Identification of Risk Factors for Postoperative Hypotension Following Transurethral Bladder Tumor Resection Performed With Oral 5-Aminolevulinic Acid: A Multivariate Analysis of a Single-Center Retrospective Cohort Study
Takashi Oshikawa, Toyoaki Maruta, Go Otao, Isao Tsuneyoshi

TL;DR
This study identifies risk factors for postoperative low blood pressure after bladder tumor surgery using 5-ALA, focusing on kidney function and pre-surgery blood pressure.
Contribution
The study is the first to identify risk factors specifically for postoperative hypotension following TUR-Bt with 5-ALA.
Findings
Impaired renal function (eGFR ≤ 45-60 or < 45 mL/min/1.73 m2) increases risk of postoperative hypotension.
Lower preoperative mean blood pressure (< 95 mmHg) is associated with higher risk of postoperative hypotension.
Risk factors were consistent across both general and spinal anesthesia groups.
Abstract
Background Transurethral resection of bladder tumors (TUR-Bt) using 5-aminolevulinic acid (5-ALA) is increasingly performed to visualize tumors. However, oral administration of 5-ALA frequently induces perioperative hypotension. Although several risk factors for intraoperative hypotension have been reported, those associated with postoperative hypotension have not yet been identified. We retrospectively evaluated risk factors for postoperative hypotension following TUR-Bt with 5-ALA administration. Methods The enrolled participants were patients who underwent TUR-Bt with 5-ALA under general or spinal anesthesia between July 2020 and December 2023. Patients who developed postoperative hypotension or used postoperative vasopressors were assigned to the hypotension group, and those who did not were assigned to the non-hypotension group. Postoperative mean blood pressure (mBP) was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
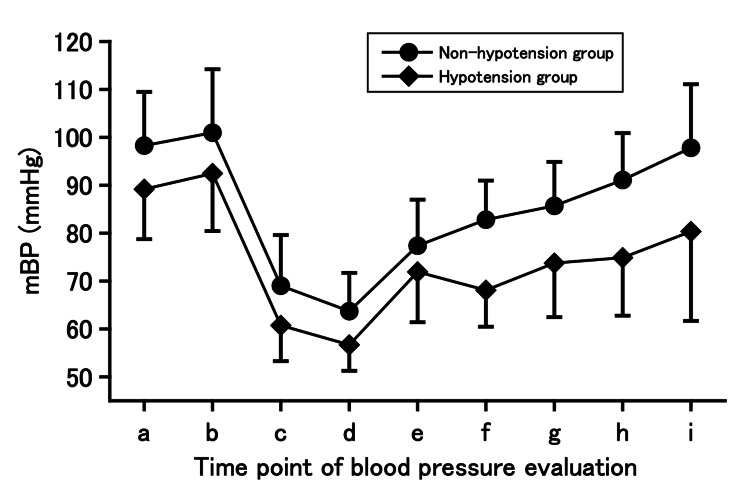 Figure 1
Figure 1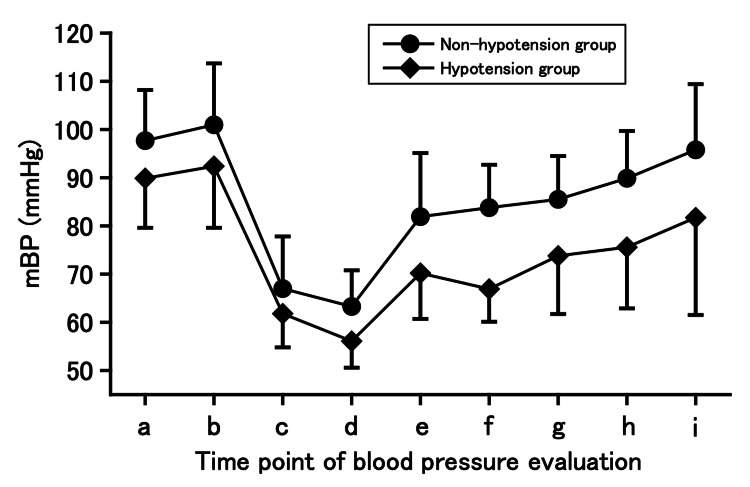 Figure 2
Figure 2| Variables | Non-hypotension group | Hypotension group |
| ||
| n | Data | n | Data | ||
| Patient characteristics | |||||
| Age (years), median (IQR) | 65 | 73.0 (66.5–81.0) | 46 | 73.0 (68.0–80.0) | 0.579 |
| Sex | 65 | 46 | 0.296 | ||
| Male, n (%) | 52 (80.0) | 41 (89.1) | |||
| Female, n (%) | 13 (20.0) | 5 (10.9) | |||
| Height (cm), median (IQR) | 65 | 163.4 (157.0–171.7) | 46 | 163.8 (159.6–167.6) | 0.790 |
| Weight (kg), median (IQR) | 65 | 61.0 (52.4–72.5) | 46 | 65.5 (57.3–68.2) | 0.088 |
| BMI (kg/m2), median (IQR) | 65 | 23.4 (20.6–25.8) | 46 | 24.1 (22.4–25.6) | 0.197 |
| ASA-PS | 65 | 46 | 0.618 | ||
| 1, n (%) | 1 (1.5) | 2 (4.3) | |||
| 2, n (%) | 58 (89.2) | 41 (89.1) | |||
| 3, n (%) | 6 (9.2) | 3 (6.5) | |||
| Hemoglobin (g/dL), median (IQR) | 65 | 14.1 (12.6–15.5) | 46 | 13.7 (12.3–15.2) | 0.320 |
| Hematocrit (%), median (IQR) | 65 | 42.1 (39.3–45.6) | 46 | 41.7 (37.4–44.9) | 0.417 |
| eGFR (mL/min/1.73 m2), median (IQR) | 64 | 64.5 (54.0–74.8) | 44 | 54.0 (43.0–68.5) | 0.008 |
| ≥ 60, n (%) | 40 (62.5) | 16 (36.4) | 0.017 | ||
| 45–60, n (%) | 15 (23.4) | 14 (31.8) | |||
| < 45, n (%) | 9 (14.1) | 14 (31.8) | |||
| Comorbidity | 65 | 46 | |||
| Hypertension, n (%) | 39 (60.0) | 26 (56.5) | 0.845 | ||
| Heart disease, n (%) | 7 (10.8) | 5 (10.9) | > 0.999 | ||
| Diabetes mellitus, n (%) | 12 (18.5) | 8 (17.4) | > 0.999 | ||
| End stage of renal disease, n (%) | 1 (1.5) | 2 (4.3) | 0.569 | ||
| Medication | 65 | 46 | |||
| RASI, n (%) | 27 (41.5) | 17 (37.0) | 0.696 | ||
| Calcium channel blocker, n (%) | 32 (49.2) | 23 (50.0) | > 0.999 | ||
| α-blocker, n (%) | 6 (9.2) | 5 (10.9) | 0.760 | ||
| β-blocker, n (%) | 7 (10.8) | 4 (8.7) | > 0.999 | ||
| Diuretic, n (%) | 5 (7.7) | 2 (4.3) | 0.697 | ||
| Perioperative data | |||||
| Anesthesia method | 65 | 46 | 0.640 | ||
| General, n (%) | 15 (23.1) | 8 (17.4) | |||
| Spinal, n (%) | 50 (76.9) | 38 (82.6) | |||
| Operation time (min), median (IQR) | 65 | 50.0 (35.0–64.3) | 46 | 48.0 (28.8–69.0) | 0.635 |
| Anesthesia time (min), median (IQR) | 65 | 77.0 (60.0–93.5) | 46 | 77.5 (50.8–95.0) | 0.722 |
| Infusion volume | 65 | 46 | |||
| Preoperative infusion volume (mL), median (IQR) | 0.0 (0.0–0.0) | 0.0 (0.0–162.5) | 0.072 | ||
| Intraoperative infusion volume (mL), median (IQR) | 700.0 (500.0–900.0) | 825.0 (637.5–1200.0) | 0.024 | ||
| Postoperative infusion volume up to 6 h (mL), median (IQR) | 480.0 (480.0–480.0) | 480.0 (480.0–480.0) | 0.806 | ||
| Intraoperative vasopressor | 65 | 46 | |||
| Ephedrine (mg), median (IQR) | 8.0 (0.0–12.0) | 12.0 (0.0–16.0) | 0.204 | ||
| Phenylephrine (mg), median (IQR) | 0.0 (0.0–0.1) | 0.2 (0.0–0.6) | 0.006 | ||
| Dopamine, n (%) | 0.0 (0.0) | 3.0 (7.3) | 0.080 | ||
| Dobutamine, n (%) | 1.0 (1.9) | 2 (5.0) | 0.573 | ||
| Norepinephrine, n (%) | 3.0 (5.5) | 6.0 (14.3) | 0.163 | ||
| Analgesic drug | 65 | 46 | |||
| Fentanyl, n (%) | 16.0 (24.6) | 9.0 (19.6) | 0.646 | ||
| Pentazocine, n (%) | 13.0 (26.0) | 9 (23.7) | > 0.999 | ||
| Blood pressure | 65 | 46 | |||
| mBP before administration of 5-ALA, median (IQR) | 96.3 (91.5–104.3) | 91.8 (79.4–95.8) | < 0.001 | ||
| mBP upon entering the operating room, median (IQR) | 101.0 (90.8–107.5) | 92.5 (85.0–101.2) | 0.001 | ||
| Minimum mBP before starting operation, median (IQR) | 65.3 (58.0–74.7) | 60.7 (56.0–65.4) | 0.003 | ||
| Minimum mBP after starting operation, median (IQR) | 62.3 (58.2–66.6) | 56.5 (52.8–59.8) | < 0.001 | ||
| mBP upon leaving the operating room, median (IQR) | 78.3 (71.7–88.5) | 70.2 (64.4–75.8) | < 0.001 | ||
| mBP 1 h after surgery, median (IQR) | 82.3 (76.2–89.2) | 67.8 (62.6–73.3) | < 0.001 | ||
| mBP 2 h after surgery, median (IQR) | 85.0 (78.2–91.3) | 73.5 (68.5–81.1) | < 0.001 | ||
| mBP 3 h after surgery, median (IQR) | 87.7 (82.0–97.3) | 71.0 (66.2–82.4) | < 0.001 | ||
| mBP 6 h after surgery, median (IQR) | 95.0 (85.3–104.2) | 80.7 (72.0–91.7) | < 0.001 | ||
| Use of postoperative vasopressors, n (%) | 65 | 0.0 (0.0) | 46 | 13.0 (28.3) | < 0.001 |
| Postoperative complications, n (%) | 65 | 6.0 (9.2) | 46 | 7.0 (15.2) | 0.379 |
| Classification | Nausea and vomiting, 7 cases; delirium, 1 case | Nausea and vomiting, 4 cases; delirium, 1 case; headache, 2 cases | |||
| Factor | Cases ( | Univariate analysis | ||
| OR | 95% CI |
| ||
| Patient characteristics | ||||
| Age (years) | 133 | 1.024 | 0.983–1.067 | 0.250 |
| Sex | 133 | |||
| Male | 1.000 | ref | ||
| Female | 0.465 | 0.148–1.464 | 0.189 | |
| Height | 133 | 1.017 | 0.974–1.061 | 0.441 |
| Weight | 133 | 1.018 | 0.989–1.047 | 0.220 |
| Body mass index | 133 | 1.071 | 0.968–1.184 | 0.180 |
| ASA-PS | 133 | |||
| 1 | 1.000 | ref | ||
| 2 | 0.670 | 0.080–5.598 | 0.710 | |
| 3 | 0.508 | 0.039–6.554 | 0.601 | |
| Hemoglobin | 133 | 0.899 | 0.720–1.124 | 0.347 |
| Hematocrit | 133 | 0.969 | 0.893–1.052 | 0.448 |
| eGFR | 130 | 0.968 | 0.946–0.991 | 0.006 |
| ≥ 60 mL/min/1.73 m2 | 1.000 | ref | ||
| 45–60 mL/min/1.73 m2 | 3.131 | 1.256–7.806 | 0.015 | |
| < 45 mL/min/1.73 m2 | 4.131 | 1.463–11.664 | 0.008 | |
| Comorbidity | 133 | |||
| Hypertension | 1.064 | 0.496–2.281 | 0.872 | |
| Heart disease | 1.105 | 0.305–3.994 | 0.879 | |
| Diabetes mellitus | 1.511 | 0.585–3.900 | 0.391 | |
| End stage of renal disease | 3.176 | 0.242–41.632 | 0.376 | |
| Medication | 133 | |||
| RASI | 1.129 | 0.522–2.444 | 0.756 | |
| Calcium channel blocker | 0.964 | 0.454–2.051 | 0.925 | |
| α-blocker | 1.532 | 0.503–4.662 | 0.450 | |
| β-blocker | 0.863 | 0.220–3.377 | 0.831 | |
| Diuretic | 1.239 | 0.286–5.363 | 0.773 | |
| Perioperative data | ||||
| Anesthesia method | 133 | |||
| General | 1.000 | ref | ||
| Spinal | 1.808 | 0.689–4.744 | 0.227 | |
| Operation time | 133 | 0.998 | 0.983–1.013 | 0.801 |
| Anesthesia time | 133 | 0.997 | 0.983–1.010 | 0.625 |
| Preoperative infusion volume | 133 | 1.001 | 0.999–1.004 | 0.284 |
| Intraoperative infusion volume | 133 | 1.001 | 1.000–1.002 | 0.025 |
| Intraoperative vasopressor | 133 | |||
| Ephedrine | 1.019 | 0.974–1.065 | 0.410 | |
| Phenylephrine | 1.261 | 0.609–2.610 | 0.529 | |
| Dopamine | 4.623 | 0.407–52.512 | 0.214 | |
| Dobutamine | 2.897 | 0.221–38.051 | 0.415 | |
| Noradrenaline | 3.642 | 0.819–16.186 | 0.089 | |
| Analgesic drug | 133 | |||
| Fentanyl | 0.596 | 0.235–1.511 | 0.237 | |
| Pentazocine | 0.809 | 0.321–2.040 | 0.650 | |
| Blood pressure | 133 | |||
| mBP before administration of 5-ALA | 0.936 | 0.899–0.973 | 0.002 | |
| mBP before administration of 5-ALA < 95 mmHg | 2.815 | 1.287–6.158 | 0.010 | |
| mBP upon entering the operating room | 0.938 | 0.906–0.971 | < 0.001 | |
| mBP upon entering the operating room < 95 mmHg | 3.442 | 1.580–7.497 | 0.002 | |
| Factor | Multivariate analysis | ||
| OR | 95% CI |
| |
| eGFR | |||
| ≥ 60 mL/min/1.73 m2 | 1.000 | ref | |
| 45–60 mL/min/1.73 m2 | 3.026 | 1.140–8.003 | 0.027 |
| < 45 mL/min/1.73 m2 | 4.851 | 1.550–15.177 | 0.007 |
| Blood pressure | |||
| mBP before administration of 5-ALA < 95 mmHg | 2.367 | 0.976–5.740 | 0.056 |
| mBP upon entering the operating room < 95 mmHg | 2.443 | 1.018–5.865 | 0.046 |
| Variables | Non-hypotension group | Hypotension group |
| ||
| n | Data | n | Data | ||
| Patient characteristics | |||||
| Age (years), median (IQR) | 50 | 73.5 (67.0–80.5) | 38 | 74.5 (68.0–80.3) | 0.673 |
| Sex | 50 | 38 | 0.252 | ||
| Male, n (%) | 39 (78.0) | 34 (89.5) | |||
| Female, n (%) | 11 (22.0) | 4 (10.5) | |||
| Height (cm), median (IQR) | 50 | 165.6 (157.0–171.9) | 38 | 163.8 (160.0–167.6) | 0.804 |
| Weight (kg), median (IQR) | 50 | 61.4 (52.4–71.9) | 38 | 66.4 (57.9–69.2) | 0.045 |
| BMI (kg/m2), median (IQR) | 50 | 23.6 (20.6–25.5) | 38 | 24.1 (22.8–26.6) | 0.090 |
| ASA-PS | 50 | 38 | 0.520 | ||
| 1, n (%) | 1 (2.0) | 4 (10.5) | |||
| 2, n (%) | 45 (76.0) | 27 (71.1) | |||
| 3, n (%) | 4 (22.0) | 7 (18.4) | |||
| Hemoglobin (g/dL), median (IQR) | 50 | 14.2 (13.4–15.4) | 38 | 13.7 (12.3–15.3) | 0.225 |
| Hematocrit (%), median (IQR) | 50 | 42.3 (39.9–45.5) | 38 | 40.8 (37.2–45.2) | 0.205 |
| eGFR (mL/min/1.73 m2), median (IQR) | 50 | 63.0 (54.0–74.5) | 38 | 54.0 (42.3–66.0) | 0.011 |
| ≥ 60, n (%) | 31 (63.3) | 13 (36.1) | 0.007 | ||
| 45–60, n (%) | 12 (24.5) | 11 (30.6) | |||
| < 45, n (%) | 6 (12.2) | 12 (33.3) | |||
| Comorbidity | 50 | 38 | |||
| Hypertension, n (%) | 31 (62.0) | 22 (57.9) | 0.826 | ||
| Heart disease, n (%) | 6 (12.0) | 3 (7.9) | 0.726 | ||
| Diabetes mellitus, n (%) | 7 (14.0) | 7 (18.4) | 0.770 | ||
| End stage of renal disease, n (%) | 1 (2.0) | 2 (5.3) | 0.576 | ||
| Medication | 50 | 38 | |||
| RASI, n (%) | 20 (40.0) | 14 (36.8) | 0.827 | ||
| Calcium channel blocker, n (%) | 29 (58.0) | 19 (50.0) | 0.520 | ||
| α-blocker, n (%) | 4 (8.0) | 2 (5.3) | 0.695 | ||
| β-blocker, n (%) | 4 (8.0) | 4 (10.5) | 0.722 | ||
| Diuretic, n (%) | 4 (8.0) | 2 (5.3) | 0.695 | ||
| Perioperative data | |||||
| Puncture intervertebral | 50 | 38 | 0.267 | ||
| < L3/4, n (%) | 1 (2.0) | 4 (10.5) | |||
| L3/4, n (%) | 38 (76.0) | 27 (71.1) | |||
| > L3/4, n (%) | 11 (22.0) | 7 (18.4) | |||
| Baricity of 0.5% bupivacaine | 50 | 38 | 0.219 | ||
| Isobaric, n (%) | 9 (18.0) | 3 (7.9) | |||
| Hyperbaric, n (%) | 41 (82.0) | 35 (92.1) | |||
| Dose of bupivacaine (mL), median (IQR) | 50 | 2.0 (1.8–2.2) | 38 | 2.0 (1.8–2.1) | 0.308 |
| ≥ 2.5 ml, n (%) | 6 (12.0) | 2 (5.3) | 0.475 | ||
| 2.5–2.0 ml, n (%) | 31 (62.0) | 25 (65.8) | |||
| < 2.0 ml, n (%) | 13 (26.0) | 11 (28.9) | |||
| Preoperative anesthesia level > 10th thoracic vertebra, n (%) | 49 | 25 (51.0) | 35 | 21 (60.0) | 0.506 |
| Postoperative anesthesia level > 10th thoracic vertebra, n (%) | 43 | 24 (55.8) | 33 | 23 (69.7) | 0.243 |
| Operation time (min), median (IQR) | 50 | 52.0 (34.8–66.8) | 38 | 45.5 (28.8–68.0) | 0.433 |
| Anesthesia time (min), median (IQR) | 50 | 72.0 (54.0–87.5) | 38 | 76.5 (49.3–92.0) | 0.866 |
| Infusion volume | 50 | 38 | |||
| Preoperative infusion volume (mL), median (IQR) | 0.0 (0.0–0.0) | 0.0 (0.0–162.5) | 0.187 | ||
| Intraoperative infusion volume (mL), median (IQR) | 725.0 (517.5–912.5) | 875.0 (687.5–1212.5) | 0.020 | ||
| Postoperative infusion volume up to 6 h (mL), median (IQR) | 480.0 (480.0–480.0) | 480.0 (480.0–492.5) | 0.585 | ||
| Intraoperative vasopressor | 50 | 38 | |||
| Ephedrine (mg), median (IQR) | 5.0 (0.0–12.0) | 8.0 (0.0–16.0) | 0.325 | ||
| Phenylephrine (mg), median (IQR) | 0.0 (0.0–0.0) | 0.2 (0.0–0.6) | 0.002 | ||
| Dopamine, n (%) | 0 | 2 (5.3) | 0.184 | ||
| Dobutamine, n (%) | 0 | 2 (5.3) | 0.184 | ||
| Norepinephrine, n (%) | 1 (2.0) | 4 (10.5) | 0.161 | ||
| Sedative drug | 50 | 38 | |||
| Propofol, n (%) | 46 (92.0) | 36 (94.7) | 0.695 | ||
| Excluding propofol, n (%) | 14 (28.0) | 7 (18.4) | 0.325 | ||
| Analgesic drug | 50 | 38 | |||
| Fentanyl, n (%) | 1 (2.0) | 1 (2.6) | > 0.999 | ||
| Pentazocine, n (%) | 13 (26.0) | 9 (23.7) | > 0 .999 | ||
| Blood pressure | |||||
| mBP before administration of 5-ALA, median (IQR) | 50 | 96.3 (91.1–106.2) | 38 | 92.5 (79.9–95.8) | 0.001 |
| mBP upon entering the operating room, median (IQR) | 50 | 99.3 (91.6–106.5) | 38 | 91.7 (84.9–101.2) | 0.005 |
| Minimum mBP before starting operation, median (IQR) | 50 | 67.0 (60.4–77.7) | 38 | 61.2 (57.3–66.3) | 0.001 |
| Minimum mBP after starting operation, median (IQR) | 50 | 62.0 (57.6–66.8) | 38 | 55.3 (52.0–57.7) | < 0.001 |
| mBP upon leaving the operating room, median (IQR) | 50 | 75.0 (70.3–84.7) | 38 | 69.3 (63.5–74.7) | < 0.001 |
| mBP 1 h after surgery, median (IQR) | 50 | 81.2 (76.0–87.8) | 38 | 66.5 (62.6–69.8) | < 0.001 |
| mBP 2 h after surgery, median (IQR) | 50 | 85.6 (78.5–91.3) | 38 | 73.0 (67.9–81.3) | < 0.001 |
| mBP 3 h after surgery, median (IQR) | 50 | 89.3 (83.3–98.0) | 38 | 72.5 (66.4–83.1) | < 0.001 |
| mBP 6 h after surgery, median (IQR) | 50 | 97.0 (87.6–104.4) | 37 | 84.0 (73.0–94.2) | < 0.001 |
| Use of postoperative vasopressors, n (%) | 50 | 0 | 38 | 12 (31.6) | < 0.001 |
| Postoperative complications, n (%) | 50 | 3 (6.0) | 38 | 6 (15.8) | 0.166 |
| Classification | Nausea and vomiting, 6 cases | Nausea and vomiting, 3 cases; delirium, 1 case; headache, 2 cases | |||
| Factor | Cases ( | Univariate analysis | ||
| OR | 95% CI |
| ||
| Patient characteristics | ||||
| Age | 105 | 1.012 | 0.961–1.066 | 0.647 |
| Sex | 105 | |||
| Male | 1.000 | ref | ||
| Female | 0.369 | 0.103–1.314 | 0.122 | |
| Height | 105 | 1.011 | 0.965–1.059 | 0.651 |
| Weight | 105 | 1.043 | 1.002–1.085 | 0.038 |
| Body mass index | 105 | 1.196 | 1.035–1.384 | 0.016 |
| ASA-PS | 105 | |||
| 1 | 1.000 | ref | ||
| 2 | 0.769 | 0.090–6.555 | 0.809 | |
| 3 | 0.799 | 0.057–11.201 | 0.866 | |
| Hemoglobin | 105 | 0.857 | 0.663–1.107 | 0.235 |
| Hematocrit | 105 | 0.946 | 0.859–1.042 | 0.254 |
| eGFR | 102 | 0.968 | 0.941–0.995 | 0.020 |
| ≥ 60 mL/min/1.73 m2 | 1.000 | ref | ||
| 45–60 mL/min/1.73 m2 | 3.072 | 1.104–8.548 | 0.032 | |
| < 45 mL/min/1.73 m2 | 4.609 | 1.410–15.067 | 0.012 | |
| Comorbidity | 105 | |||
| Hypertension | 0.982 | 0.416–2.316 | 0.966 | |
| Heart disease | 0.657 | 0.141–3.063 | 0.590 | |
| Diabetes mellitus | 2.178 | 0.727–6.520 | 0.162 | |
| End stage of renal disease | 2.842 | 0.214–37.718 | 0.425 | |
| Medication | 105 | |||
| RASI | 1.137 | 0.480–2.694 | 0.768 | |
| Calcium channel blocker | 0.653 | 0.280–1.521 | 0.320 | |
| α-blocker | 1.240 | 0.318–4.840 | 0.755 | |
| β-blocker | 1.409 | 0.300–6.605 | 0.661 | |
| Diuretic | 1.409 | 0.297–6.678 | 0.663 | |
| Perioperative data | ||||
| Puncture intervertebral | 104 | |||
| < L3/4 | 3.113 | 0.394–24.618 | 0.279 | |
| L3/4 | 1.070 | 0.366–3.130 | 0.901 | |
| > L3/4 | 1.000 | ref | ||
| Baricity of 0.5% bupivacaine | 104 | |||
| Isobaric | 1.000 | ref | ||
| Hyperbaric | 2.383 | 0.667–8.511 | 0.179 | |
| Dose of bupivacaine | 104 | 0.815 | 0.210–3.159 | 0.765 |
| ≥ 2.5 mL | 0.660 | 0.123–3.539 | 0.624 | |
| 2.5–2.0 mL | 0.881 | 0.338–2.294 | 0.793 | |
| < 2.0 mL | 1.000 | ref | ||
| Preoperative anesthesia level > 10th thoracic vertebra | 99 | 1.550 | 0.647–3.716 | 0.322 |
| Postoperative anesthesia level > 10th thoracic vertebra | 92 | 1.615 | 0.625–4.169 | 0.318 |
| Operation time | 105 | 0.991 | 0.974–1.008 | 0.281 |
| Anesthesia time | 105 | 0.994 | 0.978–1.010 | 0.439 |
| Preoperative infusion volume | 105 | 1.001 | 0.998–1.004 | 0.594 |
| Intraoperative infusion volume | 105 | 1.001 | 1.000–1.002 | 0.034 |
| Intraoperative vasopressor | 105 | |||
| Ephedrine | 1.019 | 0.971–1.070 | 0.441 | |
| Phenylephrine | 1.855 | 0.793–4.338 | 0.152 | |
| Dopamine | 3.140 | 0.233–42.284 | 0.385 | |
| Dobutamine | n.c.* | |||
| Norepinephrine | 7.926 | 0.805–78.009 | 0.076 | |
| Sedative drug during surgery | 105 | |||
| Propofol | 0.853 | 0.194–3.758 | 0.832 | |
| Excluding propofol | 0.722 | 0.269–1.938 | 0.515 | |
| Analgesic drug during surgery | 105 | |||
| Fentanyl | 1.379 | 0.069–27.547 | 0.832 | |
| Pentazocine | 0.865 | 0.337–2.217 | 0.760 | |
| Blood pressure | 105 | |||
| mBP before administration of 5-ALA | 0.942 | 0.903–0.983 | 0.006 | |
| mBP before administration of 5-ALA < 95 mmHg | 2.710 | 1.136–6.468 | 0.025 | |
| mBP upon entering the operating room | 0.943 | 0.908–0.978 | 0.002 | |
| mBP upon entering the operating room < 95 mmHg | 3.690 | 1.535–8.870 | 0.004 | |
| Factor | Multivariate analysis | ||
| OR | 95% CI |
| |
| Body mass index | 1.290 | 1.079–1.542 | 0.006 |
| eGFR | |||
| ≥ 60 mL/min/1.73 m2 | 1.000 | ref | |
| 45–60 mL/min/1.73 m2 | 3.757 | 1.153–12.249 | 0.029 |
| < 45 mL/min/1.73 m2 | 7.295 | 1.804–29.501 | 0.007 |
| Blood pressure | |||
| mBP before administration of 5-ALA < 95 mmHg | 2.751 | 0.931–8.129 | 0.067 |
| mBP upon entering the operating room < 95 mmHg | 3.134 | 1.061–9.262 | 0.039 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBladder and Urothelial Cancer Treatments · Cardiac, Anesthesia and Surgical Outcomes · Neurosurgical Procedures and Complications
Introduction
Transurethral resection of bladder tumors (TUR-Bt) using 5-aminolevulinic acid (5-ALA) is commonly performed to visualize tumors. However, perioperative hypotension occurs frequently during surgery when 5-ALA is administered [1-9]. Although several risk factors for intraoperative hypotension have been reported, those associated with postoperative hypotension have not yet been identified. These factors are also of clinical interest owing to their potential impact on patient outcomes. Postoperative hypotension is associated with myocardial infarction, myocardial injury after noncardiac surgery, and acute kidney injury, and may lead to death [10-12].
Consequently, in the present study, we retrospectively examined the dependent risk factors for postoperative hypotension in patients who underwent TUR-Bt with administration of oral 5-ALA under general or spinal anesthesia. With regard to the anesthetic technique, general anesthesia is an independent risk factor for intraoperative hypotension, compared with spinal anesthesia [13-18]; however, perioperative hypotension owing to oral 5-ALA has also been observed in patients receiving spinal anesthesia [19,20]. Furthermore, there are other factors unique to spinal anesthesia, such as the drug and method used. Therefore, we also examined the same risk factors for postoperative hypotension in a subset of patients who underwent spinal anesthesia.
Materials and methods
Study population
This study was approved by the Ethics Committee of the University of Miyazaki Hospital (approval number O-1211). The need for informed consent from patients was waived owing to the retrospective nature of the study. The enrolled participants were patients who underwent TUR-Bt with 5-ALA for photodynamic diagnosis, between July 2020 and December 2023 at the University of Miyazaki Hospital. The exclusion criteria for patients were absence of records of vital signs before 5-ALA administration, additional surgery other than TUR-Bt, reoperation owing to postoperative bleeding, surgery lasting for more than 120 min, or absence of postoperative blood pressure records. First, independent risk factors for postoperative hypotension were analyzed in all patients undergoing TUR-Bt with 5-ALA under general or spinal anesthesia. Subsequently, risk factors were analyzed in the same manner in a subset of patients who received spinal anesthesia.
All patients received oral 5-ALA (20 mg/kg; Alaglio®, SBI Pharmaceuticals Co., Ltd., Tokyo, Japan) 2−4 hours before surgery. After the patient was admitted to the operating room, standard monitoring was performed, including electrocardiography, noninvasive blood pressure measurements, and pulse oximetry. Anesthesia details and hypotension treatments were determined by an individual anesthesiologist based on the condition of the patient.
Data collection
The following data were collected from electronic medical and anesthesia records: age; sex; height; weight; body mass index (BMI); American Society of Anesthesiologists physical status classification (ASA-PS); preoperative hemoglobin concentration and hematocrit; preoperative estimated glomerular filtration rate (eGFR; mL/min/1.73 m^2^); comorbidities (hypertension, heart disease, diabetes, end stage of renal disease); use of renin-angiotensin system inhibitors (RASI), calcium channel blockers, α- and β-blockers, diuretics; anesthetic technique (general anesthesia or spinal anesthesia); operation and anesthesia time; infusion volume (preoperative infusion volume, intraoperative infusion volume, postoperative infusion volume up to 6 h after surgery); use of ephedrine, phenylephrine, dopamine, dobutamine, and noradrenaline; mean blood pressure (mBP) before 5-ALA administration and on entry into the operating room, mBP from induction of anesthesia to the beginning of surgery, mBP after the beginning of surgery, mBP on leaving the operating room, and mBP at 1, 2, 3, and 6 h after surgery; postoperative use of vasopressors; postoperative complications; and in cases of spinal anesthesia, the lumbar intervertebral space used, specific baricity, and volume of the drug solution used, and preoperative and postoperative anesthesia levels. Cardiac disease was defined as atrial fibrillation, pacemaker implantation, moderate or severe valvular disease, prior percutaneous coronary intervention or coronary artery bypass surgery, or prior heart failure.
Postoperative mBP was obtained from electronic medical records 1, 2, 3, and 6 h after intervention. Based on a previous report that investigated the association between postoperative hypotension and myocardial damage [12], postoperative hypotension was defined as an mBP of < 70 mmHg, noted at least once in the electronic medical records. Patients who developed postoperative hypotension or used postoperative vasopressors were assigned to the hypotension group. All patients were divided into two groups: the non-hypotension and hypotension groups.
Statistical analysis
Data are expressed as the median (interquartile range). mBP trends are expressed as the mean ± standard deviation (SD). For between-group comparisons, Fisher’s exact probability test was used for categorical variables, and the Mann-Whitney U test was used for continuous variables. Univariate and multivariate analyses were performed using mixed models; that is, patients who experienced two or more surgeries during the study period were also included. Multivariate analysis using the forced entry method was performed for factors that were significantly different on univariate analysis. Intraoperative blood pressure was not included in the univariate and multivariate analyses because the study aimed to predict the occurrence of postoperative hypotension from information other than intraoperative blood pressure. Intraoperative fluid volume and intraoperative vasopressors were not included in the multivariate analysis because they were expected to reflect intraoperative hypotension. Statistical significance was set at P < 0.05. Statistical analyses were performed using SPSS Statistics for Windows version 29.0 (IBM Corp., Armonk, NY, USA).
Results
In this study, a mixed model was used for univariate and multivariate analysis. Patients who underwent two or more TUR-Bt during the study period were also included, so the number of patients and cases differed. A total of 126 patients who underwent TUR-Bt with 5-ALA treatment were enrolled in the initial study: 27 patients received general anesthesia and 99 patients received spinal anesthesia. Among the patients who underwent general anesthesia, four were excluded and 23 were included in the study (28 cases). Among the 99 patients who underwent spinal anesthesia, 11 were excluded and 88 included (105 cases). Thus, a total of 111 patients were included (133 cases in total). Patients with a postoperative mBP of < 70 mmHg and those who used postoperative vasopressors were defined as the hypotension group. Thus, 65 and 46 patients comprised the non-hypotension and hypotension groups, respectively. Table 1 shows the patient characteristics and perioperative information of the two groups. In the between-group comparisons, significant differences were found in eGFR, intraoperative infusion volume, phenylephrine dose, mBP before 5-ALA administration, mBP upon entry into the operating room (before anesthesia induction), minimum mBP before surgery (after anesthesia induction), minimum mBP after starting surgery, mBP upon leaving the operating room, mBP at different time points, 1, 2, 3, and 6 h, after surgery, and use of postoperative vasopressors. The perioperative mBP trends in each group are shown in Figure 1.
Trends of mean blood pressure in the non-hypotension and hypotension groups of all patients who underwent general or spinal anesthesia. The non-hypotension group: n = 65, and hypotension group: n = 46. In this study using mixed models, patients who underwent two or more TUR-Bt during the study period were also included. For duplicate cases, data from the first case was used. Data are expressed as mean ± standard deviation. mBP, mean blood pressure. Timepoints: a, before administration of 5-aminolevulinic acid; b, upon entering the operating room; c, minimum value before surgery; d, minimum value after starting surgery; e, upon leaving the operating room; f, 1 h after surgery; g, 2 h after surgery; h, 3 h after surgery; and i, 6 h after surgery.
The results of the univariate and multivariate analyses are shown in Tables 2-3. Univariate analysis revealed significant differences in eGFR, intraoperative fluid volume, mBP before 5-ALA administration, and mBP upon entry into the operating room. Multivariate analysis was performed on these factors except for intraoperative fluid volume, and results revealed that eGFR ≤ 45-60 mL/min/1.73 m^2^, eGFR < 45 mL/min/1.73 m^2^, and mBP < 95 mmHg upon entry into the operating room were significant risk factors for postoperative hypotension.
Next, we examined the risk factors for postoperative hypotension in patients undergoing spinal anesthesia (50 patients in the non-hypotension group and 38 patients in the hypotension group). Table 4 shows the patient background characteristics and perioperative information of the two groups. Comparisons between the groups revealed significant differences in weight; eGFR; intraoperative infusion volume; phenylephrine dose; mBP before 5-ALA administration and upon entry into the operating room; minimum mBP before and during surgery; mBP on leaving the operating room and at different time points, 1, 2, 3, and 6 h, after surgery; and use of postoperative vasopressors. The perioperative mBP trends in each group are shown in Figure 2.
Trends of mean blood pressure in the non-hypotension and hypotension groups of patients who underwent spinal anesthesia.The non-hypotension group: n = 50, and hypotension group: n = 38. In this study using mixed models, patients who underwent two or more TUR-Bt during the study period were also included. For duplicate cases, data from the first case was used. Data are expressed as mean ± standard deviation. mBP, mean blood pressure. Timepoints: a, before administration of 5-aminolevulinic acid; b, upon entering the operation room; c, minimum value before surgery; d, minimum value after starting surgery; e, upon leaving the operation room; f, 1 h after surgery; g, 2 h after surgery; h, 3 h after surgery; and i, 6 h after surgery.
The results of the univariate and multivariate analyses of patients undergoing spinal anesthesia are shown in Tables 5-6. Univariate analysis revealed significant differences in body weight, BMI, eGFR, intraoperative fluid volume, mBP before 5-ALA administration, and mBP upon entry into the operating room. Multivariate analysis was performed on these factors except for intraoperative fluid volume and revealed significant differences in BMI, eGFR ≤ 45-60 mL/min/1.73 m^2^, eGFR < 45 mL/min/1.73 m^2^, and mBP < 95 mmHg upon entry into the operating room.
Discussion
Postoperative hypotension occurred in approximately 40% of patients with TUR-Bt who received oral 5-ALA. Although the patient background predicted an association between intraoperative and postoperative hypotension, intraoperative blood pressure was not included in the univariate and multivariate analyses because, in the present study, we aimed to predict the occurrence of postoperative hypotension from information other than intraoperative blood pressure; particularly, preoperative information and method of anesthesia. Multivariate analysis showed that eGFR ≤ 60 mL/min/1.73 m^2^ and mBP < 95 mmHg upon entry into the operating room were independent risk factors for postoperative hypotension, whereas method of anesthesia was not. These findings imply that poor renal function resulted in increased postoperative hypotension. In the current study, postoperative hypotension was defined in absolute rather than relative value, suggesting that higher blood pressure before anesthesia was less likely to result in postoperative hypotension.
mBP values before anesthesia in the hypotension group were significantly lower than those in the non-hypotension group of patients, irrespective of whether they received general or spinal anesthesia. Additionally, severe hypotension before anesthesia was also observed in a few patients, possibly owing to 5-ALA administration. The intraoperative infusion volume and phenylephrine dose in the hypotension group were significantly higher than those in the non-hypotension group, likely owing to intraoperative hypotension, as evidenced by a median minimum mBP of < 65 mmHg after anesthesia induction. In patients who underwent spinal anesthesia, multivariate analysis showed that BMI, eGFR ≤ 60 mL/min/1.73 m^2^, and mBP < 95 mmHg upon entering the operating room were independent risk factors for postoperative hypotension. However, none of the spinal anesthesia-related factors, such as specific baricity and dose of bupivacaine, lumbar intervertebral space used, or anesthesia level before and after surgery, were found to be risk factors. The risk factors in patients undergoing spinal anesthesia were similar to those of patients who underwent spinal or general anesthesia, and the choice of technique and drug for spinal anesthesia did not appear to be specifically associated with the occurrence of postoperative hypotension.
Several reports have described the risk factors for intraoperative hypotension associated with oral 5-ALA, but none have investigated the incidence of postoperative hypotension. The risk factors for intraoperative hypotension identified in previous reports include general anesthesia, age, female sex, BMI, eGFR, coexisting hypertension, oral calcium channel blocker or RASI treatment, preoperative general condition, and systolic blood pressure < 100 mmHg before anesthesia induction [1,4,13-18,21]. In particular, age > 70-80 years [1,4,12,13,20] and eGFR < 45-60 mL/min/1.73 m^2^ [1,21] have been frequently reported as risk factors. Importantly, BMI, eGFR, and mBP upon entry into the operating room were also associated with postoperative hypotension in the present study. Although higher hematocrit has been associated with greater intraoperative hypotension [22], this was not the case with the occurrence of postoperative hypotension in the present study, wherein the anesthesia method had no effect on the occurrence of postoperative hypotension. However, the effect of 5-ALA on lowering blood pressure continues for more than 9 h [5]; as sympathetic inhibition during spinal anesthesia is expected to continue after surgery, postoperative hypotension should be considered, especially when spinal anesthesia is selected as the method of anesthesia [20]. Although administering spinal anesthesia in patients with obesity, impaired renal function, or mBP < 95 mmHg upon entering the operating room, and especially, a severe decrease in blood pressure after 5-ALA administration, clinicians should be prepared for hypotension to occur postoperatively. Hypotension induced by 5-ALA may involve the activity of its metabolite, protoporphyrin IX, which induces blood vessel dilation [23,24]. Nonetheless, the mechanisms underlying 5-ALA-induced hypotension remain to be further clarified. Therefore, measures to prevent hypotension should be taken with reference to risk factors for perioperative hypotension.
Miyakawa et al. reported risk factors for severe hypotension in TUR-Bt with 5-ALA [21]. They defined severe hypotension cases as patients who required continuous norepinephrine administration. Severe hypotension cases occurred in eight of 128 patients, four of whom required a vasopressor due to prolonged postoperative hypotension. Risk factors for severe hypotension were concluded to be age ≥ 80 years, BMI ≥ 25 kg/m^2^ and eGFR < 45 mL/min/1.73 m^2^, which were the same as in our results, except for age. Therefore, the dose of 5-ALA should probably be adjusted in patients with a combination of these factors.
This study has some limitations. This was a single-center, retrospective study; a multicenter, prospective study is required to obtain high-quality evidence. A consensus on the definition of postoperative hypotension is lacking, which may limit the generalizability of our findings. Additionally, we did not assess the duration of hypotension, which could have provided further insights into its clinical significance. As this study was based on the assumption that hypotension was induced by oral 5-ALA, we did not include oral 5-ALA as a factor for postoperative hypotension in the statistical analysis. Therefore, patients who were not administered oral 5-ALA were not included. As few patients underwent general anesthesia, it can not be stated with certainty that the method of anesthesia has no influence on the occurrence of postoperative hypotension. Although postoperative hypotension should be monitored because it is associated with noncardiac postoperative myocardial damage and death [11,12], this study included data only up to 6 h postoperatively. In future, it would be worth performing a long-term postoperative follow-up and evaluating the outcomes in the hypotension group.
Conclusions
Dependent risk factors for postoperative hypotension in patients undergoing TUR-Bt with 5-ALA under general or spinal anesthesia included eGFR and mBP upon entry to the operating room. In spinal anesthesia cases, dependent risk factors were BMI, eGFR, and mBP upon entry to the operating room, but it did not include any of the spinal anesthesia-related factors.
Our findings demonstrated that, regardless of the anesthesia method, impaired renal function increased postoperative hypotension, and higher blood pressure before anesthesia was less likely to result in postoperative hypotension. In cases with a combination of these risk factors, it is prudent to adjust the dose of 5-ALA or avoid its use in the prevention of postoperative hypotension.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Comprehensive analysis of perioperative hypotension in photodynamic diagnosis-assisted transurethral resection of bladder tumor with 5-aminolevulinic acid Int J Urol Nohara T Takimoto A Shinzawa R 8918983120243868713810.1111/iju.15477 · doi ↗ · pubmed ↗
- 2Severe hypotension and postoperative cardiac arrest caused by 5-aminolevulinic acid: a case report J Med Case Rep Miyazaki T Taguchi S Obata N Mizobuchi S 2641820243881194110.1186/s 13256-024-04589-x PMC 11137901 · doi ↗ · pubmed ↗
- 3Effect of arginine vasopressin on intraoperative hypotension caused by oral administration of 5-aminolevulinic acid Case Rep Anesthesiol Owada G Nishizawa H Matoyama Y 1745373202320233719296010.1155/2023/1745373 PMC 10182879 · doi ↗ · pubmed ↗
- 4Association of 5-aminolevulinic acid with intraoperative hypotension in malignant glioma surgery Photodiagnosis Photodyn Ther Morisawa S Jobu K Ishida T 1026573720223484837810.1016/j.pdpdt.2021.102657 · doi ↗ · pubmed ↗
- 5Differences in 5-aminolevulinic acid-induced hemodynamic changes between patients undergoing neurosurgery and urological surgery JMA J Shiratori T Hotta K Satoh M Sato A Kamigaito T Kiuchi C Tanaka R 374386420213479629210.31662/jmaj.2021-0092 PMC 8580708 · doi ↗ · pubmed ↗
- 6Oral 5-aminolevulinic acid administration prior to transurethral resection of bladder tumor causes intraoperative hypotension: Propensity score analysis Photodiagnosis Photodyn Ther Nakatani S Ida M Wang X Naito Y Kawaguchi M 1023423420213400045010.1016/j.pdpdt.2021.102342 · doi ↗ · pubmed ↗
- 7Severe and prolonged hypotension after oral 5-aminolevulinic acid administration in a patient with end-stage renal disease undergoing transurethral resection of a bladder tumor: A case report A A Pract Kida T Kobashi T Usuda Y Kobayashi K Sumitomo M 12141420203170300710.1213/XAA.0000000000001128 · doi ↗ · pubmed ↗
- 8Preanesthetic severe postural hypotension following 5-aminolevulinic acid pretreatment in patients for photodynamic diagnosis-assisted urological surgery JA Clin Rep Shiratori T Hotta K Satoh M Kiuchi C Ogawa N Kamigaito T 74520193202593710.1186/s 40981-019-0295-1PMC 6967019 · doi ↗ · pubmed ↗