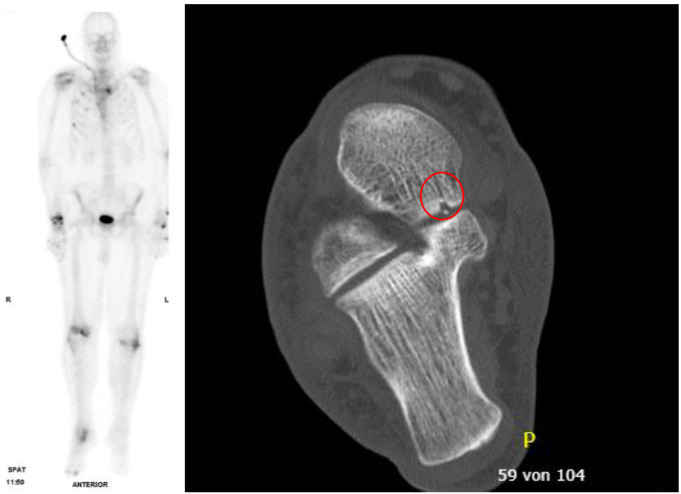 Figure 3
Figure 3- —Universitätsklinikum Jena (8979)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrauma and Emergency Care Studies · Trauma Management and Diagnosis · Abdominal Trauma and Injuries
Introduction
Delayed or overlooked injuries were referred to in the literature already in 1991 as the trauma surgeon’s “nemesis” [1]. Prior to the introduction of polytrauma spirals (whole body trauma scans), the rate of delayed diagnoses of injuries in seriously injured patients was between 1.3% and 39%, of which 15–22.3% were classified as clinically relevant. In their review, Pfeifer et al. summarise the results of 20 studies from 1980 to 2006 in which delayed diagnoses were identified by reviewing a patient’s records, re-examining the entire diagnostic process or re-examining the patient several months after the trauma [2]. In one registry study, among 26,264 patients who had been diagnosed by means of polytrauma spiral CT after trauma, 215 patients (0.82%) were identified in whom injuries were detected only after a delay [3]. Kok et al. reported in 2024 that despite polytrauma spiral CT, 13.9% of the 697 patients in the study had delayed diagnosis. This was particularly true for patients who were primarily admitted to intensive care or had an ISS ≥ 16. Half of the delayed injuries (49.5%) were imaged on CT [4].
To this day, despite polytrauma spiral CT and re-evaluation of patients and diagnostics as part of a tertiary survey according to ATLS, there are still overlooked injuries. However, the rate of undetected bony injuries in seriously injured patients is unclear, as the data in the literature are based only on follow-up examinations or registry evaluations and there are no studies in which the polytrauma spiral CT was compared to another highly sensitive method.
In 1992, Spitz et al. reported in a retrospective evaluation of 162 skeletal scintigraphies of severely injured patients that additional fractures were found in approximately ¼ of all cases. They were of the opinion that whole-body skeletal scintigraphy should be part of routine care for multi-trauma patients, similar to staging diagnostics for malignancies [5]. At the time, other authors also reported a high rate of additional fractures detected by skeletal scintigraphy in severely injured patients; for example, Runkel et al. 1993 found 68 additional fractures in 53 patients examined [6]. Despite high sensitivity and low radiation exposure for patients, skeletal scintigraphy has not become established as a routine examination for severely injured patients and has been forgotten for this indication.
Study objectives
The aim of this monocenter, prospective and blinded study was to determine whether additional fractures in multiply and seriously injured patients (ISS ≥ 9) can be detected by means of skeletal scintigraphy and whether these have clinical relevance, despite a polytrauma spiral CT and ATLS-compliant triple clinical examination.
Patients and methods
Study design
All adult (≥ 18 years), multiply or seriously injured patients (ISS ≥ 9) who were admitted to the emergency room of St. Vincenz Hospital Limburg, a regional TraumaZentrum DGU^®^, between 3 September 2019 and 18 June 2021 were included in the study with their consent (Table 1). The emergency room treatment was carried out in accordance with ATLS, including primary and secondary surveys, a polytrauma spiral CT and, if necessary, additional conventional X-rays. After four days, a standardised clinical examination by a specialist in the context of a tertiary survey was carried out to identify additional injuries. In the course of this follow-up, additional regions suspected of fracture were documented. On the sixth day after the trauma, a 3-phase whole body scintigraphy with Technetium Tc99m was performed. Based on the findings from the trauma room, the results of the follow-up clinical examination and the scintigraphy, further specific radiological diagnostics were then carried out.
Table 1; study inclusion and exclusion criteriaInclusion CriteriaExclusion CriteriaAge ≥ 18 yearsAge < 18 yearsGender Male, Female, DiverseISS ≥ 9 points and < 75 pointsISS < 9 points or = 75 pointsInpatient admissionNo inpatient admissionConsent to the studyNo consent for studywhole body CT, scintigraphy and tertiary survey performedPatient transferred or discharged before scintigraphy or tertial survey
Polytrauma spiral CT
All CT examinations were carried out using a Siemens computer tomograph (Somatom Definition Flash VA 48 A with Somaris 7 Syngo CT VA 48 A operating software). Non-contrast examination of the neurocranium (slice thickness of the reconstructions: 4 mm) was carried out first, followed by the non-contrast investigation of the cervical spine (slice thickness of the reconstructions: 2 mm). After intravenous administration of contrast agent (110 ml Imeron 350) with a delay of 80 s, the “whole body CT” was carried out from the skull base to the lesser trochanter minor, or in the case of injuries to the lower extremities, possibly including the feet (slice thickness of reconstructions: 2 mm). Arms were positioned on the body.
As part of this study, Analysis of the polytrauma spiral CT was carried out by a radiology specialist who was unaware of the clinical findings and the scintigraphy findings, as well as the radiological findings of the examination in the context of the actual clinical treatment.
Skeletal scintigraphy
All skeletal scintigraphies were carried out using a double-head camera from General Electric (Discovery NM 630). In each case, a 3-phase scintigraphy with imaging of the entire body and an additional SPECT examination was carried out.
The skeletal scintigraphy was evaluated by a specialist in nuclear medicine as part of the study, without knowledge of the clinical findings and the findings of the polytrauma spiral CT, as well as the radiological findings of the examination in the context of the actual clinical treatment.
Verification of additional scintigraphic findings
All fractures identified by scintigraphy were verified by new CT, with slice optimisation, additional CT scan or, in cases of doubt, MRI in order to rule out other causes for the enhancement.
Data collection
The fractures identified in the three examinations (polytrauma spiral CT, tertiary survey with clinical examination, skeletal scintigraphy) were recorded in an Excel database created for this purpose (Microsoft, Redmondon, USA). A total of 170 possible fracture localisations were distinguished.
Statistical analysis
Statistical analysis was performed using SPSS V.26 (IBM SPSS Statistics for Windows. Armonk, NY: IBM Corp.). In addition to descriptive statistics, the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated. Furthermore, Phi and Kappa were calculated as measures of the correlation or agreement of the examination results (Table 1).
Table 2. Interpretation of phi coefficient and Cohens kappaPhi CoefficientCohens Kappa+ 0.70 or higherVery strong positive relationship0agreement equivalent to chance+ 0.40 to + 0.69Strong positive relationship0.10–0.20slight agreement+ 0.30 to + 0.39Moderate positive relationship0.21–0.40fair agreement+ 0.20 to + 0.29weak positive relationship0.41–0.60moderate agreement+ 0.01 to + 0.19No or negligible relationship0.61–0.80substantial agreement0No relationship0.81–0.99near perfect agreement-0.01 to -0.19No or negligible relationship1perfect agreement-0.20 to -0.29weak negative relationship-0.30 to -0.39Moderate negative relationship-0.40 to -0.69Strong negative relationship-0.70 or higherVery strong negative relationship
Analysis was carried out for the entire skeleton and subsequently separated according to body regions, i.e. head, upper extremity, lower extremity, body trunk (thorax, spine, pelvis) and small bones (hand and foot skeleton). In this context, “consensus” refers to all fractures that were considered proven in the overall view of the clinical and radiological examinations and, if necessary, additional MRI or other further radiological diagnostics.
Ethics vote
The study was approved by the Ethics Committee of the University Hospital Jena (registration number 2018-1138-BO) and the performance of the additional scintigraphy was approved by the Federal Office for Radiation Protection Germany with the patient’s consent (approval number Z 5–22464/2019-110-G, valid from 03/09/2019 to 18/06/2021).
Results
In order to include a statistically significant number of patients in the study, all patients with an ISS ≥ 9 who were admitted to hospital during the study period approved by the Federal Office for Radiation Protection had to be included.
A total of 26 patients (4 female, 22 male) with a mean age of 52.9 years (range, 20 to 83 years) were included in the study. Fourteen patients had an ISS of 9 to 15 points, and 12 had an ISS of ≥ 16 points (ISS 9 to 29, mean 16.2 points). All patients were alert, oriented, and cooperative upon arrival at the emergency department. The additional physical examination as part of the tertiary survey took place on average after 4.9 days (1 to 11 days) and the skeletal scintigraphy after an average of 7.7 days (5 to 21 days) (Fig. 1).
Fig. 1. Time between admission and skeletal scintigraphy [d]
In total, 256 fractures were detected in 26 patients by means of diagnostics (consensus). Fractures at 4164 localisations were excluded (consensus).
By means of the diagnostics in the trauma room (Table 2), i.e. clinical examination, polytrauma spiral CT and, if necessary, additional X-ray diagnostics in the trauma room, 187 fractures could be correctly identified. 69 fractures were not detected (Table 3). This corresponds to a sensitivity of 73.0%. In 5 further recognised fractures, it was found in the course of treatment that there was no fracture (3x cervical spine, 1x thoracic spine, 1x lumbar spine).
The tertiary survey (Table 4), i.e., the repeat clinical examination after an interval, correctly identified 6 additional fractures (sensitivity 75.4%) and suspected fractures in 51 regions that were not confirmed in the further course. After completion of the standard procedure (trauma room diagnostics and tertiary survey), 63 fractures were not known in seriously injured patients and, in the overall view of the available findings in these areas, there was no indication for further diagnostics.
In the skeletal scintigraphy (Table 5), which was carried out as a supplementary examination in the context of this study, 252 fractures were detected (sensitivity 98.8%). Three fractures were not detected, including 2 metacarpal fractures that were not detected in the scintigraphy due to carpal fractures and insufficient Spatial resolution. They were later detected in the supplementary diagnostics due to the suspected carpal fractures. There was also one scapular fracture: an explanation for this is probably the proximal localisation to the body trunk and the early skeletal scintigraphy in this case after only 5 days post trauma. According to experience, these regions accumulate later than, for example, distal extremities near joints in the case of injuries during scintigraphy [7]. in 25 regions, a fracture was suspected, which was not confirmed by the overall findings (Table 6). in these cases, the re-evaluation of the previous diagnostic procedures and the additional MRI tests revealed only degenerative changes.
Scintigraphy has by Far the highest sensitivity at 98.8%. Only 3 of 256 fractures were not detected. Trauma room diagnostics have a sensitivity of only 73%. Sixty-nine fractures were not detected in the trauma room. In particular, rib fractures and fractures of the hand and foot skeleton were not detected. At the same time, the emergency room diagnostic investigation has the highest specificity at 99.9%. Only five vertebral fractures were not confirmed. The specificity of the scintigraphy is somewhat lower at 99.4%. Twenty-five suspected fractures were later found to be degenerative changes. The tertiary survey with a further clinical examination only slightly increased the sensitivity. Only 6 further fractures were diagnosed. However, 51 fractures that had been suspected in the clinical examination were not confirmed. The sensitivity is therefore only 75.4% (Table 7).
Table 3. Statistical calculations, trauma room diagnostics (clinical examination, polytrauma spiral CT and, if necessary, additional radiological diagnostics in the trauma room)ConsensusPositivNegativ Trauma room diagnostics positiv1875negativ694159sensitivityfalse positive73,0%0,1%false negativespecificity27,0%99,9%PPV97,4%NPV98,4%prevalence5,8%p-valuePhi0,8360,000Kappa0,8260,000
Table 4. Fractures not detected in the emergency room diagnostics. Detection using scintigraphy. Detection using X-raysPat. IDFractures that were not recognizedin the trauma room diagnosticsQtyConsequence1thoracic vertebra 7 fracturethoracic vertebra 8 fracture2conservativeconservative2os metatarsale 4 fracturemanubrium sterni fracture2immobilisationconservative3serial rib fractures 4-11os trapezium fracture9additional respiratory therapyimmobilisation4os hamatum avulsionos trapezium avulsionmetacarpale fracture 2 + 42hand was already immobilised due to thumb fracture5rib fracture 1 rightrib fracture 1 + 2 leftcorpus sterni fracture4conservativeconservativeconservative6minimal dislocated lateral longitudinal patellar fracture1conservative7serial rib fractures 7 -11spinosus process fracture L46conservativeconservative8serial rib fractures left 5-8serial rib fractures right 9–117additional respiratory therapyadditional respiratory therapy9fracture of the 5. toeinfraction medial tibial plateaufracture of the patellafracture T84immobilisationconservativeconservativeconservative10fracture L11conservative11infraction of the medial femoral condylenon-displaced fracture of the medial tibial plateauosteochondral avulsion on the posterior surface of the patella3conservativeconservativeconservative12small avulsion at the greater trochanternon-displaced scapula fracturerib fractures 9 + 104conservativeconservativeconservative13infraction of the medial femoral condyle1conservative17rib fracture 6 rightserial rib fractures 3–7 left6conservativeconservative21infraction of the medial femoral condyleinfraction of the lateral tibial plateaunon-displaced fracture of the talusinfraction of the distal fibulainfraction at the medial malleolusserial rib fractures 3–6 rightinfraction proximal fibulainfraction proximal Tibiabone bruise of the lateral femoral condylemanubrium sterni fracturescapula fracture13conservativeconservativeimmobilisationconservativeconservativeconservativeconservativeconservativeconservativeconservativeconservative22fracture L5corpus sterni fracture2conservativeconservative
Table 5. Statistical calculations, trauma room diagnostics and tertiary survey (clinical examination, polytrauma spiral CT and, if necessary, additional radiological diagnostics in the trauma room and additional clinical examination after an interval)ConsensusPositivNegativ Trauma room diagnostics
** + **
tertiary survey positiv19351negativ634113sensitivityfalse positive75,4%1,2%false negativespecificity24,6%98,8%PPV79,1%NPV98,5%prevalence5,8%p-valuePhi0,7590,000Kappa0,7580,000
Table 6. Statistical calculations from skeletal scintigraphyConsensusPositivNegativ Skeletal scintigraphy positiv25325Negativ34139sensitivityfalse postive98,8%0,6%false negativespecificity1,2%99,4%PPV91,0%NPV99,9%prevalence5,8%p-valuePhi0,9450,000Kappa0,9440,000
Table 7. Localisation of fractures over-diagnosed in scintigraphy (joint-related degenerative changes)RegionQtyclose to the acromioclavicular joint3close to the hip joint1close to the carpus and metacarpus10close to the knee joint7close to the ankle joint3ulnar shaft1
Table 8. Sensitivity and specificity of the examinations for the different regions (upper and lower extremities, each without hands or feet)DiagnosticSensitivity/SpecificityTotal[%]Head[%]Upper extremity[%]Lower extremity[%]Trunk[%]Bones of the hands or feet[%] Trauma room diagnostics Sensitivity73.0100.0100.046.275.663.6Specificity99.9100.0100.0100.099.6100.0 Trauma room diagnostics + tertiary survey Sensitivity75.4100.0100.061.576.268.2Specificity98.895.699.699.198.698.7 Scintigraphy Sensitivity98.8100.0100.0100.099.590.9Specificity99.4100.099.898.299.899.4
A subgroup analysis was performed (severely injured patients with ISS 9 to 15 vs. polytraumatized patients with ISS ≥ 16). This showed a significantly higher sensitivity in the group with ISS 9 to 15 compared to the group with ISS ≥ 16 for shock room diagnostics (66.9% vs. 80.7%) and the combination of shock room diagnostics and tertiary survey (68.3% vs. 84.2%). In case of skeletal scintigraphy, there was only a marginal difference (98.6% vs. 99.1%), with a significantly increased sensitivity of nuclear medicine diagnostics compared to standard diagnostics.
The calculation of kappa and phi, as values for reliability and correlation, also shows the best results for scintigraphy (Fig. 2).
Fig. 2. Kappa and phi for the various examinations for the whole body
The additional scintigraphy and the resulting re-evaluation of the CT diagnostics, or extended diagnostics using CT or X-ray of certain regions and MRI diagnostics, led to the detection of a total of 60 additional fractures in 15 of 26 patients (57.7%) compared to standard diagnostics consisting of trauma room diagnostics and tertiary survey. Conservative therapy was used for 54 fractures, without additional immobilisation. In 5 fractures, affecting 4 patients, additional splints were used, for example in the case of a talus fracture that was identified only in the re-evaluation of the CT diagnostics, after which the scintigraphy showed an increased accumulation (Fig. 3). Furthermore, in one case, immobilisation could be terminated after ruling out a cervical spine injury (Table 8).
Table 9. Therapeutic consequences after scintigraphy and completion of additional diagnosticsHeadUpper extremityTrunkLower extremityBones of the hands or feetConservative without additional immobilisation004680Conservative with additional immobilisation00014Surgical00000Termination of unnecessary immobilisation00100
Fig. 3. Late phase of the scintigraphy. Various rib fractures on the right and, among other features, an accumulation in the right talus can be seen well. A talus fracture (circle) that was barely visible on the CT was confirmed here
Discussion
Overlooked injuries can overshadow successful life-saving measures in the further course of treatment and may have legal consequences. In this study, additional skeletal injuries were detected in 15 of 26 patients (57.7%) by means of supplementary skeletal scintigraphy. These injuries were not detected by primary diagnostics in the trauma room and a routine third clinical examination a few days after the accident. This is a significantly higher percentage than reported in the literature, where missed injuries are reported in 0.82 to 39% of patients [2, 3, 8–10], and was possible only with the use of highly sensitive skeletal scintigraphy. It was only through this that there were indications in 63 of 256 fractures (24.6%) that fractures had been overlooked in the previous diagnostics or that further diagnostics were required. Reliable avoidance of overlooked injuries by introducing a structured “tertiary survey” with the support of an app, as reported by Moffat et al. 2019 [11], is likely to be an illusion.
Although only alert and cooperative patients were included in this study, the primary trauma room diagnostics with ATLS-compliant primary and secondary survey, including polytrauma CT, showed a sensitivity of only 73% for a patient’s bony injuries, which could be increased by only 2.4–75.4% with a tertiary survey. In particular, fractures of the ribs, avulsions of the lower extremities and of the small bones in the hands and feet were identified only in the scintigraphy. In the case of the ribs, this could be due to the axial slices of the polytrauma CT not being orthogonal to the ribs. In the future, computer algorithms such as synbo.CT Bone Reading from Siemens [12] or artificial intelligence could help in such cases [13]. In the area of the extremities, the classic CT polytrauma spiral has two problems. In this study, the upper extremities were placed on the abdomen; hence, all slices had to be calculated in order to achieve an optimal slice direction to the carpal region and, moreover, artefacts caused by the trunk could not be avoided. In the area of the lower extremity, only an initial imaging is carried out in the trauma room if there are indications of injuries below the pelvis in the primary or secondary survey, so that these regions were in some cases not imaged.
In the authors’ opinion, a supplementary skeletal scintigraphy is a safe way to detect “all” bony injuries in severely injured patients and the minimal additional radiation exposure is acceptable (Tables 9, 10). The majority of the additionally detected fractures had no therapeutic relevance in terms of additional immobilisation or surgery. However, even in this study with a relatively small number of patients, 5 fractures (7.2%) required additional immobilisation, which would not have occurred without the information provided by scintigraphy. The additional information obtained from skeletal scintigraphy could also be relevant in the long-term follow-up of patients with persistent complaints, in the context of assessments for compensation claims, accident insurance or pension applications.
Limitations of the study
Only a relatively small number of patients could be enrolled because the use of radiation on patients in Germany is subject to an extensive approval procedure and only very few and very old preliminary studies were available to indicate a benefit for patients. The inclusion of patients had to be stopped when the approval of the Federal Office for Radiation Protection and the insurance company expired.
Unfortunately, only conscious patients could be included in the study, as there is no neurosurgery on site at St. Vincenz Hospital and patients with craniocerebral trauma had to be transferred elsewhere. Accordingly, all patients were able to provide detailed information in the trauma room and during the tertiary survey about where they had pain or restricted mobility. In intubated and mechanically ventilated patients, even more fractures would probably have been detected only during skeletal scintigraphy. This requires further study at a level I trauma center.
Table 10. Radiation exposure from various diagnostic procedures [14–17]Radiological/nuclear medicine procedureRadiation exposure3-phase whole body skeletal scintigraphy with Tc99m/HDP500 MBqcorresponds to 2.85 mSvConventional x-raythoracic X-rayposterior-anterior0.02 mSvlumbar spine2.4 mSvComputed tomographyskull2 mSvthorax and abdomen8 mSvpolytrauma spiral examination31 mSv
The reference list from the paper itself. Each links out to its DOI / PubMed record.