Mycetoma-like cutaneous leishmaniasis
Beatriz Zimermano Coimbra, Ana Cláudia Cavalcante Espósito, Murilo de Oliveira Lima Carapeba, Marilda Aparecida Milanez Morgado de Abreu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1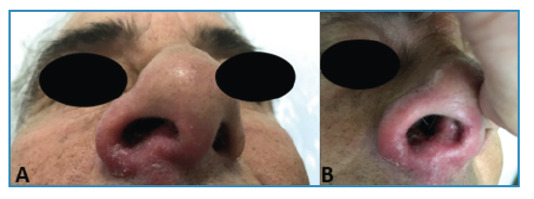 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsResearch on Leishmaniasis Studies · Beetle Biology and Toxicology Studies · Synthesis and biological activity
Cutaneous leishmaniasis is a protozoan disease caused by the bite of a sandfly that injects parasites into its host, with Leishmania (Viannia) braziliensis being Brazil's most common etiological agent1. Most patients manifest classical symptoms. However, there are atypical forms of this disease2 ^,^ 3. We report the case of a 53-year-old Brazilian man presenting with an inflammatory nodosity on the dorsum of the right foot causing pain, with local fluctuation and bloody discharge for 6 months (Figure 1A). Abscess and mycetoma hypotheses were raised and ciprofloxacin 500 mg was prescribed every 12 h for 14 days. One month later, the patient showed little improvement, and a biopsy of the lesion was performed. The histopathological examination was compatible with chronic abscessing dermatitis. Sulfamethoxazole and trimethoprim were prescribed; however, the patient was lost to follow-up. Two years later, the patient returned with erythema and infiltration in the right nostril (Figure 2A and B), and the lesion on the right foot persisted (Figure 1B). The diagnostic hypothesis was mucocutaneous leishmaniasis. Histopathological examination of a new biopsy specimen from the foot lesion revealed superficial deep granulomatous dermatitis. Despite normal laboratory test results and negative results for acid-fast bacilli, leishmania, and fungi in direct investigations, the diagnosis was confirmed using a positive indirect immunofluorescence test for leishmaniasis. Few reports of mycetoma-like leishmaniasis, as observed in this case, have been published in the literature. Glucantime was prescribed at two ampoules per day for 30 days, achieving total lesion regression without recurrence at the seven-month follow-up.
FIGURE 1:Dorsum of the right foot: A: Inflammatory nodosity (mycetoma-like aspect); B: Verrucous plaque after 2 years of evolution.
FIGURE 2: A and B: Erythematous infiltrative lesion in the right nostril.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Silveira FT What makes mucosal and anergic diffuse cutaneous leishmaniases so clinically and immunopathogically different? A review in Brazil Trans R Soc Trop Med Hyg 201929 trz 037trz 03710.1093/trstmh/trz 03731140559 · doi ↗ · pubmed ↗
- 2Elamin EM Guerbouj S Musa AM Guizani I Khalil EA Mukhtar MM Uncommon clinical presentations of cutaneous leishmaniasis in Sudan Trans R Soc Trop Med Hyg 200599118038081609900510.1016/j.trstmh.2005.04.009 · doi ↗ · pubmed ↗
- 3Bari AU Rahman SB Many faces of cutaneous leishmaniasis Indian J Dermatol Venereol Leprol 200874123271818781810.4103/0378-6323.38402 · doi ↗ · pubmed ↗