Co-production in HIV research: a case study from the COVID-19 pandemic
Vasiliki Papageorgiou, Jane Bruton, Halle Johnson, Silvia Petretti, Wezi Thamm, Joshua Anderson, Husseina Hamza, Helen Ward

TL;DR
This study explores how people living with HIV can co-produce research with academics, focusing on their experiences during the pandemic and offering lessons for future projects.
Contribution
The paper provides practical insights and recommendations for conducting remote co-produced research with people living with HIV during a global crisis.
Findings
Building trust and managing expectations is crucial for successful co-produced research.
Remote co-production is feasible with strong communication and adaptability.
Positive experiences in co-produced research may encourage future participation in research initiatives.
Abstract
Co-produced research is an approach where people with lived experience voluntarily engage as collaborators throughout the entire research process. In this study, academic researchers aimed to recruit and train people living with HIV, in partnership with a community-based organisation (Positively UK), with the objective of enhancing research skills and capabilities of the HIV community to lead and/or facilitate forthcoming research initiatives and projects. Our collaborative endeavour involved a group of academic researchers, a public involvement practitioner and people living with HIV (comprising two co-researchers and three advisory group members) to design and conduct a participatory, qualitative enquiry from January to September 2021. Our study aimed to explore the experiences of people living with HIV within the United Kingdom during the COVID-19 pandemic. All co-researchers…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1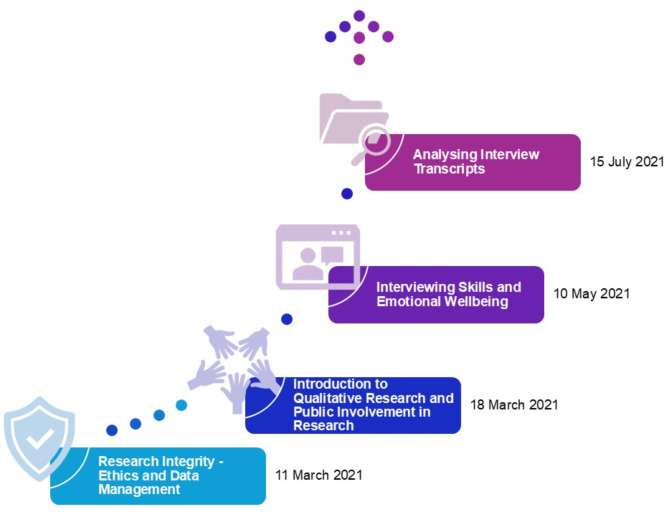 Figure 2
Figure 2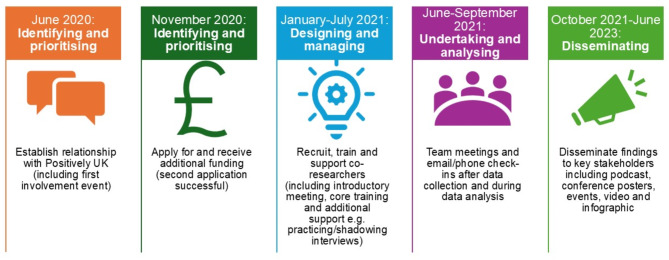 Figure 3
Figure 3- —http://dx.doi.org/10.13039/501100000761Imperial College London
- —http://dx.doi.org/10.13039/501100000269Economic and Social Research Council
- —http://dx.doi.org/10.13039/501100013342NIHR Imperial Biomedical Research Centre
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMental Health and Patient Involvement · HIV/AIDS Research and Interventions · Community Health and Development
Background
Participatory research is an approach where key stakeholders (e.g. service users, carers etc.) work in partnership with researchers to design and conduct a study [1]. Co-production (or co-research) is an example of a participatory approach in which people with lived experience are integral partners throughout the research process [2]. This approach is underpinned by the principles of reciprocity; sharing of power; building and maintaining relationships; including all perspectives and skills; and respecting and valuing the knowledge of all those working together [2]. Community-based participatory research (CBPR) acknowledges how the research is led “by communities for communities” and therefore has a role of translating research findings into actionable outcomes, including social change; CBPR rests on the pillars of ethics and community empowerment [3].
Several theories may be used in co-design, co-creation, and co-production of public health research [4]. Empowerment Theory focuses on how stakeholders can be empowered in processes such as co-creation, thereby linking individual well-being to the wider sociopolitical environment [4, 5]. Additionally, the EMERGES framework (Enablers and Empowerment; Motivation to Integrate; Empathy of the self and others; Recovery model and medical model; Growth and Transformation; Exclusion (Stigma and Discrimination); Survivor roots/Disability roots) was developed to outline the multifaceted identities of researchers or providers with lived experience [6]. The framework was developed through a systematic review in the context of mental health [6]. Nonetheless, components of these concepts can be transferred and used in HIV research. Specifically, the experiences of exclusion, stigma, and discrimination, aligned with the potential for public involvement aimed at fostering metaphorical personal and collective growth and transformation (for example, the development of a new professional identity or seeing teammates ‘blossom’), as well as a nuanced understanding and empathy of oneself and others [6, 7].
Participatory approaches are well established in the HIV response. A prevalent slogan among people living with HIV is “nothing about us,* without us”* which has its origins in the in disability rights movement [8]. Community-based organisations (CBOs) have championed the Greater and Meaningful Involvement of People Living with HIV (GIPA/MIPA) since the early days of the HIV epidemic [9]. Consequently, in HIV research, participatory approaches are progressively becoming more common [10]. However, researchers have argued for clarification regarding the terminology and definitions employed, in addition to a comprehensive framework delineating roles throughout the research cycle that aligns with specific needs and capacities of stakeholders [10].
The COVID-19 pandemic resulted in health services globally, including HIV clinics, having to rapidly adapt service delivery. For HIV clinics specifically, a need to maintain HIV care was identified early on during the pandemic [11]. For example, ensuring people living with HIV had access to antiretroviral therapy; the provision of pre- and post-exposure prophylaxis and HIV prevention tools; and adapting services including routine appointments and peer support to be delivered virtually rather than in-person [11, 12]. This presented several challenges relating to digital exclusion but also concerns for privacy and confidentiality [13, 14]. Concerns were also raised about the mental health and isolation of people living with HIV, particularly as the prevalence of mental health conditions is already high in the population [13, 14]. In the United Kingdom, some clinics had HIV staff redeployed to intensive care units during COVID-19 and at the start of the pandemic, information relating to shielding advice for people living with HIV was conflicting [12, 15, 16]. Specifically, the UK government had provided conflicting advice about whether people living with HIV should shield with some people receiving letters and text messages, despite the British HIV Association (BHIVA) and the Terrence Higgins Trust confirming this was unnecessary unless they are at the highest clinical risk of severe COVID-19 (e.g. people with CD4 count < 50 cells/microL) [17–19]. Finally, there were concerns of the impacts of COVID-19 on wider determinants of health including finances, housing and employment, particularly for the most vulnerable people living with HIV [12].
The COVID-19 pandemic also introduced a unique challenge to co-producing research as government restrictions necessitated a shift to remote activities. Despite these challenges, initial insights indicated that the public were keen to continue contributing their time and expertise to support the ongoing response [20].
Our aims were to:
-
recruit, appoint and train two qualitative researchers with lived experience to conduct and analyse interviews with people living with HIV;
-
recruit, appoint and train two advisory group members to provide guidance on the overarching strategy and progress of the project;
-
build new relationships and strengthen existing connections with people living with HIV to facilitate future co-research through prioritising study findings and disseminating results;
-
up-skill and build capacity for qualitative research within a CBO.
Methods and findings
Our approach builds on the reflections of two co-produced research projects [21, 22] and published recommendations [23, 24]. Due to the COVID-19 pandemic, the ‘community-based’ element of our project had to be transformed to work in an online/virtual space, rather than face-to-face. Here, we use the broad term ‘co-researchers’ to describe both the lived experience qualitative researchers and advisory group members, who were all living with HIV.
We frame our methods, reflections and recommendations using each stage of the research cycle according to the National Institute for Health and Care Research (NIHR) [25]. Figure 1 outlines our project timeline and Table 1 our recommendations for each stage of involvement in the research cycle.
Fig. 1. Project timeline overview (2020–2023) mapped to key stages in the research cycle
Table 1. Summary of recommendations for each stage of research cycleStage of research cycleRecommendationsIdentifying and prioritising• Academic researchers and public involvement practitioners should begin to build relationships with community-based organisations (CBOs) as early as possible.• Diversity and representation in the project team is essential to ensure all voices are heard. This includes sociodemographic factors such as age, gender, ethnicity and sexual orientation as well as years living with HIV (for people with lived experience involved). Conducting research remotely can also improve geographical representation within the team, particularly where people with lived experience live in rural or remote areas, although digital exclusion may be an issue.• Academic researchers and public involvement practitioners should identify any issues relating to technology/digital access, or knowledge, early on and ensure access or develop training to circumvent such issues arising. This may include offering additional avenues for those without access to technology to provide their insights to supplement online discussion groups.Funding and commissioning• Be flexible with funding budget – work with your community-based partner and adequately remunerate their involvement in the project, as well as the co-researchers. For example, understanding any equipment that might need to be ordered for your co-researchers (e.g. headphones) and preferences on the type of honorarium received (e.g. bank payment or vouchers).• Research funders and councils should develop more funding schemes to promote and support participatory approaches in research, with budgets ranging from low-level (advisory/consultation) to high-level (co-research) involvement.Designing and managing• Have an iterative and flexible approach to training that facilitates opportunities for co-researchers to provide feedback on the skills they feel most and least confident about. These insights can then be used to inform and enhance the design, content, and delivery of training sessions.• Training should be developed that is mindful of the histories, backgrounds, and experiences of the co-researchers (e.g. HIV-related stigma, traumatic experiences etc.).• Emotional well-being is a fundamental component of any type of participatory study and should be mandatory in training.• Links to support services (e.g. collaborating with a support organisation) can assist with developing appropriate tools and interventions.• Manage expectations on what can and cannot be achieved given resources and time.• Spend time getting to know the team on a personal level through icebreakers and allowing time in meetings for such personal information sharing discussions – what skills, hobbies and interests do people have? This can help co-researchers settle in, feel comfortable and familiarise with a project where they may be new to research and/or collaborating with the researcher.• Explore what co-researchers hope to get out of the project (e.g. future research opportunities, forms of recognition, further training or skills development for roles outside of academia).Undertaking and analysing• Encourage co-researchers to voluntarily share their backgrounds either at the start or end of the interview process with participants to help build rapport (if they feel comfortable).• Manage expectations of co-researchers about “no shows” or participants withdrawing from the interview process by explaining this during training and at check-in sessions during data collection.• Schedule debriefing meetings after interviews – an initial check-in email immediately afterwards followed by a call/team meeting for specific issues to allow time for co-researchers to reflect on any concerns.• Co-researchers could also mentor and support each other in team meetings by sharing reflections from their experiences.• Development of more in-depth, in-person training on qualitative data analysis to facilitate learning, support, and active participation.• Ensure adequate time is scheduled for data analysis and consider creative methods of coding when institutional tools (e.g. NVivo) may not be available for co-researchers.Disseminating• All key stakeholders should be involved in planning the dissemination of the research findings as this collaboration could assist with prioritising who, how and where findings should be shared/disseminated.• Creative forms of dissemination (which are co-produced) help to increase research impact, particularly if developed to be accessible in terms of language and style.Implementing and evaluating feedback• Determine the best approach and timepoints for self-reflection at the start of the project, as a group, with this formally agreed by all team members.• Be open to continuing dialogue beyond the research project to self-reflect as academic researchers and co-researchers and make changes for future co-produced research.
Identifying and prioritising: Building relationships and managing expectations
In 2020, we began collaborating with the peer-led HIV support charity, Positively UK [26]. One of the academic researchers (JB) was a Trustee of Positively UK at the time and was aware of the organisation’s motivation to develop internal research capacity, particularly amongst volunteers. Therefore, we were able to build a strong connection from an existing trusting relationship between a member of the academic research team (JB) and the CEO of the charity (SP). Our first community involvement activity was an online event1, ‘COVID-19 Community Involvement: Let’s Talk About… HIV care’, and aimed to gather insights on the challenges and opportunities presented to HIV care during the pandemic. The event, hosted by PERC on Zoom, was attended by 25 people from across the UK including people living with HIV, and providing HIV services and working at HIV charities. The event consisted of a short presentation and breakout room discussions (five rooms) each facilitated by a member of Positively UK and a PERC staff member (as a note-taker). The session aimed to shape the design and focus of the qualitative study. Priorities and views shared during this online session directly fed into the development of this project, with those in attendance highlighting the need to further explore the impact of COVID-19 on those living with HIV and the services and care available and received. Furthermore, insights gained were later used for the development of interview questions for subsequent qualitative studies as well as to identify interested participants. Details on the approach and findings are published elsewhere [12].
Following the event, we ran a debriefing session with all the facilitators to identify key messaging for the insight report [12] as well as reflections on the involvement activity.
Reflections
During the debrief, we identified what worked well and areas of improvement (Table 2). We identified how trust and rapport when building relationships is essential, particularly when all interactions are remote and with novice HIV researchers. Engaging regularly, early in the project, and with respect have been identified as important metrics when working with people with lived experiences [28]. Additionally, issues relating to access to technology and data were raised as well as ensuring that the research team was inclusive and diverse in terms of age, gender, ethnicity and geographical location.
Table 2. Reflections from Zoom event by facilitators. Adapted from Papageorgiou et al. [12]What worked wellWhat could be improvedAttendees felt open to share their experiences from both a clinical and personal perspectiveIssues of digital exclusion – other ways to involve for people who do not use, are unfamiliar with or do not have access to, ZoomHaving Positively UK facilitating and being part of the community involvement activity and research process – sharing experiences helped foster an enabling environment for attendees to open upLimited time which meant some discussions had to end quicklyThe facilitators involved were from diverse backgrounds and being a team of predominantly women worked wellGender imbalance (one male co-facilitator) may result in biasHaving a mixed group of participants including clinicians allowed for in-depth discussions on different areas of HIV care (NHS services, voluntary sector etc.)There were some technical issues with a few participants sending emails after the event to explain that they could not re-join the call after breakout discussions
Recommendations
• Academic researchers and public involvement practitioners should begin to build relationships with CBOs as early as possible.
• Diversity and representation in the project team is essential to ensure all voices are heard. This includes sociodemographic factors such as age, gender, ethnicity and sexual orientation as well as years living with HIV (for people with lived experience involved). Conducting research remotely can also improve geographical representation within the team, particularly where people with lived experience live in rural or remote areas, although digital exclusion may be an issue.
• Academic researchers and public involvement practitioners should identify any issues relating to technology/digital access, or knowledge, early on and ensure access or develop training to circumvent such issues arising. This may include offering additional avenues for those without access to technology to provide their insights to supplement online discussion groups.
Funding and commissioning: flexibility and seeking opportunities
Due to the nature of an ongoing outbreak, we had to swiftly identify available funding to enhance and support the project, particularly the remuneration of co-researchers in line with NIHR guidelines [29]. We (VP, JB, HW, HJ) co-developed a funding application2 with our collaborator (SP) and secured a budget to cover the costs of two co-researchers and two advisory group members as part of the project.3 We later re-applied to the same funder for further funding, from a different scheme, to support the dissemination of research findings.
Reflections
We identified few appropriate funding schemes to support co-research as there were no specific funds for HIV research.
Recommendations
• Be flexible with your funding budget – work with your community-based partner and adequately remunerate their involvement in the project, as well as co-researchers. For example, understanding any equipment that might need to be ordered for your co-researchers (e.g. headphones) and preferences on the type of honorarium received (e.g. bank payment or vouchers).
• Research funders and councils should develop more funding schemes to promote and support participatory approaches in research, with budgets ranging from low-level (advisory/consultation) to high-level (co-research) involvement.
Designing and managing: reciprocal learning
Two lived experience qualitative researchers and three advisory group members including one collaborator also with lived experience, were recruited and trained between January and October 2021. We designed our research approach based on published reflections from colleagues [21] and amended an ethics application already in place for another qualitative study4 to incorporate the participatory component for this project. As a result, most of the study documents were already created; however, co-researchers were asked to review and provide feedback on all the documents including the protocol, interview guide, participant information sheet, a demographics survey and resource list. The results of this activity are outlined elsewhere [30].
Core training sessions (Fig. 2) were designed and focused on building skills identified to be essential for roles from the research perspective as well as skills which were identified by co-researchers as areas of development using a “skills review” [31]. The skills review included reflections on experiences/knowledge of public involvement in medical research (e.g. contextual knowledge about HIV and COVID-19) and general skills, expertise, and knowledge (e.g. using virtual meeting platforms such as Zoom) [31]. We (VP, JB, HJ) used several existing resources to develop the training sessions. First, training on research integrity, including ethics, were designed in line with institutional requirements. As suggested by our collaborator at Positively UK (SP), training on ethics specifically focussed on issues around confidentiality, safeguarding and respecting boundaries. Ensuring appropriate support is in place for emotionally challenging research (for example, where team members have lived experience of the research topic) is essential and has also been reported in recent co-produced HIV studies as well as in other fields of health research [32, 33]. Second, the session on qualitative research and public involvement was adapted from Bees et al. [34]. Third, we developed our interviewing training to also cover emotional well-being of peer interviewers based on recommendations from other HIV researchers and organisations [23, 24, 35]. Finally, the training and approach of analysing interview transcripts was adapted from the DEPICT5 model [36]. Training session materials have been deposited online and are freely available to use [37].
Fig. 2. Overview of core co-researcher training session from March to July 2021
Additionally, during some research team meetings and one-to-one discussions, we had brief training sessions on other aspects which were not previously covered. For example, we discussed how to conduct interviews using Zoom and how to present research in academic writing (specifically writing conference abstracts). We also used time for reflections on skills development during the project.
Reflections
Research team meetings provided time to reflect on all progress made and for learning and information sharing between researchers and people living with HIV (in both directions). One co-researcher explained how they appreciated the depth and breadth of training,…the training is really helpful; you get to realise the amount of work and people that are involved in a research project.
Recommendations
• Have an iterative and flexible approach to training that facilitates opportunities for co-researchers to provide feedback on the skills they feel most and least confident about. These insights can then be used to inform and enhance the design, content, and delivery of training sessions.
• Training should be developed that is mindful of the histories, backgrounds, and experiences of the co-researchers (e.g., HIV-related stigma, traumatic experiences etc.).
• Emotional well-being is a fundamental component of any type of participatory study and should be mandatory in training.
• Links to support services (e.g. collaborating with a support organisation) can assist with developing appropriate tools and interventions.
• Manage expectations on what can and cannot be achieved given resources and time.
• Spend time getting to know the team on a personal level through icebreakers and allowing time in meetings for such personal information sharing discussions – what skills, hobbies and interests do people have? This can help co-researchers settle in, feel comfortable and familiarise with a project where they may be new to research and/or collaborating with the researcher.
• Explore what co-researchers hope to get out of the project. For example, future research opportunities, forms of recognition, further training, or skills development for roles (outside of academia).
Undertaking and analysing: flexibility and ensuring all voices are heard
We (VP) sampled participants from the 2017 Positive Voices study which is a nationally representative survey on the health and well-being of people living with HIV in England and Wales [38]. We approached 260 of 1,231 participants with valid contact details who were happy to be contacted about future research. Our recruitment approach and methods are outlined in full elsewhere [30]. In total, 19 interviews were conducted with people living with HIV between June and August 2021; five of these interviews were undertaken by two co-researchers and 14 by two academic researchers.
We scheduled check-in meetings with co-researchers and research team meetings for all members on Zoom or by phone. Check-in meetings were scheduled immediately after any interviews to discuss any issues raised as well as time scheduled during fortnightly team meetings to discuss any difficult conversations. Our partner, Positively UK, were also available to provide peer support, if required by co-researchers. Both qualitative co-researchers had a criminal record check by the Disclosure Barring Service (DBS) before conducting any interviews.
Google Jamboard was the preferred method for recording notes from research team meetings. For the qualitative analysis, each team was assigned a minimum of one transcript to code by thematic analysis, with co-researchers given transcripts from interviews they completed. All co-researchers received training on the importance of data protection and management [37] and had signed a non-disclosure agreement prior to data collection which outlined the importance of handling any sensitive data (i.e. transcripts). Transcripts were password-protected before transfer to an encrypted Microsoft OneDrive for Business folder with permissions set for ‘view only’ to prevent downloads of the file to any personal devices. We completed a whole team analysis using Google Jamboard to manage codes, categories, themes and sub-themes. All the data (code, categories, themes) were then transferred into NVivo as a coding framework, with coding applied to all transcripts by one of the academic researchers (VP).
Reflections
Some tasks were easier to co-produce than others; for example, most co-researchers were confident when interviewing if this was framed as a conversation and they were able to follow a topic guide with open-ended prompts or examples given as prompts. However, data analysis using a participatory approach was more challenging as the interview transcripts were lengthy given that the interviews lasted up to 90 minutes. Moreover, the analysis also took place during the summer months when the team members were on leave which delayed the process. Additionally, some team members experienced technical issues accessing the transcripts. These were troubleshooted by the lead researcher, who in some instances had to share the correct password for members to open files, by phone. Involving qualitative co-researchers may have improved the experiences of participants by helping to build deeper rapport, free from judgement and from a place of understanding that enhances knowledge creation although, the approach may also introduce an emotional burden or blur personal and professional boundaries [39, 40].
Recommendations
• Encourage co-researchers to voluntarily share their backgrounds either at the start or end of the interview process with participants to help build rapport (if they feel comfortable).
• Manage expectations of co-researchers about “no shows,” or participants withdrawing from the interview process by explaining this during training and at check-in sessions during data collection.
• Schedule debriefing meetings after interviews – an initial check-in email immediately afterwards followed by a call/team meeting for specific issues to allow time for co-researchers to reflect on any concerns.
• Co-researchers could also mentor and support each other in team meetings by sharing reflections from their experiences.
• Development of more in-depth, in-person training on qualitative data analysis to facilitate learning, support, and active participation.
• Ensure adequate time is scheduled for data analysis and consider creative methods of coding when institutional tools (e.g. NVivo) may not be available for co-researchers.
Disseminating: impact beyond academic outputs
We worked as a group to develop a dissemination plan (Fig. 3) and prioritised outputs according to stakeholders and timings; for example, community and participant-facing communications were prioritised in line with ‘best practice’ to recognise and appropriately respect their contributions to the research [41, 42].
Fig. 3. Dissemination plan co-designed by the group using Google Jamboard. Taken from Papageorgiou (2022) [30]
Our outputs include:
-
A co-produced reflective workshop at a conference alongside other participatory projects on “building and sustaining partnerships” co-designed and co-facilitated by co-researchers (HH, WT) [33, 43].
-
An infographic presenting our preliminary findings for all study participants.
-
A podcast episode on our experiences working together during the pandemic featuring reflections from an academic researcher (VP) and co-researcher (HH) [44].
-
A co-produced workshop for academic staff/students on how to conduct co-research co-facilitated by a co-researcher (WT).
-
A co-produced showcase event to highlight the research findings and conduct participatory activities with key stakeholders, including prioritisation of research findings [45, 46]. This included the development of a short video on our experiences working together and why co-research promotes more meaningful and impactful research [47] and a visual illustration was produced during the event [46]. Key stakeholders invited to attend the event included people living with HIV (e.g. those interviewed as part of the study), HIV charities and CBOs, policymakers, pharmaceutical companies, professional medical bodies, researchers and clinicians.
-
Two co-designed conference posters at international conferences; one was presented by a co-researcher (HH) [48, 49]. One co-researcher (WT) also received a scholarship to attend a conference virtually.
-
A blog published on the Positively UK website [50] providing a summary of our project and signposting to further information on our study webpage [51].
Reflections
Co-researchers wanted any public-facing documents to be prioritised and were keen for these to be visually and audibly accessible, rather than in word format); these outputs also had the greatest reach [30]. Key stakeholders from the showcase event assisted us to disseminate our findings and prioritising the importance of each finding [30, 46].
Recommendations
• All key stakeholders should be involved in planning the dissemination of the research findings as this collaboration could assist with prioritising who, how and where findings should be shared/disseminated.
• Creative forms of dissemination (which are co-produced) help to increase research impact, particularly if developed to be accessible in terms of language and style.
Implementing and evaluating impact: embedding continuous reflection
Initially, this step was to be embedded throughout the project through guided self-reflection activities. However, time constraints and limited uptake from co-researchers, resulted in this occurring at the end of the project and in more informal ways. For example, feedback from co-researchers received by emails and phone were recorded and published elsewhere [30].
Reflections
We aimed to advocate for empowerment as a group by ensuring that all voices were heard, actions were taken, and the impact of involvement was recorded. However, the uncertainty of the pandemic meant that we had to be flexible and open to unexpected challenges including life events and the nuances of conducting research during a pandemic.
Several of the co-researchers have continued to be involved in research (JA, HH, WT) and WT has since developed and led her own research project which aligns with literature on empowerment [6, 52]. Reflections of involvement have continued beyond the closure of this distinct research project.
Recommendations
• Determine the best approach and timepoints for self-reflection at the start of the project, as a group, with this formally agreed by all team members.
• Be open to continuing dialogue beyond the research project to self-reflect as academic researchers and co-researchers and make changes for future co-produced research.
Conclusions
HIV research lends itself to co-research due to its underlying roots in advocacy and empowerment. However, the COVID-19 pandemic raised specific challenges to conducting co-research which required iterative adaptations and creativity. Well-designed and thorough training sessions are key to ensuring co-researchers feel confident and supported when joining a research team. Creative forms of dissemination which are co-designed and co-produced by people with lived experience enhance the reach and impact of research projects, ultimately driving transformation at a service level. Developing trust between research team members early on can enhance the experiences of all involved and facilitate the development of confidence, new skills, empowerment and relationships throughout the project. Overall, our co-produced study provided the opportunity for the experiential knowledge of team members to influence the approach and interpretation of findings. This ensured that the research remained meaningful and relevant to people with HIV and the findings and recommendations were grounded in lived experience. Our approach resulted in the enhancement of research skills and capabilities within the HIV community and has led to co-researchers continuing to be involved with, or beginning to lead their own, research.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1National Institute for Health and Care Research. Glossary [Internet]. 2022. Available from: https://www.nihr.ac.uk/glossary/
- 2Hickey G, Brearley S, Coldham T, Denegri S, Green G, Staniszewska S et al. Guidance on co-producing a research project [Internet]. Southampton; 2018. Available from: https://www.learningforinvolvement.org.uk/wp-content/uploads/2021/04/Guidance-on-co-producing-a-research-project-2022.pdf
- 3AIDS United, US People Living with HIV Caucus. Embodying Meaningful Involvement of People Living with HIV: History and Lessons Learned from the Community [Internet]. Washington, DC. 2019 Sep. Available from: http://aidsunitedbtc.wpengine.com/wp-content/uploads/2021/05/MIPA_Toolkit_FINAL.pdf
- 4British HIV Association and Terrence Higgins Trust (THT). Comment from BHIVA and THT on UK Government Guidance on Coronavirus (COVID-19), Social Distancing to Protect Vulnerable Adults and Shielding to Protect Extremely Vulnerable Adults [Internet]. 2020. Available from: https://www.bhiva.org/comment-from-BHIVA-and-THT-on-UK-Government-guidance-on-Coronavirus-COVID-19
- 5British HIV Association. COVID-19 & shielding: advice for HIV clinicians, G Ps and people living with HIV [Internet]. 2020. Available from: https://www.bhiva.org/COVID-19-and-shielding-advice-for-HIV-clinicians-G Ps-and-people-living-with-HIV
- 6British HIV Association. Shielding text messages sent in error to people living with HIV, response from the British HIV Association (BHIVA) and the Terrence Higgins Trust (THT) [Internet]. 2020 [cited 2020 May 11]. Available from: https://www.bhiva.org/shielding-text-messages-sent-in-error-to-people-living-with-HIV
- 7National Institute for Health and Care Excellence. Briefing notes for researchers - public involvement in NHS, health and social care research [Internet]. 2021 Apr. Available from: https://www.nihr.ac.uk/documents/briefing-notes-for-researchers-public-involvement-in-nhs-health-and-social-care-research/27371
- 8Positively UK [Internet]. 2019 [cited 2021 Nov 23]. Available from: https://positivelyuk.org/