First reported Tannerella forsythia infection in a patient with extensive bronchiectasis: a case report
Congli Fu, Yilan Sun, Chun Chen

TL;DR
A patient with bronchiectasis was infected by Tannerella forsythia, a bacterium typically linked to oral diseases, and successfully treated with antibiotics.
Contribution
First reported case of Tannerella forsythia infection in a patient with extensive bronchiectasis and an effective treatment approach.
Findings
Tannerella forsythia was detected in bronchoalveolar lavage fluid using metagenomic next-generation sequencing.
Treatment with Piperacillin-tazobactam and ornidazole led to a favorable clinical outcome.
The infection was associated with symptoms like fever, cough, and shortness of breath in a bronchiectasis patient.
Abstract
Tannerella forsythia infection was common in oral diseases but less reported in lung diseases. This report presents a patient with bronchiectasis who was infected by Tannerella forsythia and subsequently hospitalized with symptoms including fever, progressive cough, sputum production, and shortness of breath. A chest computed tomography (CT) scan revealed multiple bilateral pulmonary bronchiectasis with signs of infection. Metagenomic next-generation sequencing (mNGS) of the bronchoalveolar lavage fluid primarily detected Tannerella forsythia. Treatment with Piperacillin-tazobactam and ornidazole resulted in a favorable outcome. This case first reported a patient with extensive bronchiectasis infected by Tannerella forsythia and provided an effective treatment.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
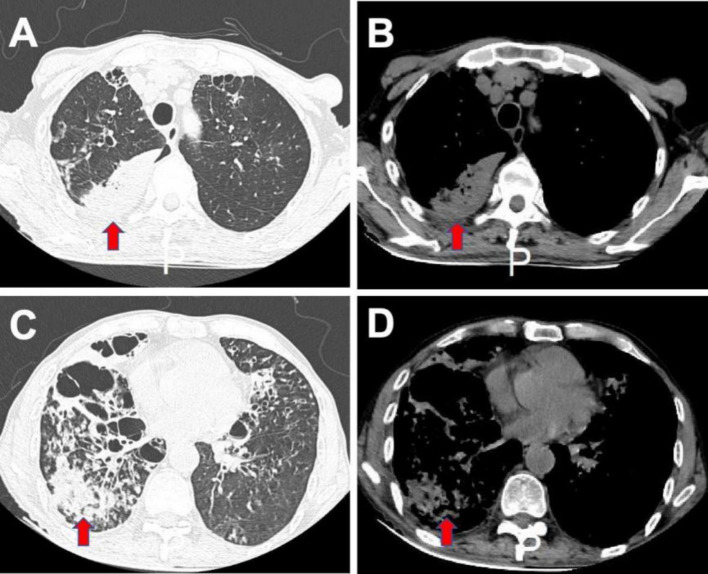 Figure 1
Figure 1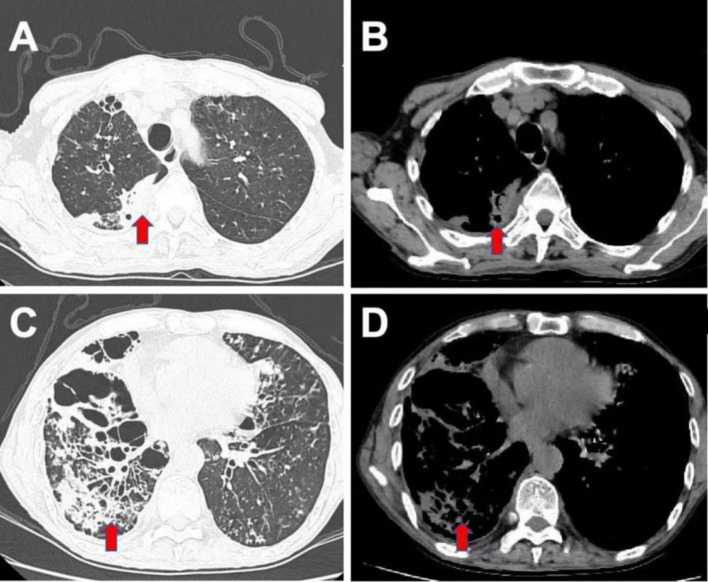 Figure 2
Figure 2| Name of pathogen | Sequences |
|---|---|
|
| 1965 |
|
| 618 |
|
| 208 |
|
| 38 |
|
| 30 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTracheal and airway disorders · Cystic Fibrosis Research Advances · Enterobacteriaceae and Cronobacter Research
Background
Bronchiectasis, a common pulmonary disease often characterized by inflammation, frequently presents with bacterial infections. In recent years, numerous studies have explored the bacteriome in bronchiectasis, identifying genera such as Pseudomonas, Haemophilus, Streptococcus, Veillonella, Prevotella, Stenotrophomonas, and Neisseria (1). Elderly patients with bronchiectasis often suffer from malnutrition and may experience weakened swallowing function. If these patients develop dental caries, oral pathogens can easily invade the lungs. However, the role of oral pathogens in bronchiectasis has received limited attention. Tannerella forsythia, a gram-negative bacterium, typically does not thrive aerobically. Instead, it is commonly associated with odontogenic diseases such as chronic periodontitis, gingivitis, and aggressive periodontitis. This article represents the first documented case of Tannerella forsythia infection in a patient with bronchiectasis.
Case presentation
A 70-year-old male was admitted to the hospital presenting with severe cough, chest pressure, and a low-grade fever. He had been experiencing symptoms of cough, sputum production, and shortness of breath following physical activity for over 40 years. About a week prior to admission, he noticed a worsening of these symptoms accompanied by fever, prompting him to seek treatment at a local community hospital. Despite receiving antibiotics such as cefuroxime axetil tablets and cough medication, his symptoms persisted. The patient denied any episodes of hemoptysis or chest pain. Subsequently, he was referred to our hospital for further evaluation. The patient had worked as a quarry owner for nearly four decades and reported no history of smoking or alcohol consumption.
During the physical examination, the patient exhibited a fever of 38.2°C, and moist rales were auscultated over both lungs. Additionally, upon further examination, two carious teeth were discovered. Blood tests revealed elevated neutrophil levels (8.49 × 10^9/L), along with increased levels of C-reactive protein (CRP) at 215.7 mg/L and elevated procalcitonin (PCT) levels at 0.77 ng/mL. A chest CT scan illustrated multiple bilateral pulmonary bronchiectases with infection (Figure 1).
Chest CT scan before treatment. The CT scan showed bilateral bronchiectasis, with predominant involvement of the right lung, bronchial wall thickening, and multiple patchy opacities in both lungs. (A,C) Lung windows; (B,D) Mediastinal windows.
The patient was started on intravenous antibiotic therapy with piperacillin-tazobactam (4.5 g every 8 h) according to the guidelines of the British Thoracic Society (BTS) and the European Respiratory Society (ERS) (2, 3). However, after a week, the patient’s fever persisted, and serum CRP levels remained elevated at 111.8 mg/L. Subsequently, bronchoalveolar lavage was conducted to identify the causative pathogens. Metagenomic next-generation sequencing (mNGS) of the bronchoalveolar lavage fluid (BALF) identified multiple organisms including Tannerella forsythia, Parvimonas micra, Fusobacterium nucleatum, Proteus mirabilis, and Streptococcus intermedius (Table 1). No pathogens were isolated through conventional culture methods from the BALF. A dental examination was performed, revealing two dental caries in the patient. Although the patient denied a history of aspiration, we speculated that latent aspiration may be present. Consequently, treatment was later adjusted to combine piperacillin-tazobactam with ornidazole (0.5 g every 12 h, instead of metronidazole) for a 10-day course, following the guidelines of the European Federation of Periodontology (EFP) (4). Subsequent review of the chest CT scan (Figure 2) revealed partial resolution of the infection. The patient experienced alleviation of symptoms, and serum inflammatory markers showed overall normalization. Consequently, he was discharged from the hospital and prescribed oral antibiotics (amoxicillin and clavulanate potassium 312.5 mg tid) for an additional week.
Chest CT scan after 10 days of anti-infection treatment. The CT scan showed similar findings of bilateral bronchiectasis and bronchial wall thickening, with a noticeable reduction in patchy consolidations. (A,C) Lung windows; (B,D) Mediastinal windows.
Discussion
Bronchiectasis is a chronic pulmonary disease characterized by the dilatation of bronchi and persistent bacterial infection of the affected bronchial tubes (5). Individuals with bronchiectasis experience a higher frequency of annual respiratory tract infections and typically have a lower quality of life compared to healthy individuals (6). The most common bacteria associated with chronic bronchial infections include Pseudomonas aeruginosa, Haemophilus influenzae, and Staphylococcus aureus (7). In this report, we identified Tannerella forsythia infection in the BALF obtained from the patient’s diseased airways.
Tannerella forsythia is a kind of Gram-negative bacterium of Tannella, a common symbiotic bacteria in humans, and a member of the red complex of periodontal disease pathogens. The red complex oral bacteria includes Porphyromonas gingivalis, Treponema denticola and Tannerella forsythia, which always existing together. They are commonly found in oral cavity, associated with periodontitis, gingivitis and various cancers (8). They can inhibit monocyte chemotaxis by blocking the expression of adhesion molecules in intercelular reactions and block the body’s anti-inflammatory response (9). Tannerella forsythia has several virulence factors including proteases (KLIKK, PrtH), dipeptidyl peptidase IV, miropin, glycosidases (SusB, SiaHI, NanH, and HexA) and the OxyR protein (10). These virulence factors protect the bacterium from being killed in host tissue and promote disease progression. Although Tannerella forsythia infection is commonly associated with oral diseases, there is limited available literature on its involvement in lung infections. Recently, there have been two reports documenting Tannerella forsythia infection in cases of massive empyema and lung abscess (11, 12). Elderly patients with bronchiectasis are often weak and malnourished, frequently exhibiting impaired swallowing function and a potential for aspiration. Oral pathogens can reach the lower respiratory tract through aspiration, leading to infections. In some cases, patients with severe periodontitis may have oral pathogens enter the bloodstream, which can then infect the lungs. As in the oral cavity, Tannerella forsythia can damage the airway mucosa, facilitate the invasion of other pathogens, inhibit monocyte chemotaxis, and suppress the body’s anti-inflammatory response. In the present case, the patient had extensive bronchiectasis for many years and was found to be infected with Tannerella forsythia in the diseased airways.
Tannerella forsythia infection is frequently misdiagnosed due to the challenges associated with its detection using conventional culture techniques. Unlike many other bacteria, Tannerella forsythia lacks the biosynthetic pathways necessary for producing the sugar N-acetylmuramic acid (MurNAc). This characteristic may contribute to its low culture detection rate (13). In the present case, conventional culture methods failed to isolate any pathogens from the BALF, whereas mNGS identified Tannerella forsythia, along with other bacteria including Parvimonas micra, Fusobacterium nucleatum, Proteus mirabilis, and Streptococcus intermedius. Accurate microbiological identification is crucial for guiding appropriate clinical treatment. However, conventional methods are often time-consuming and may have a low detection rate. Conversely, mNGS demonstrates higher sensitivity in identifying pathogens and offers advantages in detecting potential pathogens (14). Zhang’s study found that mNGS demonstrated superior performance in detecting anaerobic or facultative anaerobic bacteria in patients with lung abscess compared to conventional culture methods, providing crucial evidence for clinical decision-making (15). The prompt application of mNGS benefits to short the time of diagnosism, enabling guided and accurate medication to reduce the risk of disease progression and reduce risk of death. Nonetheless, mNGS also has drawbacks, such as its high cost and the potential for generating data on multiple microorganisms, which can lead to confusion. Moreover, mNGS does not have a clear advantage in identifying fungi, viruses, and tuberculosis. In this case, we tailored the antibiotic therapy based on the results of mNGS, resulting in a favorable treatment outcome.
The antibiotic therapy to Tannerella forsythia infection is less reported. A study indicated that amoxicillin (AMX 500 mg tid for 14 days) plus metronidazole (MTZ 400 mg tid for 14 days) therapy were effective to reduct the red complex in patients with periodontitis (16, 17). While another report showed a failure of AMX + MTZ therapy to resolve peri-implantitis in 1 year follow-up (18). Metronidazole is highly active against anaerobic bacteria. Systemic metronidazole therapy can suppress red complex significantly. However, metronidazole was taken orally three times per day for 7–14 days, which needs patient compliance. Tinidazole is a second-generation 2-methyl-5-nitroimidazole class antibiotic structurally similar to metronidazole. Tinidazole exerts marked bactericidal activity against anaerobic bacteria and possesses pharmacokinetic properties which enables once-a-day oral systemic drug dosing (19). Ornidazole is a third-generation similar to tinidazole. Liu’s study found that the ecurative effect was no significant difference between ornidazole and mertonidazole, but the side effect of mertonidazole was more severe than that of ornidazole, especially irritaion of gastrointestinal tract (20). In this case, the patient had gastrointestinal discomfort after eating metronidazole tablets before and had no financial burden. Therefore, we chose the ornidazole this time. According to clinical guidelines, metronidazole is recommended as the first-line agent against Red Complex pathogens, while ornidazole may serve as a substitute option in specific cases.
It’s also reported that systemic Sitafloxacin (200 mg/day of STFX for 5 days) and Azithromycin (500 mg/day of AZM for 3 days) monotherapy significantly decreased red complex (21). A recent report showed that meropenem and moxifloxacin treatment were effective in lung abscess infected by Tannerella forsythia (12). Another case reported amoxicillin and amoxicillin-clavulanic acid treatment in a massive empyema pateint (11).
In this case, we chose piperacillin-tazobactam for an initial therapy and added ornidazole for a better therapeutic efficacy. As a kind of anaerobic bacteria, antibiotics to Tannerella forsythia infection are similar, but the specific antibiotic susceptibility of Tannerella forsythia needs more study to confirm.
Conclusion
Tannerella forsythia, traditionally recognized as a member of the red complex of periodontal disease pathogens, has been increasingly implicated in pulmonary infections. In this case, we present the first documented instance of a patient with bronchiectasis being infected by Tannerella forsythia. Diagnosis of Tannerella forsythia infection is often reliant on mNGS, as conventional culture techniques frequently fail to confirm its presence. In our approach to treatment, we opted for a combination therapy of piperacillin-tazobactam and ornidazole, which yielded a favorable curative outcome. While antibiotics effective against anaerobic bacteria may demonstrate efficacy in treating Tannerella forsythia infection, further investigation into the specific antibiotic susceptibility of this pathogen is warranted. This case underscores the importance of considering unconventional pathogens in pulmonary infections and highlights the potential utility of mNGS in their identification and subsequent management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mac Aogáin M Dicker AJ Mertsch P Chotirmall SH. Infection and the microbiome in bronchiectasis. Eur Respir Rev. (2024) 33:240038. doi: 10.1183/16000617.0038-2024, PMID: 38960615 PMC 11220623 · doi ↗ · pubmed ↗
- 2Hill AT Sullivan AL Chalmers J Dde Soyza A Elborn SJ Floto AR. British Thoracic Society guideline for bronchiectasis in adults. Thorax. (2019) 74:1–69. doi: 10.1136/thoraxjnl-2018-212463, PMID: 30545985 · doi ↗ · pubmed ↗
- 3Polverino E Goeminne PC Mc Donnell MJ Aliberti S Marshall SE Loebinger MR. European Respiratory Society guidelines for the management of adult bronchiectasis. Eur Respir J. (2017) 50:1700629. doi: 10.1183/13993003.00629-2017, PMID: 28889110 · doi ↗ · pubmed ↗
- 4Sanz M Herrera D Kebschull M Chapple I Jepsen S Beglundh T. Treatment of stage I–III periodontitis—the EFP S 3 level clinical practice guideline. J Clin Periodontol. (2020) 22:4–60. doi: 10.1111/jcpe.13290 PMC 789134332383274 · doi ↗ · pubmed ↗
- 5King PT. The role of the immune response in the pathogenesis of bronchiectasis. Biomed Res Int. (2018) 2018:1–12. doi: 10.1155/2018/6802637, PMID: 29744361 PMC 5878907 · doi ↗ · pubmed ↗
- 6Sperlich JM Grimbacher B Soetedjo V Workman S Burns SO Lowe DM. Predictive factors for and complications of bronchiectasis in common variable immunodeficiency disorders. J Clin Immunol. (2022) 42:572–81. doi: 10.1007/s 10875-022-01206-8, PMID: 35015197 PMC 9015976 · doi ↗ · pubmed ↗
- 7Solarat B Perea L Faner Rde la Rosa D Martínez-García MÁSibila O. Pathophysiology of chronic bronchial infection in bronchiectasis. Arch Bronconeumol. (2023) 59:101–8. doi: 10.1016/j.arbres.2022.09.004, PMID: 36180278 · doi ↗ · pubmed ↗
- 8Boyanova L Markovska R Yordanov D Gergova R Hadzhiyski P. Anaerobes in specific infectious and noninfectious diseases: new developments. Anaerobe. (2023) 81:102714. doi: 10.1016/j.anaerobe.2023.102714, PMID: 37349047 · doi ↗ · pubmed ↗