Mycotic Aneurysm of the Superior Mesenteric Artery due to Infective Endocarditis
Elif Gündoğdu, Mustafa Kürşat Topal

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
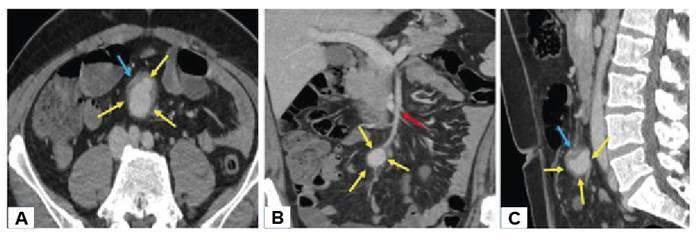 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Aortic and Vascular Conditions · Abdominal vascular conditions and treatments · Vascular Procedures and Complications
A 45-year-old male patient presented to the emergency department with a 1-month history of cough, fever, chills, sweating, and, recently, general malaise and fatigue. The patient's medical history included hypertrophic cardiomyopathy. The patient’s vital signs were within normal limits. Laboratory tests revealed leukocytosis (30.71×10³ uL) and elevated levels of C-reactive protein (99.1 mg/L), procalcitonin (12.60 ng/mL), and Troponin T (0.055 ng/mL). Echocardiography revealed a 42×18 mm vegetation originating from the mitral valve. Blood cultures revealed Streptococcus oralis. The patient was diagnosed with infective endocarditis and underwent mitral valve replacement. On the 15th postoperative day, the patient complained of periumbilical pain and abdominal computed tomography (CT) was performed. The CT scan showed an aneurysm approximately 3 cm in diameter distal to the superior mesenteric artery, with surrounding inflammatory soft tissue densities and fat tissue stranding (Figure 1). Mycotic aneurysms (MAs) are balloon-like dilatations of the arterial wall due to infection, usually bacterial1. MAs are associated with high mortality rates due to their increased risk of rupture and embolus production. CT is the modality of choice for detection. MAs appear on CT as lobulated vascular masses with an indistinct, irregular arterial wall and perivascular soft tissue inflammation and edema2. The noninvasive and rapid nature of CT allows for early diagnosis and intervention, significantly increasing the patient's chances of survival.
FIGURE 1:Axial (A), coronal (B), and sagittal (C) plane abdomen CT shows aneurysm (yellow arrows) of the superior mesenteric artery (red yellow) and perivascular fat stranding and inflammatory soft tissue (blue arrows).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pérez Baztarrica G Cherjovsky R Blanco N Porcile R Mycotic axillary artery aneurysm Rev Esp Cardiol 20096244514521940113210.1016/s 1885-5857(09)71674-3 · doi ↗ · pubmed ↗
- 2Zhang N Xiong W Li Y Mao Q Xu S Zhu J Sun Z Sun L Imaging features of mycotic aortic aneurysms Quant Imaging Med Surg 2021116286128783407974710.21037/qims-20-941PMC 8107294 · doi ↗ · pubmed ↗