Troponin May Lie: Recognizing an Atypical Case of Wellens Syndrome
Juthipong Benjanuwattra, Cristian Castillo‐Rodriguez, Manisha Das, Shaheer Zulfiqar, Imran Arif

TL;DR
This paper discusses a rare heart condition called Wellens syndrome that can be missed due to misleading test results.
Contribution
The paper highlights the importance of recognizing Wellens syndrome despite normal or misleading ECG and troponin results.
Findings
Wellens syndrome can be missed if relying solely on ECG and troponin tests.
Urgent revascularization is critical for patients with this syndrome.
Noninvasive stress tests may be harmful if used inappropriately.
Abstract
Wellens syndrome is associated with a critical coronary artery stenosis and an impending extensive myocardial infarction. Despite having chest pain, both ECG and troponin can be misleading. It is crucial to recognize this syndrome to allow urgent revascularization. Failure to recognize and noninvasive stress tests were shown to be detrimental.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
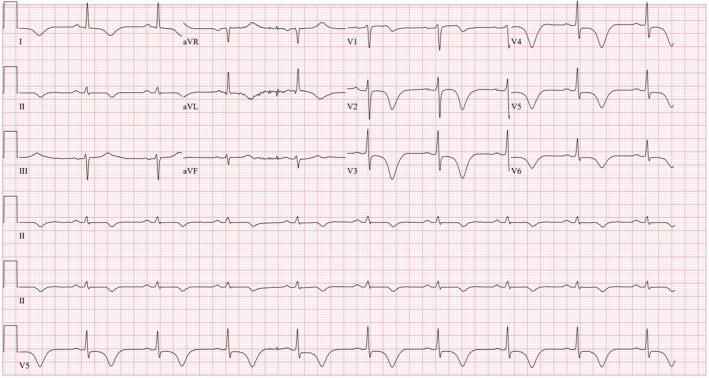 FIGURE 1
FIGURE 1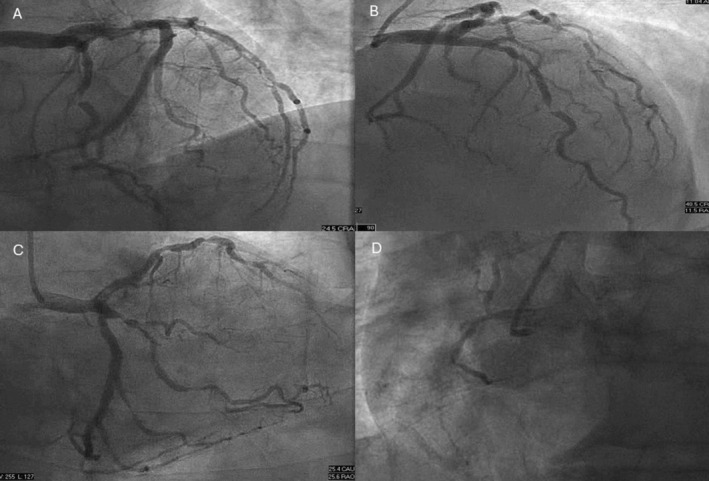 FIGURE 2
FIGURE 2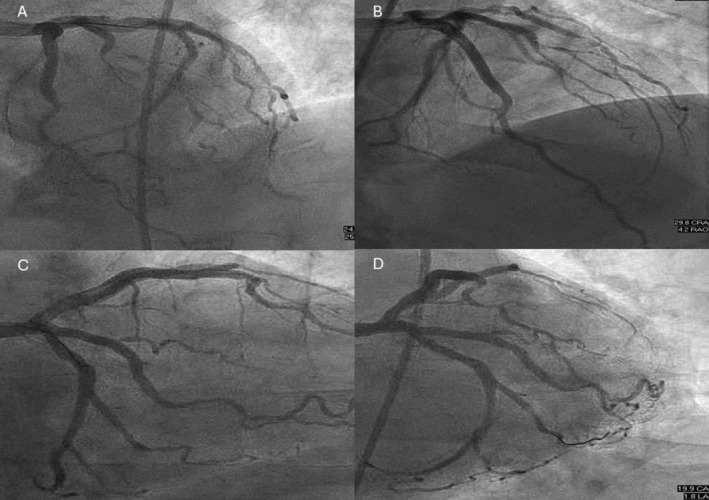 FIGURE 3
FIGURE 3| Time | First presentation | Second presentation (ng/L) |
|---|---|---|
| Arrival | 13 ng/L | 27 |
| 2 h after arrival | 15 ng/L | 33 |
| Delta 2 h | 2 ng/L | 6 |
| 5 h after arrival | n/a | 34 |
| Delta 3 h | n/a | 1 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Imaging and Diagnostics · Acute Myocardial Infarction Research · Cardiac electrophysiology and arrhythmias
Introduction
1
Wellens syndrome, which was first described by Zwaan and Wellens in 1982, signifies a critical stenosis in the left anterior descending coronary artery (LAD) with characteristic ECG features [1]. The diagnosis can be overlooked or delayed as patients often present in a pain‐free state, and troponin is also not a reliable marker.
Recently, a concept of occlusion myocardial infarction (OMI) was proposed to shift a paradigm away from solely relying on the presence of persistent ST‐segment elevation as an indication for emergent reperfusion, as only about 40% of acute OMI fulfill the ST‐elevation myocardial infarction (STEMI) criteria and up to 30% of non‐STEMI are found to have OMI [2]. Several ECG patterns predictive of OMI, without persistent ST‐segment elevation, include De Winter T waves, left bundle branch block meeting Sgarbossa criteria, diffuse ST‐segment depression with ST‐segment elevation in aVR, and, unsurprisingly, Wellens syndrome [3].
Hereby we present a case of a male patient with intermittent chest pain and unremarkable troponin, with Wellens syndrome and severe multivessel disease. The case highlights the importance of clinical awareness of this condition to allow timely diagnosis and revascularization.
Case History/Examination
2
A 70‐year‐old man with a history of hypertension, hyperlipidemia, prior stroke, and frontotemporal dementia presented with intermittent chest pain for the past 3 days. Three days prior, he had sharp substernal pain that resolved spontaneously within 20 min. Physical examination was normal. ECG did not show any specific ST‐T abnormality. High‐sensitivity troponin (hs‐cTn, Abbott) was at 13 ng/L, which was below the 99th percentile of the upper reference level (20 ng/L), and delta 2‐h of 2 ng/L. Based on the current guideline [4], acute myocardial infarction (MI) was ruled out, and he was discharged.
He then presented again with severe substernal pressure and dyspnea that lasted for 1 h. En route to the hospital, he was hypertensive to 200/100 mmHg. He received aspirin 325 mg. Upon arrival, he was normotensive and other vital signs were normal. Chest pain had resolved. Initial hs‐cTn was elevated but below the MI rule‐in value (27 ng/L) with a repeat hs‐cTn at 33 and 34 ng/L (delta 2‐ and 3‐h of 6 and 1 ng/L, respectively) (Table 1). ECG, which was obtained in a pain‐free state, showed sinus bradycardia with a prolonged QT interval and deeply inverted T waves across the precordial, I, II, and aVL leads (Figure 1). He was initially deemed to have demand ischemia associated with a hypertensive emergency. A noninvasive stress test was planned as a diagnostic test given that the patient had an intermediate risk with no known coronary disease [5]. However, several hours later, he developed a third episode of chest pain with blood pressure up to 200/100 mmHg. A heparin drip was started. Chest pain and hypertension were resolved with sublingual nitroglycerin.
ECG showing deep symmetrical T wave inversion across the precordial, I, and aVL leads, associated with prolonged QT interval.
Differential Diagnosis, Investigations, and Treatment
3
Cardiology was notified, and a decision was made to perform an urgent coronary angiogram because of a concern of Wellens syndrome, as suggested by the intermittent nature of chest pain and characteristic ECG findings.
Coronary angiogram revealed multivessel disease (Figure 2). There was a critical stenosis in the mid left anterior descending coronary artery (LAD) and the ostium of the first diagonal branch (D1), severe stenosis of the proximal segment of the first and second obtuse marginal (OM) branches, and chronic total occlusion of the RCA. Echocardiography, which was obtained after revascularization, showed normal function without wall motion abnormality.
Coronary angiogram showing critical 99% stenosis in the mid left anterior descending artery, critical stenosis of the first diagonal branch, and severe 95% stenosis of the proximal first obtuse marginal and second obtuse marginal branches (A–C). Chronic total occlusion of the right coronary artery was shown (D).
Outcomes and Follow‐Up
4
Patient underwent percutaneous coronary intervention (PCI) to the LAD and D1 with drug‐eluting stents. Staged PCI was later performed to both OM branches (Figure 3). There was no periprocedural MI or cardiovascular event during follow‐up.
Coronary angiogram showing TIMI‐3 flow in the left anterior descending artery, first diagonal, and both obtuse marginal branches following coronary intervention.
Discussion
5
Wellens syndrome is a condition with specific ECG patterns associated with critical stenosis of the LAD [1, 6]. The risk factors for Wellens syndrome include the traditional risk factors for coronary artery disease, such as hypertension, diabetes mellitus, dyslipidemia, obesity, smoking, and family history of premature coronary disease [7]. Interestingly, those with Wellens syndrome are less likely to have a personal history of coronary disease or previous PCI compared with non‐Wellens patients [7].
The ECG is characterized by biphasic T waves in leads V2–V3 (Type A) or primarily deeply inverted T waves in leads V2–V3 that can extend across all precordial leads (Type B) [1, 6]. The Type B pattern is much more common and represents approximately 75% of cases [8]. Other suggestive ECG features include absence of pathological precordial Q wave, preserved precordial R wave progression, and isoelectric or minimal ST‐segment elevation (< 1 mm) [9].
The finding of ST depression in multiple leads, particularly in eight or more leads, together with ST elevation in aVR and/or V1 is suggestive of severe multivessel or left main disease [10]. As in our case, there are widespread > 8 leads with T wave inversion, including lead I and aVL, with minimal ST elevation in V1, which is most likely explained by occlusion of LAD and OM branches. Another case report of Wellens syndrome with both LAD and proximal circumflex stenosis also exhibited T wave inversion in lead I and aVL [11].
The prevalence of Wellens syndrome in a cohort of patients with unstable angina was approximately 14% on the basis of a study conducted by de Zwaan et al. [8] over three decades ago. The proximal and mid LAD lesions were found to be culprits in 29% and 54% of patients, respectively. Multivessel disease was found in 22% of patients [8]. Among those who were not revascularized, approximately 30% of cases developed acute MI during follow‐up [6]. In the current era of hs‐cTn, the prevalence of Wellens syndrome has changed [7]. Based on a cohort of 2,127 patients with non ST‐elevation ACS from a culprit LAD, there were 200 patients (9.4%) fulfilling the ECG criteria for Wellens syndrome [7]. A relatively similar prevalence of 8.8% was reported from another retrospective cohort study [6]. The prevalence of multivessel disease did not differ between those with and without ECG characteristics of Wellens syndrome. However, based on this single center retrospective study, the prevalence of multivessel disease was almost four times higher than the previously reported prevalence of 22% [7]. The presence of the Wellens sign had a sensitivity of 24.6% and a specificity of 96.2% in predicting a culprit LAD lesion [6].
The characteristic feature of Wellens syndrome involves coronary artery stenosis with intermittent reperfusion and reocclusion that can develop over days to weeks, thus explaining the dynamic change of ECG findings and stuttering nature of chest pain [12]. Although not shown in our patient, clinicians must be aware that T wave may appear normal and upright during a period of reocclusion and active chest pain, which is described as “pseudonormalization.” Acute ST‐elevation MI can eventually develop if the artery remains occluded [12].
Patients typically present during a pain‐free state, with normal or slightly elevated cardiac biomarkers [9]. As in our patient, even hs‐cTn is falsely reassuring. Recognizing these ECG patterns and the nature of chest pain are crucial, as these patients require early coronary revascularization because of the imminent risk of extensive anterior wall STEMI [13]. Also, a stress test should be avoided as shown in a previous case who developed acute STEMI and cardiac arrest shortly after starting exercise [9].
Given that Wellens syndrome is associated with a large territory of jeopardized myocardium, clinical awareness of its ECG pattern is of paramount importance to allow timely coronary angiography and revascularization [1]. Care must be taken to avoid premature diagnostic closure, as a variety of cardiac and noncardiac conditions are also associated with precordial T wave inversion, such as Takotsubo cardiomyopathy, arrhythmogenic right ventricular dysplasia, hypertrophic cardiomyopathy, pulmonary embolism, and increased intracranial pressure [14].
Conclusion
6
Wellens syndrome is an urgent condition associated with imminent risk of acute extensive anterior wall STEMI. It can be diagnosed by appropriate clinical context and recognition of its ECG characteristics. Clinicians should not rely on cardiac biomarkers. In actively symptomatic patients, the ECG may not show the classic Wellens sign because of pseudonormalization. Clinical awareness is crucial to allow timely diagnosis and coronary revascularization.
Author Contributions
Juthipong Benjanuwattra: writing – original draft, writing – review and editing. Cristian Castillo‐Rodriguez: writing – original draft. Manisha Das: conceptualization, supervision, visualization. Shaheer Zulfiqar: supervision, writing – review and editing. Imran Arif: supervision, validation, writing – review and editing.
Consent
Written informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1C. de Zwaan , F. W. Bär , and H. J. Wellens , “Characteristic Electrocardiographic Pattern Indicating a Critical Stenosis High in Left Anterior Descending Coronary Artery in Patients Admitted Because of Impending Myocardial Infarction,” American Heart Journal 103, no. 4 Pt 2 (1982): 730–736, 10.1016/0002-8703(82)90480-x.6121481 · doi ↗ · pubmed ↗
- 2M. Y. Alsagaff , T. S. Putra , B. P. D. Khrisna , and R. A. Nugraha , “Case Report: Wellens Syndrome in Acute Critical Coronary Occlusion Saved by Collateral,” F 1000 Research 11 (2022): 1486.39109383 10.12688/f 1000 research.125820.3PMC 11301133 · doi ↗ · pubmed ↗
- 3M. Kola , N. Shuka , H. P. Meyers , E. Zaimi Petrela , and S. W. Smith , “OMI/NOMI: Time for a New Classification of Acute Myocardial Infarction,” Journal of Clinical Medicine 13, no. 17 (2024): 5201, 10.3390/jcm 13175201.39274412 PMC 11395726 · doi ↗ · pubmed ↗
- 4J. P. Collet , H. Thiele , E. Barbato , et al., “2020 ESC Guidelines for the Management of Acute Coronary Syndromes in Patients Presenting Without Persistent ST‐Segment Elevation,” European Heart Journal 42, no. 14 (2021): 1289–1367.32860058 10.1093/eurheartj/ehaa 575 · doi ↗ · pubmed ↗
- 5M. Gulati , P. D. Levy , D. Mukherjee , et al., “2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of CHEST Pain: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines,” Circulation 144, no. 22 (2021): e 336–e 367.10.1161/CIR.000000000000103034709928 · doi ↗ · pubmed ↗
- 6A. Kobayashi , N. Misumida , S. Aoi , and Y. Kanei , “Prevalence and Clinical Implication of Wellens' Sign in Patients With Non‐ST‐Segment Elevation Myocardial Infarction,” Cardiology Research 10, no. 3 (2019): 135–141.31236175 10.14740/cr 856PMC 6575113 · doi ↗ · pubmed ↗
- 7L. Zhou , X. Gong , T. Dong , H. H. Cui , H. Chen , and H. Li , “Wellens' Syndrome: Incidence, Characteristics, and Long‐Term Clinical Outcomes,” BMC Cardiovascular Disorders 22, no. 1 (2022): 176.35429969 10.1186/s 12872-022-02560-6PMC 9013025 · doi ↗ · pubmed ↗
- 8C. de Zwaan , F. W. Bär , J. H. Janssen , et al., “Angiographic and Clinical Characteristics of Patients With Unstable Angina Showing an ECG Pattern Indicating Critical Narrowing of the Proximal LAD Coronary Artery,” American Heart Journal 117, no. 3 (1989): 657–665, 10.1016/0002-8703(89)90742-4.2784024 · doi ↗ · pubmed ↗