Beyond Surgical Limits: A Case Report of Follicular Variant of Papillary Thyroid Carcinoma With Persistent Disease Despite Aggressive Surgical Management
Saleh Khurshied, Mehrun Nisa, Wafa Abdul Malik, Hassan Mansoor, Rayyan Sabih

TL;DR
A young woman with thyroid cancer had three surgeries, but the disease persisted, showing how some cancers resist complete surgical removal.
Contribution
This case highlights the persistence of follicular variant papillary thyroid carcinoma despite aggressive surgical interventions.
Findings
A thyroid remnant was found 10 years after complete thyroidectomy, indicating incomplete removal.
The patient remained asymptomatic and biochemically normal despite persistent disease.
Three surgeries failed to fully remove the resistant carcinoma.
Abstract
The most prevalent type of thyroid gland cancer is called papillary thyroid carcinoma, which typically manifests as a painless thyroid mass in women over 50 years of age. Fine-needle aspiration cytology (FNAC) and ultrasonography (USG) are used to make the diagnosis, and the patient's symptoms and these results determine the course of treatment. We reported a rare case of follicular variant papillary thyroid cancer in a young woman, diagnosed at an unusual age of 22 years, who had three thyroid surgeries intended to completely remove the disease but were unable to do so. The woman was diagnosed with a case of follicular variant of papillary thyroid carcinoma (FVPTC) initially 10 years back, and a hemithyroidectomy was done for diagnostic purposes. Later on, with the diagnosis of FVPTC, a complete thyroidectomy was done at the same time, and the patient recovered uneventfully. For the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
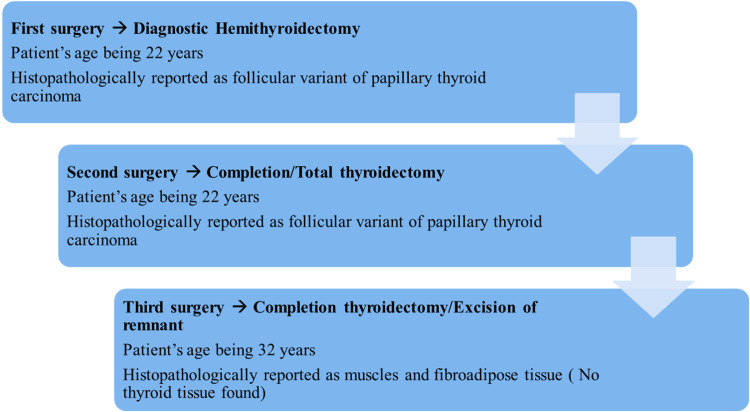 Figure 1
Figure 1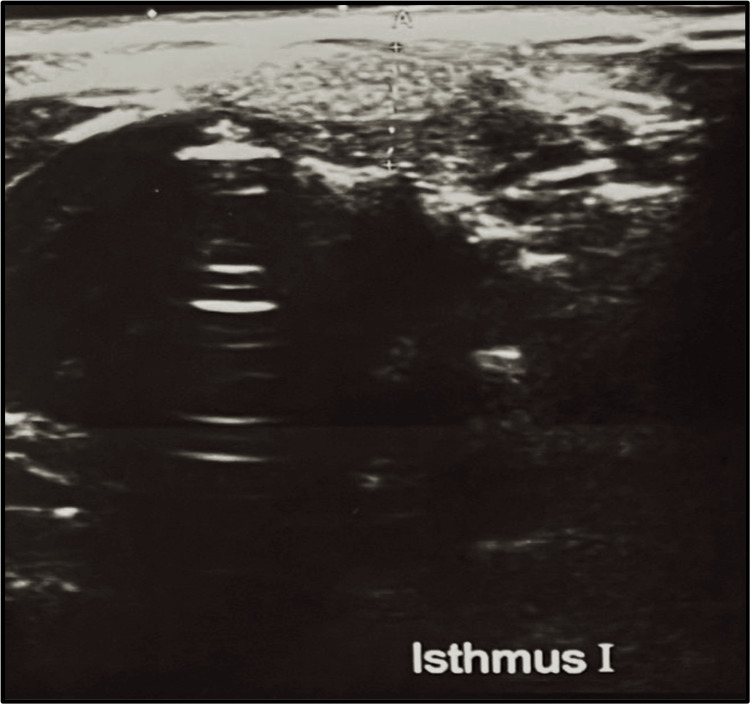 Figure 2
Figure 2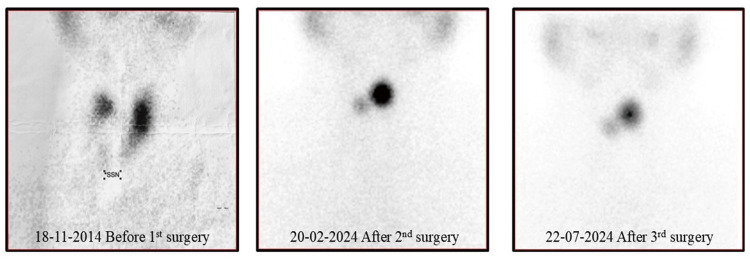 Figure 3
Figure 3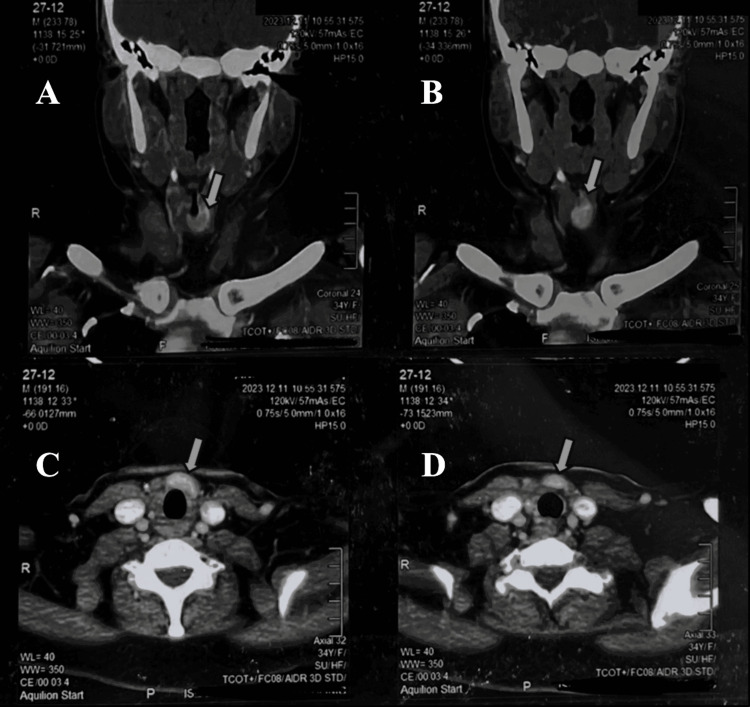 Figure 4
Figure 4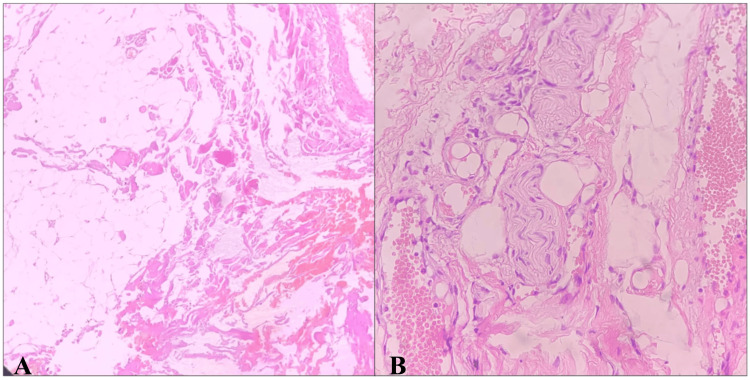 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Cancer Diagnosis and Treatment · Head and Neck Anomalies · Genetic factors in colorectal cancer
Introduction
A rare form of cancer, thyroid gland carcinoma, accounts for around 1% of all newly diagnosed malignant conditions. Women are diagnosed with it three times more frequently than men. Fifty is the median age that it affects [1,2]. The four most prevalent types of these carcinomas are follicular, papillary, medullary, and anaplastic. As "well-differentiated" thyroid tumors, papillary carcinomas account for about 80-85% of all thyroid malignancies [3].
Long-term survival rates for papillary thyroid carcinoma (PTC) are over 95% in numerous studies, indicating that most cases have a favorable prognosis. A less favorable disease is associated with the following risk factors: distant metastases, extra thyroid extension, tumor size greater than 4 cm, and patient age of 45 years or older [4]. Over the past few decades, it has become more common [5].
The recognition of follicular variant of papillary thyroid carcinoma (FVPTC) has grown over the past few years. According to reports, it accounts for between 11.8% and 53.3% of all PTC instances [6]. In the United States, the number of thyroid cancer patients doubled between 1997 and 2007 and reached 62450 in 2015. A total of 90% of thyroid malignancies are well-differentiated thyroid tumors, and PTC accounts for 70% of them [7,8].
Even with its high occurrence, FVPTC's clinical behavior and results are still debatable, which makes developing a standard treatment plan difficult. About one-third of all cases are FVPTC, a fairly frequent variation of PTC. It has distinct clinical behavior and resembles a middle-aged entity with characteristics halfway between classical papillary thyroid carcinoma (CPTC) and follicular thyroid carcinoma (FTC). It's interesting to note that these individuals' long-term results are nonetheless great and comparable to CPTC despite the differences in clinical behavior [7].
The most typical way that FVPTC manifests itself is as a painless lump at the thyroid level. As a result of tracheal compression and/or involvement of the recurrent laryngeal nerve, about 20% of patients may report dysphagia or hoarseness. Thyroid function tests will often be normal in these individuals. The diagnosis is made by fine-needle aspiration cytology (FNAC) and ultrasonography (USG). If it is determined that the tumor is unifocal, smaller than 4 cm, and does not exhibit any evidence of lymph node metastases, the last resort is surgery, either a total thyroidectomy or a lobectomy. Unilateral or bilateral neck dissection is advised for patients with advanced primary malignancies, depending on the size of local lymph nodes and the requirement for further staging [1,9]
The American Thyroid Association (ATA) therapy guidelines state that a lobectomy is adequate for tumors under 1 cm, but a total thyroidectomy is recommended for tumors bigger than 4 cm. Thyroid lobectomy is the recommended treatment for low-risk carcinomas that are greater than 1 cm but smaller than 4 cm [10].
We detailed a unique case of FVPTC that presented in a young woman of 22 years of age. She underwent three thyroid surgeries for total removal of this carcinoma but still retained a thyroid remnant in her neck. Thus, making this case rare and unique by making it beyond the limits of surgery, on one hand, and the patient being clinically and biochemically normal, on the other hand.
Case presentation
A 22-year-old woman from Punjab province in Pakistan, with no known comorbidities and no family history of thyroid cancer, initially presented 10 years ago in 2014 in the ear, nose, and throat (ENT) outpatient department with a complaint of painless, progressively increasing anterior neck swelling for the last year. Neck examination showed a firm to hard 4 x 4 cm swelling in the center of the neck, mobile on deglutition, nontender with normal color and temperature, noncystic, and irreducible. Thyroid function tests (serum TSH, T4, and T3 levels) were normal; however, FNAC revealed Bethesda III, and USG thyroid performed in October 2014 revealed multinodular goiter TIRAD 3. In February 2015, the patient had a diagnostic hemithyroidectomy, and the histology report showed an FVPTC. In April 2015, the patient underwent a total thyroidectomy due to the diagnosis of FVPTC. The patient recovered completely and well. The patient was started on 50 mcg of thyroxine twice a day orally (BD). Three monthly thyroid function tests were performed, and the results were within the normal range on nearly all follow-ups. A chronologically ordered, step-by-step surgical intervention done on this patient is shown in Figure 1.
Stepwise surgical intervention done in chronological order
The patient was doing well until November 2023, at which point she began experiencing intermittent dizziness, shortness of breath when walking, and generalized weakness. The patient saw a general practitioner, who ordered a full blood count since the patient appeared pale and had a USG thyroid scan, even though the patient did not exhibit any other thyroid disease symptoms, such as neck pain or swelling. The result showed that the patient’s hemoglobin was 9.4 mg/dl, and coincidentally, USG revealed a thyroid remnant in the isthmus measuring 1.7 x 0.7 cm, as shown in Figure 2. The patient had a thyroid scan that showed remnant tissue in the isthmus, as shown in Figure 3. Contrast-enhanced computed tomography (CECT) of the head and neck showed a thyroid remnant in the region of the isthmus measuring 0.86 x 1.44 cm, as shown in Figure 4. The antithyroid antibodies and tumor markers for thyroid cancer came out to be negative.
USG thyroid showing thyroid remnant at the level of isthmus (post-total thyroidectomy)USG: ultrasonography
Thyroid scan of patient before and after every surgery, showing constant thyroid remnant
Contrast-enhanced computed tomography neck showing thyroid remnant at the level of isthmus (post-total thyroidectomy)A and B: coronal view showing thyroid remnant as shown by the arrow; C and D: axial view showing thyroid remnant as shown by arrow
The patient underwent a complete thyroidectomy with bilateral level 1 neck dissection in June 2024. The surgeons' perioperative examinations showed that there was no obvious thyroid remnant visible at the site shown in radiological investigations, and the surgeon removed all the visible tissue in front of the trachea and from the potential remnant location. The histopathology report, as shown in Figure 5, showed muscle fiber and fibroadipose/cartilaginous tissue and no histological evidence of any thyroid tissue; the lymph nodes were also free of tumors.
Histopathology picture of completion thyroidectomy specimen without any evidence of thyroid tissueA: photomicrograph showing fibroadipose tissue with entrapped skeletal muscle bundles; B: photomicrograph showing nerve bundle with fibroadipose tissue and dilated vessels
The case was discussed in a multidisciplinary team meeting with representatives from the fields of oncology, nuclear medicine, ENT-head and neck surgery, endocrinology, and internal medicine. Given that the patient was symptomless and had normal thyroid function test results, negative thyroid antibodies and tumor markers, and no nodal or lymphovascular invasion, the patient was put on regular follow-up with no further surgical intervention or radioactive iodine ablation to be done for now.
Discussion
This case report details a distinct manifestation of thyroid follicular variant papillary cancer because of the patient's unusual demographics. We presented an unusual case of FVPTC in a 22-year-old young female patient, where this carcinoma silently survived for over 10 years even after having three thyroid surgeries with the aim of totally eradicating the disease but failing to do so. This symptomless patient was then kept on regular follow-ups with close monitoring. PTC commonly affects women (between 2:1 and 4:1), and the median age at which a patient usually presents is 50 years [1,2]. The patient we described was a 22-year-old woman who was otherwise healthy. Furthermore, in PTC, the tumor size is usually around 1 cm to 3 cm, but in our case, it was exceptionally larger, measuring approximately 5 x 3 x 2 cm [11].
For patients with FVPTC with tumors measuring more than 1.5 centimeters, lobectomy or total thyroidectomy are the two main possible surgical options [12]; some doctors advise a complete thyroidectomy, and so that was the surgical plan in our case, where we aimed for total thyroidectomy. Additionally, recommendations state that a lobectomy suffices for the encapsulated, noninvasive FVPTC [13].
To minimize the amount of residual thyroid tissue, total/near thyroidectomy is advised by the 2015 ATA guidelines and in certain papers [14]. This procedure can increase the likelihood of a successful total removal and reduce the rates of recurrence, distant metastasis, and mortality. Therefore, we kept the patient on regular follow-ups instead of having a thyroid remnant in the end. Holsinger et al. [15] in their research concluded that thyroid remnants are nearly always present, despite surgeons' radical intentions, and the removal of all thyroid tissue via complete thyroidectomy is still a "myth" and so was in our case.
According to Pan et al.'s study [16], only 2.2% of patients had a true total thyroidectomy, meaning that no remnant was discovered after the procedure. The rest of the patients, however, had some thyroid remnant that was visible using any imaging modality. In addition, a substantial thyroid remnant was seen in 14.7% of patients, which is what happened in our instance. In their study of all thyroidectomy patients, Salvatori et al. [17] discovered that 93.1% of patients had thyroid remnants. However, even after three thyroid surgeries, our patient experienced no surgical issues.
According to Zidan et al. [18], there is disagreement over the ideal surgical extent. According to them, the proportion of patients who had a total thyroidectomy and a subtotal thyroidectomy was comparable in both PTC and FVPTC, and the survival rates of the thyroidectomy and subtotal thyroidectomy groups were identical.
Conclusions
This case report illustrates an unusual presentation and resistance to complete removal of FVPTC even after multiple surgeries. Thus, there could be a chance of remnant being left behind even after complete thyroidectomy, and the patient may be totally symptomless, giving the impression that this tumor was beyond the limits of surgery in our case. Also, the literature review gave the impression that it is not uncommon to have a thyroid remnant after total thyroidectomy for any reason; most of the time, it's an incidental finding.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Papillary Thyroid Carcinoma Limaiem F Rehman A Mazzoni T Treasure Island (FL)Stat Pearls Publishing 2024 https://www.ncbi.nlm.nih.gov/books/NBK 536943/30725628 · pubmed ↗
- 2Thyroid carcinoma Lancet Sherman SI 50151136120031258396010.1016/s 0140-6736(03)12488-9 · doi ↗ · pubmed ↗
- 3Thyroid Cancer Lee K Anastasopoulou C Chandran C Cassaro S Treasure Island (FL)Stat Pearls Publishing 2025 https://pubmed.ncbi.nlm.nih.gov/29083690/29083690 · pubmed ↗
- 4Risk group stratification and prognostic factors in papillary carcinoma of thyroid Ann Surg Oncol Shaha AR Shah JP Loree TR 53453831996891548410.1007/BF 02306085 · doi ↗ · pubmed ↗
- 5Increasing incidence of thyroid cancer in the United States, 1973-2002 JAMA Davies L Welch HG 2164216729520061668498710.1001/jama.295.18.2164 · doi ↗ · pubmed ↗
- 6Clinical behavior of follicular variant of papillary thyroid carcinoma: presentation and survival Laryngoscope Lin HW Bhattacharyya N 71271612020102020524110.1002/lary.20828 · doi ↗ · pubmed ↗
- 7Follicular variant of papillary thyroid carcinoma is a unique clinical entity: a population-based study of 10,740 cases Thyroid Yu XM Schneider DF Leverson G Chen H Sippel RS 126312682320132347734610.1089/thy.2012.0453 PMC 3787730 · doi ↗ · pubmed ↗
- 8Trends in the presentation, treatment, and survival of patients with medullary thyroid cancer over the past 30 years Surgery Randle RW Balentine CJ Leverson GE Havlena JA Sippel RS Schneider DF Pitt SC 13714616120172784291310.1016/j.surg.2016.04.053PMC 5164945 · doi ↗ · pubmed ↗