Perceptions about COVID-19 vaccine among healthcare workers in Rwanda: A mixed-methods study
Erigene Rutayisire, François X. Ndayambaje, Sembuche Senga, Raji Tajudeen, Darius Uzabakiriho, Solange Nikwigize, Marie F. Muremba, Eric Remera, Tonny Muwonge, Leah Mbabazi, Rodgers R. Ayebare, Francis Kakooza, Tamrat Shaweno, Nebiyu Dereje, Elizabeth Gonese, Mosoka P. Fallah

TL;DR
This study explores healthcare workers' perceptions of the COVID-19 vaccine in Rwanda, finding overall positivity but also gaps in confidence.
Contribution
The study provides insights into vaccine perceptions among healthcare workers in a low-income country context.
Findings
Most healthcare workers in Rwanda had a positive perception of the COVID-19 vaccine.
A significant portion lacked confidence in addressing patient questions about the vaccine.
The findings suggest the need for educational interventions to improve vaccine confidence.
Abstract
Healthcare workers (HCWs) are crucial for coronavirus disease 2019 (COVID-19) vaccination programmes, but their perceptions of the vaccine, particularly in low-income countries, are underexplored. This study investigated HCWs perceptions of the COVID-19 vaccination in Rwanda. This study aimed to understand HCWs’ perceptions of the COVID-19 vaccine in Rwanda. A convergent mixed-methods study was conducted in 45 purposively selected health facilities in Rwanda. A sample of 230 HCWs was purposively calculated to include 45 health facilities from both rural and urban districts across Rwanda to participate in this study. Healthcare workers were selected conveniently ensuring representation of the different cadres. Furthermore, one participant per facility underwent an in-depth interview. Data were analysed using STATA 17 (quantitative) and Dedoose (qualitative) software. Descriptive…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
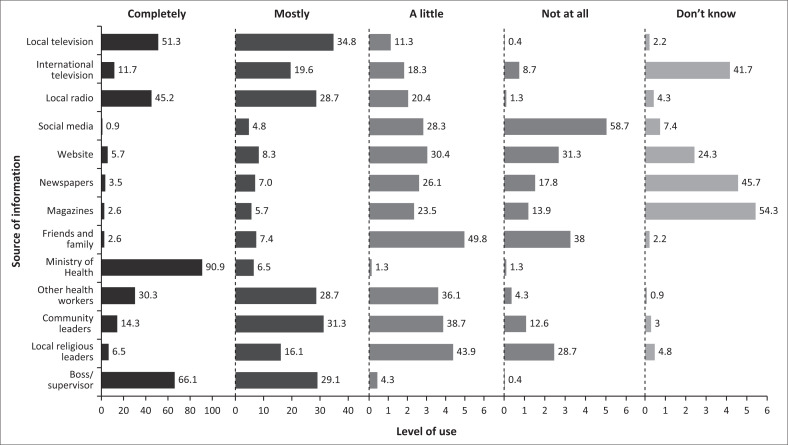 FIGURE 1
FIGURE 1| Variables | Frequency ( | Percentage | Mean | IQR |
|---|---|---|---|---|
|
| - | - | ||
| Female | 183 | 79.6 | - | - |
| Male | 47 | 20.4 | - | - |
|
| 39 | 33–44 | ||
| 21–29 | 32 | 13.9 | - | - |
| 30–39 | 93 | 40.4 | - | - |
| 40–49 | 75 | 32.6 | - | - |
| 50–62 | 30 | 13.0 | - | - |
|
| - | - | ||
| Urban | 139 | 60.4 | - | - |
| Semi-urban | 21 | 9.1 | - | - |
| Rural | 70 | 30.4 | - | - |
|
| - | - | ||
| Didn’t receive a booster dose | 4 | 1.7 | - | - |
| Received a booster dose | 226 | 98.3 | - | - |
|
| - | - | ||
| Physicians | 19 | 8.3 | - | - |
| Nursing and midwifery | 98 | 42.6 | - | - |
| Pharmaceutical personnel | 17 | 7.4 | - | - |
| Laboratory health workers | 33 | 14.4 | - | - |
| Community and public health workers | 22 | 9.6 | - | - |
| Other health workers | 41 | 17.8 | - | - |
|
| - | - | ||
| Health centre | 209 | 90.9 | - | - |
| Pharmacy | 3 | 1.3 | - | - |
| Community centre/Health post | 13 | 5.7 | - | - |
| Any other location designated by MoH | 21 | 9.1 | - | - |
| Indicators | Frequency ( | Percentage |
|---|---|---|
|
| ||
| Moderately easy | 9 | 3.9 |
| Not at all easy | 3 | 1.3 |
| Very easy | 218 | 94.8 |
|
| ||
| Definitely recommend | 216 | 93.9 |
| I do not know | 2 | 0.9 |
| Probably not recommend | 1 | 0.4 |
| Probably recommend | 11 | 4.8 |
|
| ||
| I would not recommend booster vaccine dosing | 2 | 0.9 |
| I would recommend booster vaccine doses recommended by the WHO | 87 | 37.8 |
| I would recommend some booster vaccine schedules and not others | 18 | 7.8 |
| I would recommend the booster vaccine doses recommended by the MoH in my country | 123 | 53.5 |
|
| ||
| A little confident | 54 | 23.5 |
| Moderately confident | 84 | 36.5 |
| Not at all confident | 5 | 2.2 |
| Very confident | 87 | 37.8 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMiddle East and Rwanda Conflicts
Introduction
The coronavirus disease 2019 (COVID-19) pandemic emerged and rapidly spread through the world in early 2020. In a swift global response, efficacious vaccines were developed and distributed worldwide in late 2020 to control the pandemic.^1^ The burden of COVID-19 in Rwanda is characterised by 133 518 cases and 1468 deaths of COVID-19 reported by the World Health Organization (WHO) as of 13 January 2024. A total of 27.3 million vaccine doses have been administered, and 84% of the eligible population has completed the primary vaccine schedule.^2^ Rwanda received the first batch of 1000 doses of COVID-19 vaccines from Moderna in mid-February 2021. Furthermore, on 03 March 2021, Rwanda received 240 000 doses of the AstraZeneca-Oxford COVID-19 vaccine, followed by the first 102 960 doses of the Pfizer vaccine in Africa through the COVAX initiative.^3^
Healthcare workers (HCWs) are at the frontline of the response to health emergencies and pandemics such as the COVID-19 pandemic. They commonly care for patients and control the virus’s spread.^4^ In addition to their natural exposure to risk factors as part of the community and because of the nature of their work and the direct contact with patients infected with different pathogens, frontline HCWs are at high risk of acquiring a wide range of infections, including COVID-19.^5,6^ Because of the high risk of infection and their crucial role in implementing disease prevention and control measures, including immunisation programmes, HCWs were among the first groups to receive the COVID-19 vaccine in Rwanda.^3^ Despite having early access to vaccines and facing both national regulations and institutional mandates for HCW vaccination, the readiness of HCWs to receive the vaccine themselves or to recommend it to their patients remains unclear.
Nevertheless, HCWs play a critical role in promoting health practices in the community, including vaccine acceptance. They are often a trusted source of information for patients and the public.^7^ Therefore, their perceptions and beliefs may influence the message they share with the patients and community. Studies have shown that HCWs who are vaccinated themselves are more likely to promote and advocate for vaccine uptake among their patients and communities.^8,9^
However, there is limited evidence on the perceptions of COVID-19 vaccines among HCWs in low- and middle-income countries (LMICs), including Rwanda. A study done in Ethiopia found that about 40% of HCWs had a negative perception of the COVID-19 vaccine; similarly, this was 34 % in Singapore.^10,11^
As HCWs’ perceptions about COVID-19 vaccines play a key influential role in the vaccine’s acceptability and uptake among their communities, it is crucial to understand their perceptions and underlying beliefs to implement vaccination programmes successfully. Therefore, in this study, we explore HCWs’ perceptions towards COVID-19 vaccination in Rwanda.
The overall objective of this study was to explore the HCW’s perceptions towards COVID-19 vaccines. Specifically, HCWs ability to communicate with patients and trusted sources about COVID-19 vaccine information. Our study was guided by the following research questions:
What are the trusted sources of COVID-19 vaccine information?
What is the ability of the HCWs to communicate with patients about COVID-19 vaccine?
Are HCWs willing to recommend COVID-19 vaccine to others?
Research methods and design
Study design and setting
This was a cross-sectional convergent mixed-methods study involving both primary quantitative and qualitative data collection. The study was conducted in Rwanda, a low-income country with a population of 13 246 394 as of August 2022.^12^ Rwanda’s healthcare system is led by the Ministry of Health and includes various institutions managing policies and resources. The country has a network of public and private health facilities providing various healthcare services.^13^
Study population and sampling strategy
A sample of 230 HCWs was purposively estimated. Healthcare workers were sampled from 45 health facilities from both rural and urban districts across Rwanda to participate in this study. Healthcare workers were selected conveniently ensuring adequate representation of the different cadres from various geographic locations, both rural and urban, as well as different types of facilities. The inclusion criteria required participants to be HCWs aged 18 years and older who provided informed consent. For the qualitative aspect of the study, one key informant, an HCW actively involved in managing COVID-19 cases during the pandemic, was selected from each of the 45 health facilities, resulting in a total of 45 key informants.
Data collection
The data collection tools were developed following the ‘WHO – Evaluation of COVID-19 Vaccine Effectiveness Guide (2021)’^14^ and validated through a pilot session to ensure their relevance to the research questions. A structured questionnaire based on the behavioural and social drivers model^15^ was used to collect data on demographics including gender (male or female), age in complete years, number of vaccination doses received, vaccination experiences, perceptions and information sources (Appendix 1). It explored the likelihood of recommending the vaccine, confidence in addressing patient queries, barriers to vaccination and reasons for hesitancy or refusal. Furthermore, it asked about trust levels in various information sources about COVID-19 and vaccinations. Within each health facility, five HCWs who had direct interactions with COVID-19 patients were randomly selected for participation in the quantitative phase using a simple random sampling method. The data collection process was meticulous, ensuring the reliability and validity of the quantitative data through data collector training and support supervision along with continuous data audits and cleaning. Data were collected within 3 months, from 08 May 2023 to 02 July 2023 and entered into REDcap, an online data management platform, promptly. Trained researchers conducted qualitative interviews to ensure consistency and rigorous data collection.
In-depth interviews were conducted with 45 key informants (one from each health facility selected) to explore their perspectives in more detail. Interviews were audio-recorded and transcribed, with one exception where detailed notes were used. The interviews allowed flexibility in exploring the key informants’ perspectives and perceptions towards COVID-19 vaccination, ensuring a rich and comprehensive qualitative dataset. The interviews were conducted within the key informants’ places of work to create a comfortable and familiar setting, promoting open and honest discussions. Almost all interviews were conducted in the local ‘Kinyarwanda’ language, and only one was conducted in English. Transcription was done in Kinyarwanda and then back-translated to English by an independent consultant to ensure reliability.
Data analysis
The data analysis was conducted using STATA version 17 (StataCorp, College Station, Texas, United States [US]) for the quantitative portion, where descriptive statistics such as frequencies and percentages were employed to summarise the findings; graphical representations were also created to enhance the understanding of the data. For the qualitative analysis, an external consultant was engaged to code and analyse the data using Dedoose software (University of California, Los Angeles, Unites States [US]), which helped reduce bias in the process. An inductive thematic analysis was then performed to identify key themes within the coded data.
Ethical considerations
Ethical approval to conduct this study was obtained from the Rwanda National Research Ethics Committee (RNEC) (IRB 00001497 of IORG0001100; Ref No.100/ RNEC/2023). Written informed consent was obtained from all participants after providing them with information about the study. Data were anonymised to ensure participant confidentiality.
Results
Of the 230 HCWs, 183 (79.6%) were female and 47 (20.4%) were male. The majority of HCWs, 93 (40.4%), were aged between 30 years and 39 years, and the median (interquartile range [IQR]) age was 39 (33–44) years. The study enrolled 98 (42.6%) nurses and midwives. Participants from health centres located in urban areas were 139 (60.4%), whereas 21 (9.2%) and 70 (30.4%) were in semi-urban and rural areas, respectively. All participants in this study were fully vaccinated, and most had received a booster, with only four (1.7%) having not received the booster dose (Table 1).
Most HCWs, 209 (90.9%), were comfortable receiving the vaccine at the health centre. In comparison, 21 (9.1%) healthcare providers were comfortable receiving the vaccine from any other location designated by the Ministry of Health (MoH) (Table 1). Participants also shared that the community preferred receiving the vaccines from health facilities, as one midwife described in an in-depth interview:
‘The vaccines were found at the health centres or vaccination sites set up by MoH/RBC, but most people preferred to come to the health centre; of course, they are used to coming here.’ (HCW02, female, midwife)
During the COVID-19 pandemic, different communication platforms were used to disseminate related information. In this study, 209 (90.9%) HCWs said they had complete trust in the information about COVID-19 and vaccination provided by the Rwanda MoH, and 152 (66.1%) HCWs had complete confidence in the information provided by their supervisors. However, most HCWs, 135 (58.7%), did not trust information about COVID-19 on social media (Figure 1). The key informants reiterated the doubt in social media information and strong trust in government information sources as expressed by this participant:
‘The Vaccine came before we were prepared for it. We doubted at first time because of wrong information that was shared on social media and networking sites, newspapers and on the radio where you heard about vaccines and the people who refused to have them but when we heard some news on radio and television, we knew that our leaders would not give something wrong to their people.’ (HCW34, female, nurse)
Trust in information sources about coronavirus disease 2019 and vaccination.
According to 218 (94.8%) HCWs, COVID-19 vaccination services were easily accessible (Table 2). Key informants emphasised that they were accessible because there was access to transport modes such as motorcycles and that the requirements to attain vaccination were easy:
‘We have had no problem getting the COVID-19 vaccine. First, at the District Hospital, they are available; if they are not available there, they give us the schedule, and we go to the command post so that we would never miss the vaccines whenever we need them. We never had that case. Also, the Ministry of Health has created an easy way to get these vaccines because it provides us with transportation.’ (HCW14, male, nurse)
A total of 206 (89.6%) HCWs believed that being vaccinated against COVID-19 reduces the risk of a person getting sick or dying, and 216 (93.9%) HCWs agreed that they would recommend COVID-19 vaccination to community members. A total of 87 (37.8%) HCWs said that they would recommend booster vaccine doses recommended by the WHO, and 123 (53.5%) HCWs would recommend those recommended by the Rwanda MoH (see Table 2). Moreover, the key informants emphasised their willingness to encourage community members to take on the vaccines:
‘Our role is to show them/patients the benefits of the vaccine and usually talk about it at health centres and hospitals so that those people who have not taken vaccine could take it.’ (HCW31, female, nurse)
While 54 (23.5%) HCWs reported little confidence in answering patient questions about COVID-19 and vaccines, 87 (37.8%) HCWs reported that they would be very confident in doing so (see Table 2). However, the in-depth interviews with key informants revealed that because of limited knowledge of the vaccines, they were unsure how to respond to patient queries about the COVID-19 vaccines, as expressed by one nurse:
‘As the vaccine caused concern, people were worried because it was the first vaccine that entered the population, then there was no one else, let’s say a doctor, we did not know what side effects were, we had no experience with it, so when someone came to you and told you that he had a problem, you tried to explain to him because it was in the system, you go If you look at Google, there are times when you see something wrong because there is no reliable information about it, there are no experts.’ (HCW43, female, nurse)
Discussion
This study explored HCWs’ perceptions of COVID-19 vaccination in Rwanda. The findings offer valuable insights into their level of trust in information sources, confidence in vaccines and willingness to recommend vaccination to the community. They align with broader research on HCW vaccine hesitancy.
The results demonstrated a high trust in the MoH and a preference for health facilities for vaccination. The majority of HCWs expressed trust in information from the Rwanda MoH and preferred receiving vaccines at health facilities. This contradicts the findings from other sub-Saharan African countries where low trust in the MoH and Government was reported.^16,17^ High trust in government information sources on COVID-19 has been chiefly consistent with findings from high-income countries such as the United States.^18^ Trust in formal information sources about COVID-19 has previously been found to influence vaccine uptake.^19^ Therefore, the trust reported by the participants could explain the 100% vaccination coverage in this group.
This study also highlighted concerns about misinformation and lack of confidence in COVID-19 vaccines. This is consistent with global trends reported in Germany,^20^ India,^21^ and in a global review,^22^ highlighting the widespread challenge of misinformation and its impact on vaccine hesitancy among HCWs.
Concerning accessibility, the study found that HCWs perceived COVID-19 vaccination services as readily accessible. This differs from the experiences reported in neighbouring Kenya and South Africa, where a study found that less than a quarter of the HCWs reported that accessing vaccination services for themselves was easy.^23^ The reported higher accessibility to vaccination services could be attributed to Rwanda’s strong health governance and policy implementation^24,25^ that was applied to implementing COVID-19 vaccination mandates for HCWs. In addition, the majority (over 90%) expressed willingness to recommend vaccination to community members, demonstrating their commitment to promoting public health, as observed in studies from Ghana^26^ and Jordan.^27^
Limitations in addressing patient questions: Despite their willingness, a significant proportion of HCWs (23%) reported limited confidence in answering patient questions about COVID-19 and vaccines. This echoes concerns raised in Kenya^28^ and Angola,^29^ highlighting the need for targeted training programmes to equip HCWs with the knowledge and skills to address vaccine-related inquiries effectively. Similarly, in Japan, a study revealed that HCWs had low confidence regarding COVID-19 care.^30^ This was also demonstrated in another study where only 39.4% of HCWs showed adequate self-confidence in applying infection control COVID-19 measures.^31^
The findings of this study highlight the importance of addressing misinformation through effective communication strategies that are tailored to the concerns and preferred information channels of HCWs. It is crucial to build trust in COVID-19 vaccines by providing accurate information that emphasises their benefits and addresses specific concerns raised by HCWs, which underscores the necessity of pharmacovigilance programmes. Moreover, equipping HCWs with the knowledge and skills needed to confidently answer patients’ questions about COVID-19 and vaccines can be achieved through targeted training programmes. Future studies should explore the specific reasons for HCWs’ lack of confidence in COVID-19 vaccines within the Rwandan context, considering potential differences across various professional cadres and regions. Researchers should also identify the most effective communication strategies to combat misinformation and build trust among HCWs in Rwanda, taking into account the local media landscape and information consumption habits. Finally, assessing the impact of training programmes on HCWs’ confidence in addressing patient inquiries about COVID-19 and vaccines will be important, including measuring changes in knowledge, attitudes and self-reported confidence. By addressing these issues and building upon existing research, Rwanda’s policymakers and public health officials can develop targeted interventions to improve vaccine confidence and uptake among HCWs and the broader community, ultimately contributing to the success of COVID-19 vaccination efforts and other initiatives aimed at preventing vaccine-preventable diseases.
This study’s limitation is that the focus was restricted solely to HCWs, overlooking the broader spectrum of multisectoral involvement. Consequently, the findings may not reflect a comprehensive explanation for the remarkable success of the vaccination programme in Rwanda.
Conclusion
Understanding and addressing the perceptions of HCWs regarding the COVID-19 vaccine is crucial for effective vaccination campaigns, public health strategies and overall pandemic control. The overwhelming positive perceptions of the COVID-19 vaccine among Rwandans HCW echo the massive adoption of the COVID-19 vaccine in Rwanda. Such exceptional positive perceptions about COVID-19 vaccines among HCWs warrant further analyses to explore the promoting factors, including the broad spectrum that led to Rwanda’s super successful vaccination programme. We recommend maintaining open and transparent communication about vaccine distribution, safety and effectiveness, especially for new vaccines.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mathieu E, Ritchie H, Rodés-Guirao L, et al. Coronavirus pandemic (COVID-19). Our world in data [homepage on the Internet]. 2020 [cited 2024 Mar 14]. Available from: https://ourworldindata.org/coronavirus
- 2WHO. COVID-19 Rwanda situation. WHO COVID-19 dashboard [homepage on the Internet]. [cited 2024 Mar 14]. Available from: https://data.who.int/dashboards/covid 19/cases?m 49=646&n=c
- 3Nsanzabaganwa C, Bigirimana N, Hitimana N, et al. Rwanda COVID-19 vaccination program implementation [homepage on the Internet]. Kigali; 2021 [cited 2024 Mar 14]. Available from: https://rbc.gov.rw/publichealthbulletin/img/RPHB%20Vol.%203,%20issue%201.%20pp 7-9.pdf
- 4Hoernke K, Djellouli N, Andrews L, et al. Frontline healthcare workers’ experiences with personal protective equipment during the COVID-19 pandemic in the UK: A rapid qualitative appraisal. BMJ Open. 2021;11:e 046199. 10.1136/bmjopen-2020-046199 PMC 781884033472794 · doi ↗ · pubmed ↗
- 5Moyo I, Mavhandu-Mudzusi AH, Haruzivishe C. Frontline healthcare workers’ experiences of providing care during the COVID-19 pandemic at a COVID-19 centre in Bulawayo, Zimbabwe: A phenomenological study. Curationis. 2022;45(1):e 1–e 11. 10.4102/curationis.v 45i 1.2292 PMC 925768435792610 · doi ↗ · pubmed ↗
- 6Nguyen LH, Drew DA, Graham MS, et al. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health [serial online]. 2020 [cited 2024 Mar 14];5:e 475–e 483. Available from: http://www.thelancet.com/article/S 246826672030164 X/fulltext 32745512 10.1016/S 2468-2667(20)30164-XPMC 7491202 · doi ↗ · pubmed ↗
- 7Niyigena A, Nyirahabimana N, Cubaka V, et al. Knowledge and practices surrounding outbreaks and COVID-19 among community health workers in rural Rwanda: A cross-sectional mixed-methods study. Pan Afr Med J. 2023;45:35. 10.11604/pamj.2023.45.35.3702037545611 PMC 10403765 · doi ↗ · pubmed ↗
- 8Alhassan RK, Owusu-Agyei S, Ansah EK, Gyapong M. COVID-19 vaccine uptake among health care workers in Ghana: A case for targeted vaccine deployment campaigns in the global south. Hum Resour Health. 2021;19:1–12. 10.1186/s 12960-021-00657-134742301 PMC 8571849 · doi ↗ · pubmed ↗