Obstructive Jaundice as a Presenting Symptom of Acute Lymphocytic Leukemia in Adults: A Case Report
Sami M Al-Shehab, Tayseer K El Saheb

TL;DR
A 58-year-old man with obstructive jaundice was later diagnosed with acute lymphoblastic leukemia, highlighting the disease's varied symptoms.
Contribution
This case report highlights an atypical presentation of acute lymphoblastic leukemia as obstructive jaundice in an adult.
Findings
Obstructive jaundice was initially diagnosed due to elevated direct bilirubin levels.
Bone marrow analysis revealed blast cell infiltration consistent with B-cell acute lymphoblastic leukemia.
CD20 positivity confirmed the B-cell lineage of the leukemia.
Abstract
We present a unique case of acute lymphoblastic leukemia in an adult. A 58-year-old male presented complaining of epigastric pain. He was initially diagnosed with obstructive jaundice, as indicated by an elevated ratio of direct bilirubin to total bilirubin levels. Bone marrow aspirate revealed hypercellular marrow with heavy infiltration of blast cells. The target cells were positive for CD20 by immunostaining. This finding is consistent with acute lymphoblastic leukemia B cell type. This case emphasizes that acute lymphoblastic leukemia can exhibit a wide range of symptoms and should be considered a differential diagnosis, especially when encountering atypical obstructive jaundice.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
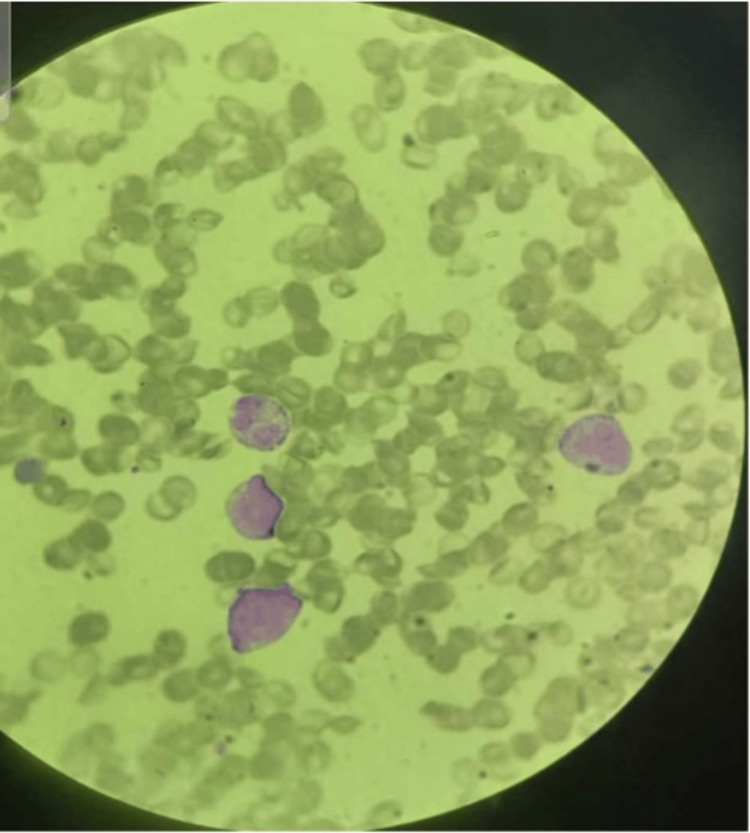 Figure 1
Figure 1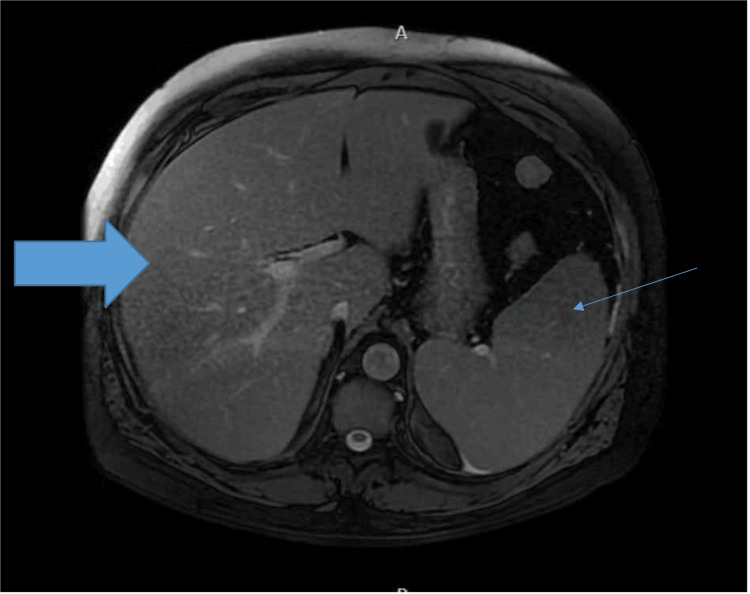 Figure 2
Figure 2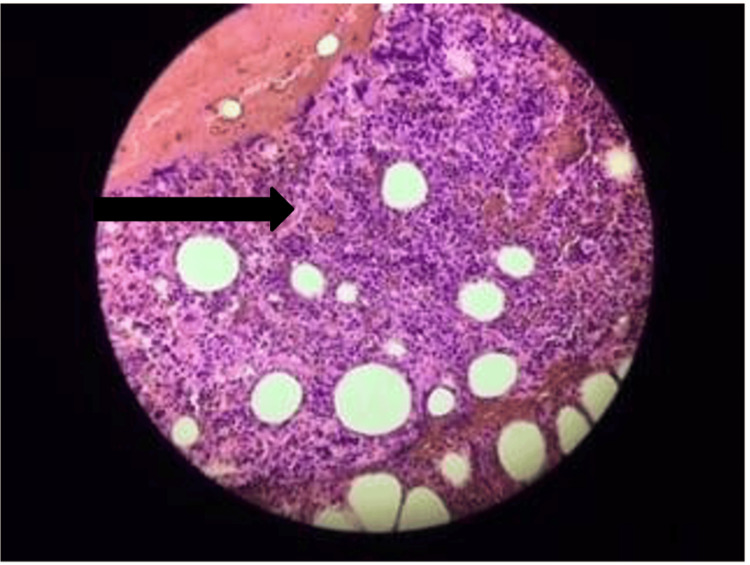 Figure 3
Figure 3| Test | Value | Normal range |
| Hemoglobin | 12.3 g/dL | 14–17 g/dL |
| White blood cell count | 12.9 * 10 ^3/µL | 4–10 * 10 ^3/µL |
| Neutrophils | 17% | 40–75% |
| Lymphocytes | 76% | 25–45% |
| Platelet count | 62000/µL | 140000–450000/µL |
| Creatinine | 1.5 mg/dL | 0.5–1.35 mg/dL |
| Urea | 50 mg/dL | 11–50 mg/dL |
| Uric acid | 9.2 mg/dL | 2.5–6 mg/dL |
| Sodium | 142 mmol/dL | 135–150 mmol/dL |
| Potassium | 4.6 mmol/dL | 3.5–5.3 mmol/dL |
| Total bilirubin | 10.2 mg/dL | 0.2–1.2 mg/dL |
| Direct bilirubin | 6.2 mg/dL | 0–0.3 mg/dL |
| Alanine aminotransferase | 73 U/L | 10–65 U/L |
| Aspartate aminotransferase | 68 U/L | 0–40 U/L |
| Gamma-glutamyl transferase | 330 U/L | 7–55 U/L |
| Alkaline phosphatase | 179 U/L | 40–136 U/L |
| Antinuclear acid antibody titer | <1:80 | <1:80 |
| Anti-smooth muscle antibody titer | <1:10 | <1:10 |
| Anti-mitochondrial antibody titer | <1:10 | <1:10 |
| C-reactive protein | 18 mg/L | 0–5 mg/L |
| Lactate dehydrogenase level | 370 U/L | 80–250 U/L |
| Phosphorus level | 7.4 mg/dL | 2.5–5 mg/dL |
| Hepatitis profile | Negative | Negative |
| Epstein-Barr virus | Negative | Negative |
| Cytomegalovirus | Negative | Negative |
| Prothrombin time | 14.1 s | 12–16 s |
| International normalization ratio | 1.007 | 1 |
| Partial thromboplastin time | 32 | 25–35 s |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Lymphoblastic Leukemia research · Neonatal Health and Biochemistry · Pediatric Hepatobiliary Diseases and Treatments
Introduction
Acute leukemia is the uncontrolled proliferation of malignantly transformed hematopoietic stem cells [1], constituting the most common childhood cancer [2]. Conversely, acute lymphocytic leukemia denotes a malignancy of lymphocyte precursor cells [3]. Acute lymphoblastic leukemia constitutes approximately 12% of leukemia cases. Leukemic cells have the ability to migrate and invade different types of tissues [4] and are usually diagnosed via bone marrow aspirate. Moreover, acute lymphoblastic leukemia predominantly affects the pediatric age group, but carries a poorer prognosis if it presents in adults [5]. Acute lymphoblastic leukemia seldom manifests with abdominal pain and jaundice in adult patients. In this case report, we present a patient with acute lymphoblastic leukemia with right upper quadrant pain and jaundice.
Case presentation
A 58-year-old male patient presented to the Emergency Department of Istiklal Hospital in Amman, Jordan, complaining of epigastric pain that was progressive, constant, and radiating to the right upper quadrant over the past two weeks. The pain intensified after consuming fatty food and was alleviated with vomiting. Concurrently, the patient displayed yellowish discoloration in both eyes, general weakness, nausea, and bilious vomiting on five separate occasions. Additionally, the patient reported dark urine but no change in stool color. The patient reported no changes in bowel habits, itching, recent weight loss, history of drug or alcohol abuse, or the use of pain medications.
Upon examination, the patient exhibited jaundiced sclera and skin, along with epigastric pain, tenderness in the right upper quadrant, and a positive Murphy’s sign. Consequently, the patient was diagnosed and admitted for obstructive jaundice, as indicated by an elevated ratio of direct bilirubin to total bilirubin levels, as seen in Table 1.
Blood smear analysis revealed normocytic normochromic red blood cells with few macrocytes and polychromasia, anisocytosis, occasional normal red blood cells, normal white blood cells, few atypical lymphocytes, and marked thrombocytopenia (Figure 1).
Blood smear exhibiting atypical lymphocytes.
On magnetic resonance cholangiopancreatography, the biliary tree was not dilated, with a prominent left lobe of the liver and splenomegaly measuring approximately 14.7 cm (Figure 2).
Magnetic resonance cholangiopancreatography revealing an enlarged liver and splenomegaly (thin arrow).
The patient was initiated on ursodeoxycholic acid 150 mg orally every six hours (to promote secretion of bile acid), with intravenous fluid, and ceftriaxone 1 gm intravenously every 12 hours (due to suspected ascending cholangitis). Prednisolone 5 mg orally, two tablets every 12 hours, was added after magnetic resonance cholangiopancreatography revealed no biliary obstruction.
On day five following admission, the patient’s laboratory test findings revealed the following: white blood cell count of 0.7 * 10^3/µL, platelet count of 15 * 10^3 /µL, reticulocyte count of 1.4%, and total bilirubin level of 5 mg/dL (direct bilirubin level = 3.1 mg/dL).
Bone marrow aspiration was performed (indicated by the massively reduced white blood cell and platelet counts) on the same day. Analysis revealed hypercellular marrow with heavy infiltration of blast cells (Figure 3). Further, the target cells were positive for CD20 and negative for CD117, CD3, and myeloperoxidase by immunostaining. This finding is consistent with that of acute lymphoblastic leukemia B cell type.
Hypercellular bone marrow with heavy infiltration of blast cells (black arrow).
Repeated blood smears were performed and revealed severe leukopenia, no blast cells, and severe thrombocytopenia. The patient was then initiated on chemotherapy and went into complete remission. He received the hyper-CVAD protocol, beginning with induction course A, including cyclophosphamide 300 mg/m² IV over two hours every 12 hours for six doses on days one to three with mesna uroprotection, vincristine 2 mg IV on days four and 11, doxorubicin 50 mg/m² IV on day four, and dexamethasone 40 mg orally (PO) on days one to four and 11 to 14, alternating every three to four weeks with consolidation course B, which comprised methotrexate 200 mg/m² IV over two hours, followed by 800 mg/m² IV over 22 hours on day one with leucovorin rescue, and cytarabine 3 g/m² IV over two hours every 12 hours for four doses on day two (reduced to 1 g/m² for patients >60 years), plus methylprednisolone 50 mg IV every 12 hours on days one to three for CNS prophylaxis. Maintenance therapy was planned post‑remission with 6‑mercaptopurine 75 mg/m² PO daily, methotrexate 20 mg/m² PO weekly, and monthly vincristine 2 mg IV plus prednisone 40 mg/m² PO on days one to five every three months, with each cycle administered at 21‑day intervals and close monitoring of hematologic and organ function.
Discussion
To the best of our knowledge, we have encountered only two similar cases of acute lymphoblastic leukemia in patients presenting with right upper quadrant abdominal pain and jaundice similar to obstructive jaundice. In the first case, a 43-year-old male presented with epigastric pain and jaundice and was diagnosed with acute lymphoblastic leukemia [6]. The second case involved a 44-year-old male who presented with right upper quadrant abdominal pain and obstructive jaundice [7]. In both instances, the treatment approach consisted of standardized chemotherapy for acute lymphoblastic leukemia, supplemented by a short course of prednisone before initiating chemotherapy. There was a substantial reduction in bilirubin levels and alleviation of abdominal pain.
The mechanism behind the jaundice and abdominal pain is thought to be due to hepatic sinusoidal infiltration of leukemic cells [8]. The diagnosis is usually confirmed by bone marrow biopsy findings, revealing heavy infiltration of blast cells [7].
In conclusion, acute lymphoblastic leukemia can manifest in various ways, none of which are specific. Acute lymphoblastic leukemia should be suspected and included in the list of differential diagnoses when any abnormalities in complete blood count results are observed.
Conclusions
Acute lymphoblastic leukemia in adults can present with atypical symptoms such as obstructive jaundice and right upper quadrant pain, mimicking hepatobiliary pathology. In any adult patient with unexplained cholestatic liver enzyme elevations or obstructive jaundice, especially when routine imaging is non‐revealing, peripheral blood counts should be scrutinized for blasts or cytopenias. Prompt bone marrow evaluation remains the gold standard for diagnosis. Early recognition and initiation of standard acute lymphoblastic leukemia chemotherapy protocols, often preceded by a brief course of corticosteroids, can rapidly reverse hepatic infiltration, normalize bilirubin levels, and induce remission.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Acute leukemia in adults: recent developments in diagnosis and treatment CA Cancer J Clin Devine SM Larson RA 326352441994795391410.3322/canjclin.44.6.326 · doi ↗ · pubmed ↗
- 2Acute lymphocytic leukemia in the adolescent: diagnosis, treatment, and outcomes Adolesc Med Dunsmore KP 4070407-17, x-xi 101999 https://pubmed.ncbi.nlm.nih.gov/10611938/10611938 · pubmed ↗
- 3Acute lymphocytic leukemia in adults. Pathologic features and prognosis Rom J Intern Med Marinescu C Vlădăreanu AM Mihai F 3136532015 https://pubmed.ncbi.nlm.nih.gov/26076558/2607655810.1515/rjim-2015-0004 · doi ↗ · pubmed ↗
- 4Leukaemia: a model metastatic disease Nat Rev Cancer Whiteley AE Price TT Cantelli G Sipkins DA 4614752120213395337010.1038/s 41568-021-00355-z PMC 8722462 · doi ↗ · pubmed ↗
- 5Recent advances in managing acute lymphoblastic leukemia Am Soc Clin Oncol Educ Book De Angelo DJ Jabbour E Advani A 330342402020 https://doi.org/10.1200/EDBK_2801753242144710.1200/EDBK_280175 · doi ↗ · pubmed ↗
- 6Adult acute lymphoblastic leukemia presenting as jaundice Am J Gastroenterol Jha R Rampertab SD Chamberlain S 08992004 https://journals.lww.com/ajg/fulltext/2004/10001/adult_acute_lymphoblastic_leukemia_presenting_as.606.aspx
- 7Precursor B-cell acute lymphoblastic leukemia presenting as obstructive jaundice: a case report J Med Case Rep Siddique MN Popalzai M Aoun N Maroun R Awasum M Dai Q 26952011 https://doi.org/10.1186/1752-1947-5-269.2172237910.1186/1752-1947-5-269PMC 3141714 · doi ↗ · pubmed ↗
- 8Acute lymphoblastic leukemia Hematol Oncol Clin North Am Onciu M 6556742320091957716310.1016/j.hoc.2009.04.009 · doi ↗ · pubmed ↗