Promising Treatment Strategy for Primary Malignant Melanoma of the Esophagus by Radical Esophagectomy and Nivolumab as Adjuvant Therapy: A Case Report
Yusuke Yamamoto, Junya Kitadani, Keiji Hayata, Taro Goda, Shinta Tominaga, Tomoki Nakai, Shotaro Nagano, Ryuta Iwamoto, Manabu Kawai

TL;DR
A patient with rare esophageal melanoma had successful treatment with surgery and nivolumab, remaining recurrence-free for over a year.
Contribution
This case report presents a novel treatment approach combining radical surgery and adjuvant nivolumab for primary malignant melanoma of the esophagus.
Findings
The patient remained recurrence-free for over 1 year after treatment.
Adjuvant nivolumab was well-tolerated with no serious side effects.
The treatment approach may be promising for PMME, similar to cutaneous melanoma.
Abstract
Primary malignant melanoma of the esophagus (PMME) is a rare malignant tumor of the esophagus with very poor prognosis due to high rates of recurrence and metastasis even after radical resection. Recently, however, immune checkpoint inhibitors such as anti-programmed cell death-1 antibodies have been suggested to improve the prognosis of malignant melanoma. This report describes the use of postoperative nivolumab as adjuvant therapy after surgical resection of PMME, with recurrence-free follow-up for more than 1 year. A 69-year-old man had chest discomfort and tightness in his throat. Upper gastrointestinal endoscopy revealed multiple melanosis and an elevated lesion in the middle esophagus. After histological examination, he was diagnosed as having PMME, so he underwent thoracoscopic subtotal esophagectomy, three-field lymphadenectomy, pedunculated jejunum reconstruction with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
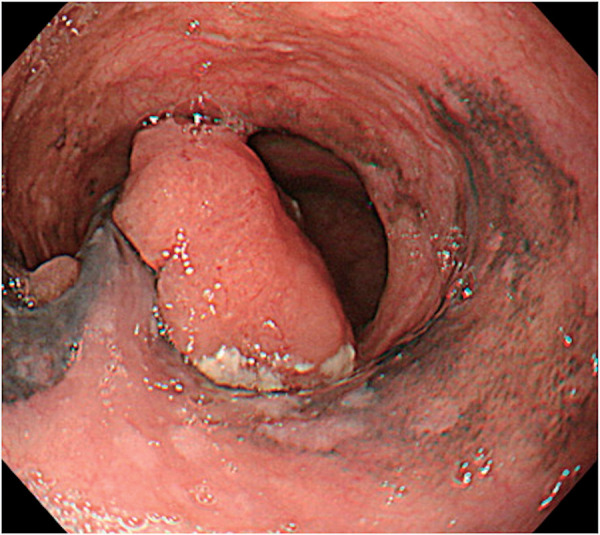 Fig. 1
Fig. 1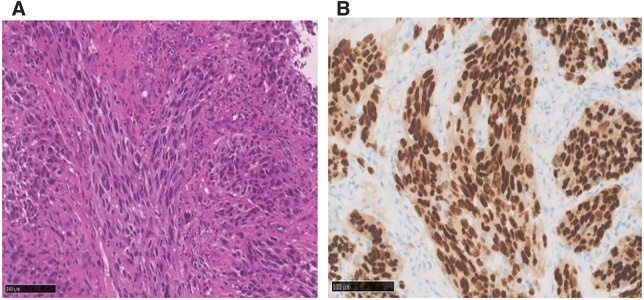 Fig. 2
Fig. 2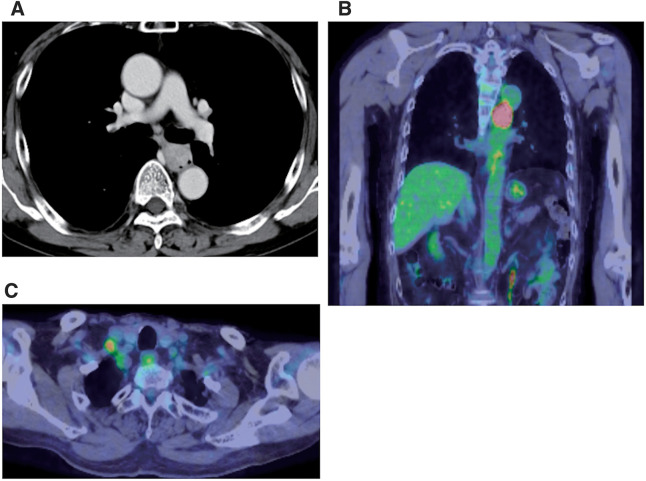 Fig. 3
Fig. 3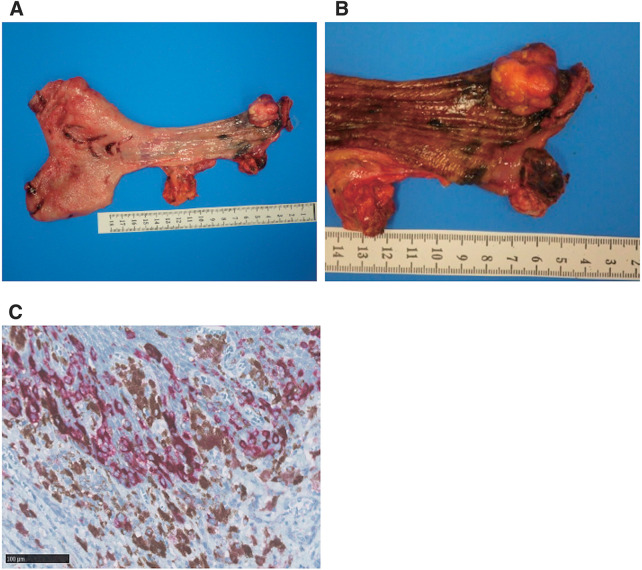 Fig. 4
Fig. 4| No. | Author | Year | Age | Sex | Stage (AJCC/UICC 8th edition) | Metastasis or recurrence | Therapy | Therapeutic duration | Adverse events | Follow-up period | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Inadomi et al. | 2016 | 73 | M | IV | Liver, lung, lymph node | Chemoradiotherapy → nivolumab | 1 month (Chemoradiotherapy) → 4 months | Bi-cytopenia | 7 months | Dead |
| 2 | Endo et al. | 2020 | 70 | M | Ⅲ | Retroperitoneal | Nivolumab | 41 courses | Adrenal insufficiency | 20 months | Alive |
| 3 | Ito et al. | 2021 | 81 | F | Ⅲ | Multiple lymph nodes, bone | Nivolumab | 30 courses | None | 27 months | Dead |
| 4 | Yamaguchi et al. | 2021 | 75 | F | Ⅱ or Ⅲ | Pleural dissemination, pancreas | Nivolumab → RT | 3 courses → RT | Renal dysfunction | 26 months | Alive |
| 5 | Tsukamoto et al. | 2021 | 74 | M | Ⅰ | Liver | Nivolumab → nivolumab + ipilimumab | 7 courses → nivolumab + ipilimumab 2 courses | None | Unknown | Unknown |
| 6 | Okamoto et al. | 2021 | 79 | M | IV | Lymph nodes, lung, pleural, peritoneal metastases | Nivolumab | 6 courses | Kidney injury | 5 years | Alive |
| 7 | Kashfi et al. | 2022 | 76 | F | IV | Bone | Nivolumab | 2 courses | None | 2 months | Dead |
| 8 | Hanada et al. | 2022 | 65 | F | Ⅰ | Jejunum, cervical esophagus, lymph nodes, lung | Nivolumab | 32 courses | None | 9 months | Alive |
| 9 | Furune et al. | 2022 | 62 | M | II or III | None | Nivolumab | 7 months | Interstitial pneumonitis | Unknown | Unknown |
| 10 | Nambara et al. | 2022 | 60 | F | Ⅳ | None | Nivolumab | 1 year (adjuvant) | Pneumothorax | 12 months | Alive |
| 11 | Attlassy et al. | 2023 | 66 | F | IV | Liver | Pembrolizumb → nivolumab + ipilimumab | Pembrolizumb 8 courses → nivolumab + ipilimumab 4 months | Kidney disease | 3 years | Alive |
| 12 | Shibayama et al. | 2025 | 75 | M | III | None | Ipilimumab and nivolumab → operation → nivolumab | Ipilimumab and nivolumab 4 courses (neoadjuvant) → one year (adjuvant) | Hyponatremias | 3 years | Alive |
| 13 | Our case | 2025 | 69 | M | Ⅱ | None | Nivolumab | 24 courses (adjuvant) | None | 12 months | Alive |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Immunotherapy and Biomarkers · Cutaneous Melanoma Detection and Management · Immunotherapy and Immune Responses
Abbreviations
PD-1 programmed cell death-1 PET positron emission tomography PMME primary malignant melanoma of the esophagus SOX SRY-related HMG-box
INTRODUCTION
PMME is a malignant tumor originating from melanocytes in the basal portion of the esophageal squamous epithelium and the stromal border. PMME is rare, accounting for <0.1%–0.2% of all esophageal malignancies, and <0.05% of all melanoma subtypes.^1)^ Poor prognosis of PMME is associated with delayed detection and a high likelihood of metastasis and recurrence. Esophagectomy is a radical treatment for PMME, but the recurrence rate remains high. Furthermore, the prognosis has been extremely poor, with an average life expectancy of 13.5 months at the time of diagnosis.^2)^ However, with the improvement of diagnostic techniques for early detection and the use of immune checkpoint inhibitors such as anti-PD-1 antibodies, the prognosis is considered to be improved.^3–6)^ Cases of long-term survivors who underwent immune checkpoint inhibitors for PMME have been reported.^7–15)^ However, the number of such cases remains limited, and further research is needed to provide conclusive evidence. In this report, we describe a case of PMME treated with radical esophagectomy followed by adjuvant therapy with nivolumab that has been relapse-free for more than 1 year. Furthermore, literature reviews regarding nivolumab for the treatment of PMME were performed.
CASE PRESENTATION
A 69-year-old man with a history of pyloric gastrectomy for duodenal ulcer, multiple colonic polyps and hemorrhoids saw his usual doctor with chest discomfort and tightness in his throat. Upper gastrointestinal endoscopy revealed melanosis and an elevated lesion in the middle esophagus, so he was referred to our department. There was no pigmentation of the skin or oral mucosa.
Re-examination of upper gastrointestinal endoscopy showed a 40 mm large, dark brown tumor with a surrounding 100 mm black pigmentation in the middle thoracic esophagus (Fig. 1). Tumor biopsy revealed proliferation of polygonal and spindle-shaped cells with reduced adherence, prominent nucleoli and stromal fibrosis (Fig. 2A). Immunostaining was negative for CK (AE1/AE3), p63, and S100, but diffusely strongly positive for SOX 10, which confirmed diagnosis of PMME (Fig. 2B). PD-L1 protein (clone 28-8) was expressed in <1%. Contrast-enhanced CT scan showed a mass lesion with contrast effect in the middle thoracic esophagus (Fig. 3A) and an 8 mm-sized lymph node swelling (Station No. 104R). There was no obvious distant metastasis. Fluorodeoxyglucose PET-CT indicated abnormal accumulation in each region (Fig. 3B and 3C).
Esophagogastroscopy showed a 40 mm large dark brown tumor with a surrounding 100 mm black pigmentation, located in the middle thoracic esophagus.
Microscopic findings of the biopsy specimen. (A) Histopathological examination with magnification ×20. (B) SOX-10 staining with magnification ×20.
Preoperative findings. (A) Contrast-enhanced computed tomography of chest showing a mass lesion with contrast effect in the middle thoracic esophagus. (B) Fluorodeoxyglucose positron emission tomography-computed tomography showing an abnormal accumulation in the same region. (C) Accumulated lymph node (Station No. 104R).
The patient was diagnosed as cStage IVa PMME (cT2, cN0, cM1a [AJCC 8th^16)^]) and underwent thoracoscopic subtotal esophagectomy, 3-field lymphadenectomy, pedunculated jejunum reconstruction with super-charge and super-drainage, and feeding jejunostomy. The operation time was 661 minutes and the blood loss was 420 mL. Minor leakage occurred at the esophagojejunostomy (Clavien-Dindo classification Grade II). The patient was discharged 50 days after the surgery. A nodular mass (25 × 22 mm) protruding into the lumen had formed 10 mm from the proximal cut end and blackish changes were observed in the surrounding mucosa (Fig. 4A and 4B). Pathologically, atypical spindle-shaped cells proliferated mainly in bundles, and atypical epithelial-like cells producing brown pigment proliferated solidly on the basal epithelial layer of the surrounding mucosa, indicating PMME (pT3, LVI [−], PMx, pDM0, pRM0, pN0). Preoperative PET-CT showed uptake of the Standard Uptake Value max 4. Lymph node dissection on both sides of No. 104 was completely performed, but no metastases were observed in the pathological findings. Therefore, swollen lymph nodes were considered to be inflammatory changes. SOX-10 and Melan A positive melanocytes (Fig. 4C) were distributed up to 1.5 mm from the cut edge, and melanin deposition and melanocyte proliferation were observed at the cut edge beyond the melanocyte distribution. Although melanocytes were found at the resection margin, the degree of cellular atypia was mild. Finally, they were diagnosed as ectopic melanocytes and designated as PMx. With the patient’s informed consent, nivolumab therapy (240 mg, every 2 weeks) was administered for 1 year. The patient showed no serious adverse events related to immunotherapy and is alive without relapse at the point of completion of adjuvant therapy. Follow-up findings of contrast-enhanced CT and esophagogastroscopy after completion of adjuvant therapy showed no recurrence of melanoma (Supplementary Fig. 1).
Surgical specimen of esophagus. (A) Protruding into the lumen was formed at 10 mm from the proximal end. (B) Blackish changes in the surrounding mucosa. (C) Microscopic findings of the surgical specimen of Melan-A staining with magnification ×20.
DISCUSSION
PMME is a rare tumor of the esophagus, with only about 480 cases reported by 2021 since Baur reported the first case in 1906.^17)^ Due to its rare occurrence, the clinical and molecular etiology and the optimal treatment of PMME are not properly understood. The prognosis of these tumors has been considered poor, with a reported 5-year survival rate of 4% in resected cases.^18,19)^ However, recent advances in endoscopic techniques have enabled early diagnosis, and a recent paper reported the 5-year survival rate after resection as 37%.^20)^
The average age of onset of PMME is 60 years, younger than that of esophageal cancer, and dysphagia and epigastralgia are common chief complaints.^21)^ The middle and lower esophagus account for 92.1% of all cases and more than half have invasion deeper than the muscular layer when detected, which is also thought to be a factor in the poor prognosis.^22)^ Surgical resection is the most common treatment and according to one report, 59 of 76 patients with PMME (77.6%) underwent esophagogastrostomy with subtotal esophagectomy and lymph node dissection, with subsequent recurrence identified in 89.7% of patients postoperatively.^22)^ In another report, more than 90% of postoperative recurrences in patients with PMME occurred within 2 years after the primary surgery.^2)^ The most frequent sites of recurrence were reported to be lymph nodes, the liver, the lungs, in bone, and in sites of anastomosis.^2)^
The high recurrence rate dictates the need for postoperative adjuvant therapy, but there is no consensus on the use of postoperative chemotherapy for rare cancers.^22–24)^ The combination of temozolomide and cisplatin as adjuvant chemotherapy for malignant melanoma significantly improved both relapse-free survival and overall survival.^22)^ However, the CheckMate 066 study for patients with unresectable, untreated stage III and stage IV malignant melanoma compared nivolumab with the conventional chemotherapy of dacarbazine.^25)^ Nivolumab had significantly improved response rate, progression-free survival, and overall survival. Nivolumab has thus become a standard treatment for advanced malignant melanoma. The CheckMate 238 trial also showed that nivolumab significantly prolonged relapse-free survival compared with the cytotoxic T-lymphocyte antigen-4 inhibitor ipilimumab in Stage IIIB or IIIC and IV malignant melanoma after resection.^26)^ Additionally, the CheckMate 76 K revealed a statistically significant improvement in 1-year recurrence-free survival with nivolumab versus placebo in Stage IIB/C melanoma (89% vs. 79%; HR 0.42, 95% CI: 0.30–0.59; P < 0.0001), underscoring its role in reducing recurrence risk by nivolumab for 12 months.^27)^ As with this report, a 1-year course of adjuvant nivolumab is considered appropriate for PMME.
Malignant melanoma is characterized by a high tumor mutational burden and a diversity of tumor-associated antigens, contributing to recognition by the immune system and making it highly responsive to immune checkpoint inhibitors.^28)^ As with cutaneous melanoma, PMME is expected to be a target for immune checkpoint inhibitors. Furthermore, the CheckMate 577 trial demonstrated the efficacy of nivolumab as adjuvant therapy for esophageal or gastroesophageal junction cancer, showing a significant improvement in disease-free survival compared with a placebo.^29)^ This landmark result supports the potential use of nivolumab in other malignancies, including rare cancers such as PMME. Due to the aggressive nature of PMME and the limited options available for adjuvant therapy, the concept of using nivolumab as adjuvant treatment in this setting appears to be promising, although there are currently no large-scale trials specifically designed for PMME. However, extrapolation of the CheckMate 577 results to PMME could guide future investigations and therapeutic strategies.
Only 13 patients with PMME who underwent administration of nivolumab have been reported, including our case (Table 1).^7–15,30–32)^ In these reports, nivolumab was primarily used for PMME with recurrence or metastasis, although one case involved its use as neoadjuvant therapy. Additionally, only three cases, including ours, reported the use of nivolumab as adjuvant chemotherapy for PMME, with no recurrences reported to date.^9,15)^ Similar to cutaneous melanoma, our results suggest that radical esophagectomy followed by 1 year of adjuvant therapy with nivolumab may be a promising treatment strategy for PMME in the future. While nivolumab has been suggested to improve progression-free survival in cases of metastatic or recurrent PMME, its efficacy as an adjuvant therapy for PMME has not yet been proven. Validation studies of adjuvant therapy with nivolumab for PMME are needed to collect more cases and long-term follow-up data, although the number of patients is limited due to rare cancer types.
CONCLUSIONS
Postoperative adjuvant therapy with nivolumab for PMME seems to be a safe, feasible, and potentially effective treatment to improve long-term outcomes. However, further case series and validation are needed.
SUPPLEMENTARY MATERIALS
Supplementary Fig. 1. Follow-up findings. (A) Contrast-enhanced CT showed no evidence of recurrence. (B) Esophagogastroscopy showed no pigmentation at the anastomosis site, suggestive of recurrence of melanoma.
ACKNOWLEDGMENTS
The authors acknowledge proofreading and editing by Benjamin Phillis from the Clinical Study Support Center at Wakayama Medical University.
DECLARATIONS
Funding
Not applicable.
Authors’ contributions
YY and JK drafted the manuscript.
KH, TG, ST, TN, SN, and MK critically revised the manuscript.
RI gave pathological diagnosis and collected the pathological pictures.
All authors have agreed to and significantly contributed to this case report.
All authors have read and approved the manuscript.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. We got the consent from the patient to participate in this study.
Consent for publication
The patient provided permission to publish the features of his case.
Competing interests
The authors declare that they have no competing interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Li J Guan W Ren W Longitudinal genomic alternations and clonal dynamics analysis of primary malignant melanoma of the esophagus. Neoplasia 2022; 30: 100811.35661532 10.1016/j.neo.2022.100811 PMC 9166384 · doi ↗ · pubmed ↗
- 2Dai L Wang ZM Xue ZQ Results of surgical treatment for primary malignant melanoma of the esophagus: a multicenter retrospective study. J Thorac Cardiovasc Surg 2021; 161: 294–302.10.1016/j.jtcvs.2020.03.00632359897 · doi ↗ · pubmed ↗
- 3Postow MA Chesney J Pavlick AC Nivolumab and ipilimumab versus ipilimumab in untreated melanoma. N Engl J Med 2015; 372: 2006–17.25891304 10.1056/NEJ Moa 1414428 PMC 5744258 · doi ↗ · pubmed ↗
- 4Weber JS D’Angelo SP Minor D Nivolumab versus chemotherapy in patients with advanced melanoma who progressed after anti-CTLA-4 treatment (Check Mate 037): a randomised, controlled, open-label, phase 3 trial. Lancet Oncol 2015; 16: 375–84.25795410 10.1016/S 1470-2045(15)70076-8 · doi ↗ · pubmed ↗
- 5Wolchok JD Chiarion-Sileni V Gonzalez R Overall survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med 2017; 377: 1345–56.28889792 10.1056/NEJ Moa 1709684 PMC 5706778 · doi ↗ · pubmed ↗
- 6Chang CY Park H Malone DC Immune checkpoint inhibitors and immune-related adverse events in patients with advanced melanoma: a systematic review and network meta-analysis. JAMA Netw Open 2020; 3: e 201611.32211869 10.1001/jamanetworkopen.2020.1611 PMC 7097702 · doi ↗ · pubmed ↗
- 7Endo F Akiyama Y Onishi M Primary esophageal malignant melanoma successfully treated with anti-PD-1 antibody for retroperitoneal recurrence after esophagectomy: a case report. Int J Surg Case Rep 2020; 75: 152–6.32950945 10.1016/j.ijscr.2020.09.034PMC 7508692 · doi ↗ · pubmed ↗
- 8Hanada K Tsunoda S Nomura M A case of long-term survival treated with three metastasectomies and two subsequent adjuvant nivolumab therapies for recurrent malignant melanoma of the esophagus. Surg Case Rep 2022; 8: 206.36333558 10.1186/s 40792-022-01561-z PMC 9636353 · doi ↗ · pubmed ↗