Seminal Vesicle Atrophy and Ejaculatory Dysfunction Secondary to Prostatic and Seminal Vesicle Abscesses
Shinya Miyazaki, Takashi Ueda, Masashi Tsujimoto, Jintetsu Soh, Osamu Ukimura

TL;DR
This paper reports a rare case where prostate and seminal vesicle abscesses led to seminal vesicle atrophy and ejaculatory dysfunction.
Contribution
The study presents a novel clinical case linking abscesses to ejaculatory dysfunction and seminal vesicle atrophy.
Findings
A 56-year-old man developed ejaculatory dysfunction after conservative treatment for abscesses.
MRI showed severe seminal vesicle atrophy following the infection.
Treatments like tadalafil and testosterone therapy failed to improve symptoms.
Abstract
Seminal vesicle (SV) and prostatic abscesses are rare urological infections. However, their effect on sexual function remains unknown. In the present study, we encountered a case of SV atrophy and ejaculatory dysfunction (EjD) after conservative treatment. The patient was a 56-year-old man with fever who complained of pain during urination. He was diagnosed with SV and prostate abscesses and treated conservatively with antibiotics. One month after treatment, an EjD was observed, and magnetic resonance imaging revealed severe atrophy of the SV. Although various treatments for these symptoms, such as tadalafil and testosterone replacement therapy, were administered, the symptoms did not improve. Here, we report a case of EjD associated with SV and prostate abscesses. Factors leading to SV atrophy are unknown; however, complications should be noted.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
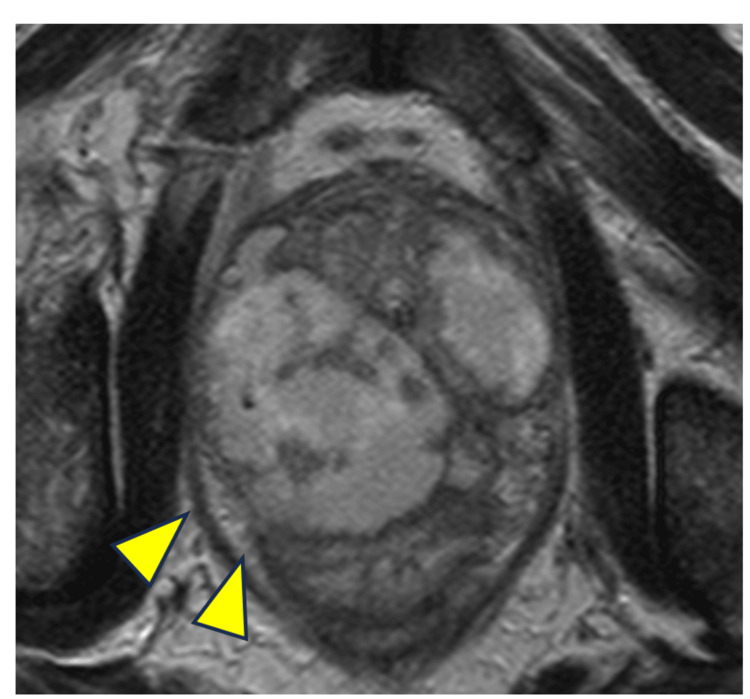 Figure 1
Figure 1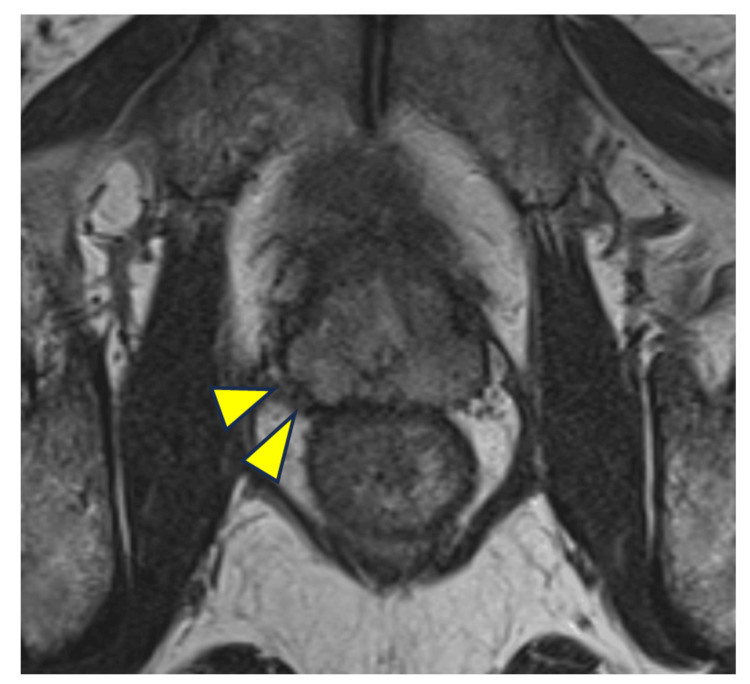 Figure 2
Figure 2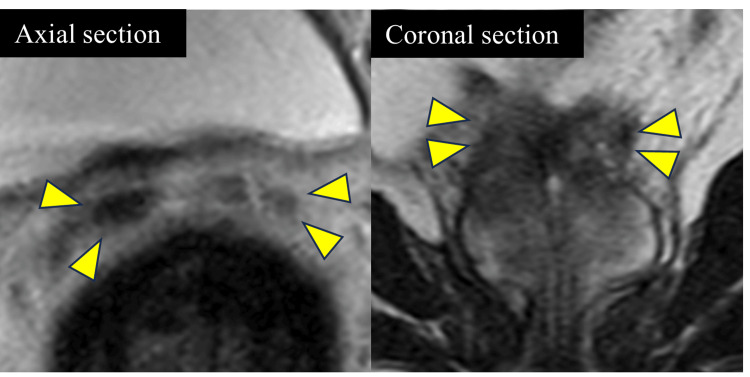 Figure 3
Figure 3| Test | Measured value | Normal range |
| White blood cell | 5500/μL | 3300-8600/μL |
| Red blood cell | 479 × 104/μL | 435-555 × 104/μL |
| Hemoglobin | 15.4 g/dL | 13.7-16.8 g/dL |
| Platelet | 19.9 × 104/μL | 15.8-34.8 × 104/μL |
| C-reactive protein | 0.02 mg/dL | < 0.14 mg/dL |
| Prostate-specific antigen | 0.394 ng/mL | < 4 ng/mL |
| Luteinizing hormone | 1.67 mIU/mL | 0.79-5.72 mIU/mL |
| Follicle-stimulating hormone | 10.8 mIU/mL | 2-8.3 mIU/mL |
| Total testosterone | 4.11 ng/mL | 1.31-8.71 ng/mL |
| Free testosterone | 7.8 pg/mL | 4.6-19.6 pg/mL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrologic and reproductive health conditions · Genital Health and Disease · Urological Disorders and Treatments
Introduction
Seminal vesicle (SV) and prostatic abscesses are rare. Although the SV and prostate are highly involved in sexual function, little is known about the sexual dysfunction caused by these infectious diseases. The symptoms of these diseases include fever, dysuria, perineal pain, and other nonspecific symptoms [1,2]. There are several treatment options, including long-term conservative treatment with antibiotics and various methods of drainage, such as transperineal, transurethral, and transrectal [3,4], but no standardized treatment exists. Herein, we describe a case of SV atrophy and ejaculatory dysfunction (EjD) secondary to conservative therapy. No similar case reports were listed on PubMed as of April 4, 2025, using the search terms prostate, SV, and EjD. To the best of our knowledge, this case is believed to be the first reported case of SV atrophy and EjD following SV and prostatic abscesses.
Case presentation
A 56-year-old man visited a local clinic with fever and pain during urination. The patient was diagnosed with acute prostatitis based on an elevated inflammatory response and tenderness on rectal examination, and antibiotic therapy was initiated. There was no history of diabetes or any other special notes in the patient's medical history. First-line antibiotics did not improve inflammation, and magnetic resonance imaging (MRI) revealed an abscess involving the prostate and SVs (Figure 1). The type of antibiotic was changed, and the inflammation improved. Approximately one month after the end of treatment, EjD was observed, and the patient was referred to our hospital. The patient had an Aging Males' Symptoms score of 27 and an International Index of Erectile Function of 5 out of 10. Blood samples showed a negative inflammatory response and a mild decrease in the free testosterone level to 7.8 pg/mL (Table 1).
MRI of swollen prostate and seminal vesicles prior to initiation of treatmentThe prostate and bilateral seminal vesicles were markedly swollen, a finding that was suspicious for fluid collection in the arrowheads area.
MRI showed improvement in fluid collection in the prostate and SV, as well as severe atrophy of the SV (Figures 2-3). The patient complained of an inability to have an orgasm. Amoxapine and testosterone replacement therapy were administered to rule out retrograde ejaculation and erectile dysfunction; however, only improvement in erectile dysfunction was observed, and no improvement in EjD was achieved. Tadalafil and vitamin B did not improve the EjD. The patient was unable to have an orgasm, and no post-ejaculation urinalysis was performed. The patient was diagnosed with EjD other than retrograde ejaculation or psychogenic and classified as emissionless due to SV atrophy based on his medical history. However, the possibility could not be ruled out that it was EjD due to ejaculatory duct obstruction since the patient did not want to undergo an invasive contrast examination of the vas deferens. The patient did not wish to have children; therefore, the treatment was terminated, and the patient was followed up.
Prostate on MRI after conservative treatmentProstatic and bilateral seminal vesicle swellings improved and fluid collection almost disappeared (arrowheads).
Atrophied seminal vesicles on MRI after conservative treatmentNo high-signal areas were observed within the bilateral seminal vesicles (indicated by arrowheads). The findings were suggestive of seminal vesicle atrophy and decreased seminal fluid.
Discussion
We encountered a case of SV atrophy and EjD secondary to the conservative treatment of SV and prostatic abscesses.
SV and prostatic abscesses are rare. Prostatic abscesses were reported to account for 0.5-2.5% of prostate disease, with an estimated incidence of 0.2-0.5% [5,6]. Since the prostate and SV are close, there have been reports of cases in which acute bacterial prostatitis spilled over to the SV and formed an abscess simultaneously, as in this case [7].
There is no standard treatment for SV or prostatic abscesses. Ludwig et al. reported the criteria for the treatment of prostatic abscesses with antibiotics alone to be within 1 cm in diameter [8]. If conservative treatment is not successful, transperineal, transrectal, or transurethral drainage may be performed with antibiotics [3,4]. In this case, the inflammatory response was relieved without drainage by antibiotics administered by the previous physician.
To the best of our knowledge, there are no reported cases of EjD with SV atrophy after an abscess. The SV is involved in semen production, and the vas deferens is a part of the seminal tract. The vas deferens also orifices into the prostate urethra. These factors may explain why SV and prostate abscesses can cause EjD. In the present case, because the patient was not aware of the orgasm, SV atrophy was considered the main cause of EjD. However, the patient did not want to undergo an invasive close examination, and the presence of obstruction to the passage of the vas deferens could not be evaluated. Therefore, we could not rule out the possibility that the patient had a coexisting ejaculatory duct obstruction due to inflammation. Because SV atrophy occurred after only one month, it was thought to be SV infarction associated with inflammation, although MRI could not point to any pelvic perfusion abnormality such as the SV artery. Because tadalafil has been reported to improve vascular endothelial function [9], the patient was administered tadalafil to improve blood flow; however, this did not lead to improvement. Amoxapine, a tricyclic antidepressant similar to imipramine, which has been reported to be effective for retrograde ejaculation [10], and testosterone replacement therapy were also administered concurrently to exclude the possibility of retrograde ejaculation or erectile dysfunction due to late-onset hypogonadism syndrome but were ineffective.
It is unclear whether conservative treatment led to SV atrophy, and more knowledge is required. In addition, treatment should be performed considering the possibility of SV atrophy, a secondary complication of SV abscesses that can cause ejaculation problems. Aggressive drainage may be considered for early inflammatory control, especially in young sexually active patients.
Conclusions
Here, we report a case of SV atrophy and EjD associated with SV and a prostatic abscess. Although the factors leading to atrophy are unknown, early aggressive treatment should be considered, taking into account the presence of sexual activity and the hope of “raising a child,” since the abscess may affect sexual function. Post-treatment follow-up regarding complications such as this may also be important.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diagnosis and treatment of patients with prostatic abscess in the post-antibiotic era Int J Urol Ackerman AL Parameshwar PS Anger JT 1031102520182894450910.1111/iju.13451 · doi ↗ · pubmed ↗
- 2An unusual groin mass. Seminal vesicle abscess: a case report Cases J Saha S Wright G Arulampalam T Corr J 6531220091982981910.1186/1757-1626-2-6531 PMC 2740224 · doi ↗ · pubmed ↗
- 3Transrectal ultrasound-guided transperineal and transrectal management of seminal vesicle abscesses Eur J Radiol Sağlam M Uğurel S Kilciler M Taşar M Somuncu I Uçöz T 3293345220041564371910.1016/j.ejrad.2003.11.006 · doi ↗ · pubmed ↗
- 4Seminal vesicle abscess after vasectomy: evaluation by transrectal sonography and CTAJR Am J Roentgenol Zagoria RJ Papanicolaou N Pfister RC Stafford SA Young HH 2nd 1371381491987329670810.2214/ajr.149.1.137 · doi ↗ · pubmed ↗
- 5Prostatic abscess: diagnosis and treatment J. Urol Granados EA Riley G Salvador J Vincente J 80821481992161388710.1016/s 0022-5347(17)36516-3 · doi ↗ · pubmed ↗
- 6The value of transrectal ultrasound guided needle aspiration in treatment of prostatic abscess Eur J Radiol Gogus C Ozden E Karaboga R Yagci C 94985220041538085210.1016/S 0720-048X(03)00231-6 · doi ↗ · pubmed ↗
- 7Extensive prostatic abscess drained by CT-guided percutaneous approach: case report Radiol Case Rep Lahfidi A Traore WM Andour H Abdellaoui M Fenni JE Saouab R 272327271720223566922610.1016/j.radcr.2022.04.049PMC 9166371 · doi ↗ · pubmed ↗
- 8Diagnosis and therapeutic management of 18 patients with prostatic abscess Urology Ludwig M Schroeder-Printzen I Schiefer HG Weidner W 340345531999993305110.1016/s 0090-4295(98)00503-2 · doi ↗ · pubmed ↗