Pyomyositis in an immunocompetent man
Elcio Bakowski, Aline Serfaty, Eduardo Alexandrino Medeiros, Gláucia Zanetti, Edson Marchiori

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
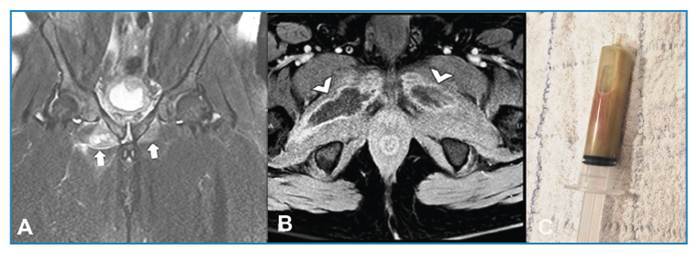 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Diseases and Tuberculosis · Musculoskeletal Disorders and Rehabilitation · Spinal Dysraphism and Malformations
A 44-year-old man presented with a history of severe pain in the right groin, particularly during abduction and external rotation of the lower limb, persisting for 2 days. No history of fever or trauma was reported. Blood tests revealed the following: white blood cell count, 18.2×10^3^/μL; C-reactive protein levels, 288 mg/L; and erythrocyte sedimentation rate, 128 mm/h. Magnetic resonance imaging (MRI) of the pelvis revealed fluid collection and diffuse edema in the external obturator muscles (Figures 1A and 1B). Blood culture revealed oxacillin-sensitive Staphylococcus aureus. Percutaneous computed tomography-guided drainage of the collections yielded purulent material. The culture results confirmed S. aureus infection (Figure 1C), substantiating the diagnosis of pyomyositis. Targeted antibiotic therapy was commenced.
FIGURE 1: (A) Coronal fat-suppressed T2-weighted magnetic resonance imaging (MRI) of the pelvis demonstrating diffuse muscle edema in the bilateral external obturator muscles (arrows). (B) Axial fat-suppressed post-contrast T1-weighted MRI showing fluid collections in the muscle bellies, with bilateral peripheral enhancement (arrowheads). (C) Aspirated purulent material obtained during CT-guided percutaneous drainage, confirming the diagnosis of pyomyositis caused by oxacillin-sensitive Staphylococcus.
Pyomyositis, a bacterial infection of the skeletal muscle, is characterized by the presence of localized pain, swelling, fever, and occasional abscess formation in advanced stages. Often referred to as “tropical pyomyositis,” pyomyositis is more prevalent in tropical regions; however, it has been observed increasingly in temperate climates, particularly in association with immunocompromised status, diabetes mellitus, recent trauma, and bacterial infections. Imaging plays a crucial role in the diagnosis and management of pyomyositis. MRI, which can reveal diffuse muscle edema with high signal intensity on T2-weighted images and contrast enhancement in the early stages1 ^,^ 2, is the preferred imaging modality. This report highlights the rarity of pyomyositis in immunocompetent patients without typical risk factors, underscoring the importance of early diagnosis using MRI, timely CT-guided drainage, and targeted antibiotic therapy to achieve favorable outcomes, even in non-tropical regions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wasserman PL Way A Baig S Gopireddy DR MRI of myositis and other urgent muscle-related disorders Emerg Radiol 202128240942110.1007/s 10140-020-01866-233169179 PMC 7652376 · doi ↗ · pubmed ↗
- 2Corin N Bennet S Hill J Thomas S Magnetic resonance imaging in the evaluation of suspected hip sepsis in children J Child Orthop 202216540941510.1177/1863252122112692236238140 PMC 9551002 · doi ↗ · pubmed ↗