Timing of postoperative chemotherapy and prognosis in neoadjuvant-treated gastric cancer patients: a multicenter real-world cohort study
Hua-Long Zheng, Ling-Kang Zhang, Hong-Hong Zheng, Chen-Bin Lv, Bin-Bin Xu, Guang-Tan Lin, Qi-Yue Chen, Jian-Xian Lin, Chao-Hui Zheng, Chang-Ming Huang, Jian-Wei Xie

TL;DR
Starting chemotherapy 6-8 weeks after surgery improves survival and delays cancer recurrence in patients with advanced gastric cancer who had pre-surgery treatment.
Contribution
Identifies a 6-8 week optimal window for postoperative chemotherapy in neoadjuvant-treated gastric cancer patients.
Findings
Patients with 6-8 week TTC had significantly lower 3-year mortality rates compared to other groups.
Shorter or longer TTC intervals were linked to higher risks of cancer-specific and all-cause mortality.
The 6-8 week TTC group experienced delayed cancer recurrence compared to other timing groups.
Abstract
The optimal time to chemotherapy (TTC) in locally advanced gastric cancer (LAGC) patients treated with neoadjuvant chemotherapy (NLAGC) remains unclear. Consecutive 524 patients with NLAGC between Jan. 2010 and Dec. 2022 were identified. Patients were categorized into three groups: TTC < 6w, 6w ≤ TTC ≤ 8w, and TTC > 8w. Survival analysis was conducted using the Cox proportional hazards model to assess the impact of TTC on gastric cancer-specific mortality (GCSM) and all-cause mortality (ACM). Cumulative competing risk curves were employed to evaluate the incidence of competing events. Overall, 451 patients were included.Cumulative competing risk curves showed that the 3-year ACM and GCSM were significantly lower in the 6w ≤ TTC ≤ 8w group (ACM: 19.7% vs. 37.2% vs. 39.7%, GCSM: 19.7% vs. 35.2% vs. 38.8%) compared to the TTC < 6w and TTC > 8w groups. Compared to patients with 6w ≤ TTC ≤…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
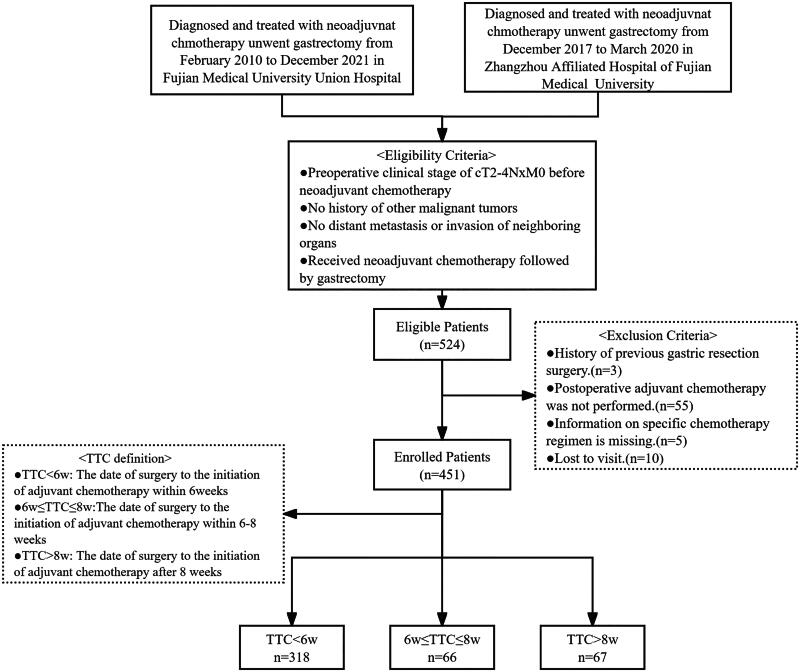 Figure 1
Figure 1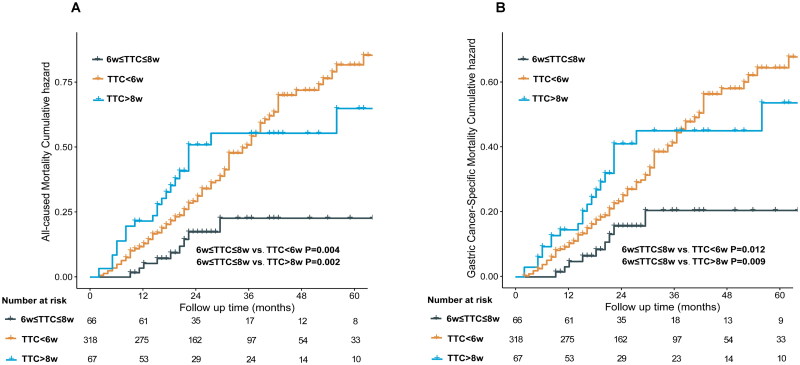 Figure 2
Figure 2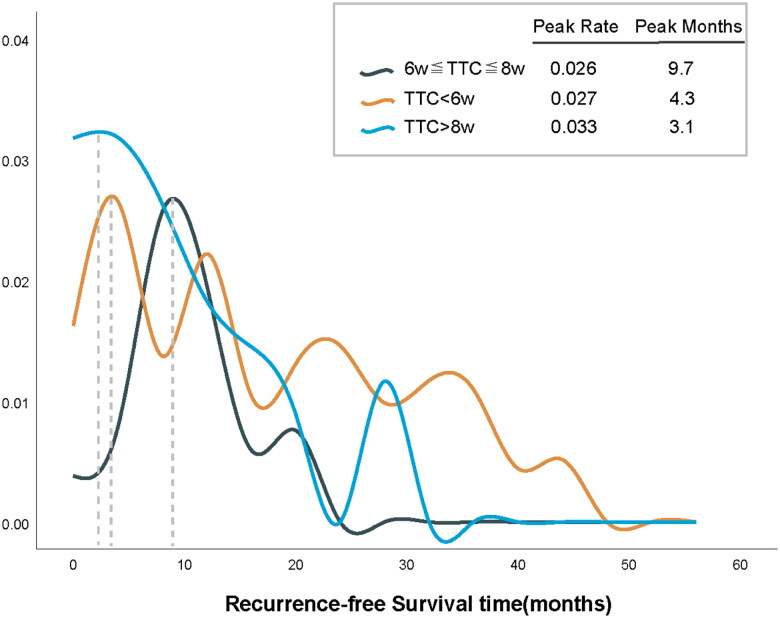 Figure 3
Figure 3| Characteristic | TTCs | p-Valuea | ||
|---|---|---|---|---|
| TTC < 6w | 6w ≤ TTC ≤ 8w | TTC > 8w | ||
| Age, n (%) |
| |||
| <65 | 190 (59.7) | 27 (40.9) | 38 (56.7) | |
| ≥65 | 128 (40.3) | 39 (59.1) | 29 (43.3) | |
| Sex, n (%) | 0.093 | |||
| Male | 234 (73.6) | 50 (75.8) | 41 (61.2) | |
| Female | 84 (26.4) | 16 (24.2) | 26 (38.8) | |
| BMI, n (%) | 0.093 | |||
| <25 kg/m2 | 263 (82.7) | 47 (71.2) | 55 (82.1) | |
| ≥25 kg/m2 | 55 (17.3) | 19 (28.8) | 12 (17.9) | |
| ASA, n (%) | 0.815 | |||
| 1 | 46 (14.5) | 7 (10.6) | 10 (14.9) | |
| 2 | 227 (71.4) | 50 (75.8) | 45 (67.2) | |
| 3 | 45 (14.2) | 9 (13.6) | 12 (17.9) | |
| ypTNM stage, n (%) | 0.157 | |||
| ypCR/I | 60 (18.9) | 17 (25.8) | 12 (17.9) | |
| II | 106 (33.3) | 20 (30.3) | 14 (20.9) | |
| III | 152 (47.8) | 29 (43.9) | 41 (61.2) | |
| Location, n (%) | 0.896 | |||
| Upper | 137 (43.1) | 30 (45.5) | 27 (40.3) | |
| Middle | 62 (19.5) | 13 (19.7) | 11 (16.4) | |
| Lower | 93 (29.2) | 20 (30.3) | 22 (32.8) | |
| Mixed | 26 (8.2) | 3 (4.5) | 7 (10.4) | |
| Tumor size, n (%) | 0.520 | |||
| <5 cm | 187 (58.8) | 35 (53) | 42 (62.7) | |
| ≥5 cm | 131 (41.2) | 31 (47) | 25 (37.3) | |
| TRG, n (%) | 0.352 | |||
| 0/1 | 76 (23.9) | 21 (31.8) | 15 (22.4) | |
| 2/3 | 242 (76.1) | 45 (68.2) | 52 (77.6) | |
| Lymphovascular invasion, n (%) | 0.567 | |||
| No | 191 (60.1) | 35 (53) | 40 (59.7) | |
| Yes | 127 (39.9) | 31 (47) | 27 (40.3) | |
| Neural invasion, n (%) | 0.248 | |||
| No | 160 (50.3) | 37 (56.1) | 28 (41.8) | |
| Yes | 158 (49.7) | 29 (43.9) | 28 (41.8) | |
| R status, | 0.292 | |||
| R0 | 286 (89.9) | 56 (84.8) | 57 (85.1) | |
| R1 | 32 (10.1) | 10 (15.2) | 10 (14.9) | |
| NACT cycles, median (IQR) | 4 (3–4) | 4 (3–4) | 3 (3–4) | 0.213 |
| AC cycles, median (IQR) | 4 (2–6) | 4 (3–6) | 3 (1–4) |
|
| AC, n (%) |
| |||
| <4 cycles | 113 (35.5) | 24 (36.4) | 36 (53.7) | |
| ≥4 cycles | 205 (64.5) | 42 (63.6) | 31 (46.3) | |
| Surgical outcomes | ||||
| Blood loss, median (IQR) | 50 (30–50) | 50 (30–60) | 50 (30–65) | 0.426 |
| The length of operation, median (IQR) | 184 (165–210) | 190 (160–230) | 180 (152–232) | 0.472 |
| Postoperative hospital stay, median (IQR) | 9 (7–12) | 8 (7–10) | 8 (7–12) | 0.054 |
| Complications, n (%) | 0.132 | |||
| No | 254 (79.9) | 46 (69.7) | 49 (73.1) | |
| Yes | 64 (20.1) | 20 (30.3) | 18 (26.9) | |
| Clavien-Dindo | 0.421 | |||
| I | 44 (68.8) | 15 (75) | 10 (55.6) | |
| ≥II | 20 (31.2) | 5 (25) | 8 (44.4) | |
| Characteristic | Univariate analysis | Multivariate analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95 CI | HR | 95 CI | |||
| Age | ||||||
| <65 | REF | |||||
| ≥65 | 0.988 | 0.714–1.369 | 0.944 | |||
| Sex | ||||||
| Male | REF | |||||
| Female | 1.106 | 0.780–1.569 | 0.572 | |||
| BMI | ||||||
| <25 kg/m2 | REF | |||||
| ≥25 kg/m2 | 0.903 | 0.588–1.388 | 0.642 | |||
| ASA | ||||||
| 1 | REF | REF | ||||
| 2 | 1.273 | 0.769–2.105 | 0.348 | 1.377 | 0.827–2.292 | 0.219 |
| 3 | 2.642 | 1.488–4.693 |
| 2.391 | 1.329–4.299 |
|
| ypStage | ||||||
| ypCR/I | REF | REF | ||||
| II | 1.371 | 0.717–2.622 | 0.340 | 1.061 | 0.527–2.134 | 0.869 |
| III | 3.587 | 2.016–6.383 |
| 2.747 | 1.409–5.358 |
|
| Tumor size | ||||||
| <5 cm | REF | REF | ||||
| ≥5 cm | 1.496 | 1.086–2.061 |
| 1.120 | 0.797–1.572 | 0.514 |
| Location | ||||||
| Upper | REF | |||||
| Middle | 1.052 | 0.671–1.650 | 0.824 | |||
| Lower | 1.067 | 0.725–1.570 | 0.742 | |||
| Mixed | 1.589 | 0927–2.727 | 0.092 | |||
| Lymphovascular invasion | ||||||
| No | REF | REF | ||||
| Yes | 1.564 | 1.113–2.159 |
| 1.107 | 0.769–1.594 | 0.585 |
| Neural invasion | ||||||
| No | REF | REF | ||||
| Yes | 1.446 | 1.045–2.002 |
| 0.998 | 0.690–1.442 | 0.990 |
| R status | ||||||
| Negative | REF | REF | ||||
| Positive | 1.617 | 1.017–2.571 |
| 1.147 | 0.712–1.849 | 0.573 |
| AC | ||||||
| <4 cycles | REF | REF | ||||
| ≥4 cycles | 0.713 | 0.515–0.985 |
| 0.641 | 0.455–0.904 |
|
| TTC | ||||||
| 6w ≤ TTC ≤ 8w | REF | REF | ||||
| TTC < 6w | 2.651 | 1.345–5.227 |
| 3.102 | 1.559–6.171 |
|
| TTC > 8w | 2.959 | 1.386–6.317 |
| 2.786 | 1.297–5.988 |
|
| TRG grade | ||||||
| 0/1 | REF | REF | ||||
| 2/3 | 2.149 | 1.355–3.409 |
| 1.315 | 0.776–2.227 | 0.309 |
| Complications | ||||||
| No | REF | |||||
| Yes | 1.307 | 0.919–1.859 | 0.137 | |||
| TTC (weeks) | Number of patients | Number of events | Model A | Model B | Model C | |||
|---|---|---|---|---|---|---|---|---|
| HR (95% CI) |
| HR (95% CI) |
| HR (95% CI) |
| |||
| Gastric cancer-specific mortality | ||||||||
| 6–8 | 66 | 9 | Ref. | Ref. | Ref. | |||
| <6 | 318 | 106 | 2.395 (1.204–4.766) |
| 2.591 (1.289–5.207) |
| 2.792 (1.382–5.641) |
|
| >8 | 67 | 24 | 2.552 (1.171–5.563) |
| 2.341 (1.020–5.376) |
| 2.343 (1.060–5.180) |
|
| All-cause mortality | ||||||||
| 6–8 | 66 | 9 | Ref. | Ref. | Ref. | |||
| <6 | 318 | 115 | 2.736 (1.380–5.425) |
| 2.913 (1.457–5.824) |
| 3.102 (1.545–6.230) |
|
| >8 | 67 | 26 | 3.004 (1.403–6.433) |
| 2.871 (1.326–6.215) |
| 2.719 (1.255–5.892) |
|
- —Fujian Provincial Medical ‘Building High-level Hospitals, High-level Clinical Medical Centers and Key Clinical Specialty Projects’
- —Fujian Provincial Health Technology Project10.13039/501100017686
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Gastrointestinal Tumor Research and Treatment · Metastasis and carcinoma case studies
Introduction
In 2020, more than 1 million new cases of gastric cancer (GC) were diagnosed globally, with ∼783,000 GC-related deaths, rendering it the fifth most common and fourth most lethal cancer worldwide [1,2]. Surgical resection remains the cornerstone of treatment for resectable gastric cancer; however, its efficacy as a monotherapy is limited [3]. The MAGIC trial in 2006 [4] was pivotal in demonstrating that perioperative chemotherapy combined with surgery significantly improved overall survival and progression-free survival compared to surgery alone. Similarly, in 2011, a phase III clinical trial conducted by Ychou et al. produced analogous findings [5]. Khrizman et al. [6] also highlighted that even in specialized cancer centers, a considerable proportion of patients undergoing neoadjuvant treatment with curative intent do not complete postoperative chemotherapy, underscoring the need for strategies to promote completion of this third and final stage of treatment following neoadjuvant chemotherapy and surgery. Consequently, the integration of perioperative chemotherapy with surgery has emerged as a novel therapeutic approach for Locally Advanced Gastric Cancer (LAGC) [7–10].
Previous studies have suggested that prolonged intervals between surgery and adjuvant chemotherapy may increase the risk of micrometastatic expansion. Delayed chemotherapy could hinder the early inhibition of angiogenesis in micrometastases and contribute to the development of initial drug resistance [11,12]. Additionally, animal models have shown that surgery may lead to an increase in circulating tumor cells, which could promote metastatic growth [13,14]. This process has been linked to reduced angiogenesis and elevated tumorigenic growth factors. Based on these findings, it has been proposed that excessive delays in adjuvant chemotherapy may negatively impact treatment outcomes. Previous studies on breast, colorectal, and pancreatic cancers have demonstrated a close association between the timing of adjuvant chemotherapy initiation and tumor prognosis [15–21]. Initiating postoperative chemotherapy within the appropriate time window can help reduce recurrence and improve survival rates. For instance, a meta-analysis revealed that patients with stage III colorectal cancer (CRC) should commence adjuvant chemotherapy within eight weeks postoperatively because initiating chemotherapy beyond this timeframe significantly diminishes overall survival [15]. Moreover, Gagliato et al. observed that in specific subsets of patients with breast cancer (those with stage III TNM, TNBC, and Her2-positive tumors), delayed chemotherapy [time to chemotherapy (TTC) > 61 days] was associated with poor prognosis [16]. Hence, the prompt administration of chemotherapy is recommended for high-risk patients. Furthermore, many researchers have focused on the impact of the initiation time of postoperative adjuvant chemotherapy on the prognosis of patients with directly operable gastric cancer [22–24]. Studies have found that delaying TTC beyond six weeks is significantly associated with an increased risk of local recurrence and mortality [25]. Huang et al. indicated that patients who commenced chemotherapy more than 8 weeks after surgery exhibited poorer long-term prognosis than those with TTC < 8 weeks (with respective 5-year overall survival rates of 56.6 and 40.2%, and corresponding 5-year recurrence-free survival rates of 57.6 and 46.4%) [26].
In recent years, significant progress has been made in neoadjuvant chemotherapy for locally advanced gastric cancer (LAGC), particularly in combination treatment strategies. For instance, a Phase II trial by Zhao et al. [27] demonstrated that camrelizumab (a PD-1 inhibitor) combined with mFOLFOX achieved a 9.1% pathological complete response (pCR) rate, with HER2 and CTNNB1 mutations potentially associated with treatment sensitivity. Additionally, multi-drug regimens, such as docetaxel, oxaliplatin, and S-1 (DOS), have shown promising efficacy in the JCOG1704 Phase II trial [28] and the Neo-REGATTA study [29], suggesting that successful neoadjuvant chemotherapy followed by radical surgery may improve patient outcomes. However, despite advances in perioperative chemotherapy regimens and the evolving role of neoadjuvant therapy, key postoperative treatment questions remain unresolved, including TTC and the ideal duration of adjuvant chemotherapy, both of which require further investigation.
With the widespread adoption of perioperative chemotherapy, many researchers have explored the TTC postoperatively in patients undergoing neoadjuvant chemotherapy (NACT) followed by curative surgery. Research indicates that irrespective of cancer type (breast, colorectal, or pancreatic) and NACT administration, the timing of chemotherapy initiation post-surgery significantly correlates with patient survival prognosis. Thong et al. found that CRC patients in the non-delayed group at 23 (proposed) and 25 (median) weeks’ cutoff reported better 5-year disease-free survival (DFS) compared to those in the delayed group by 4.1 and 0.8%, respectively. Conversely, at a cutoff of 28 (mean) weeks, the delayed group exhibited better DFS by 4.4% [30]. After investigating the time to initiation of postoperative radiotherapy (PORT) in breast cancer patients receiving neoadjuvant chemotherapy, Saulo et al. discovered that receiving PORT at 8 weeks postoperatively was associated with superior disease-free survival (DFS) (<8 vs. 8–16 weeks: HR 0.33; 95% CI 0.13–0.81; p = 0.02; <8 vs. >16 weeks: HR 0.38; 95% CI 0.15–0.96; p = 0.04) and overall survival (OS) (<8 vs. 8–16 weeks: HR 0.22; 95% CI 0.05–0.90; p = 0.036; <8 vs. >16 weeks: HR 0.28; 95% CI 0.07–1.15; p = 0.08). They concluded that early initiation of PORT is imperative [31].
With the advancements in perioperative treatment for gastric cancer, there has been a steady rise in the number of patients with LAGC undergoing NACT. These patients can benefit from multidisciplinary treatment approaches, including chemotherapy, radiotherapy, and targeted therapy, which have the potential to improve prognosis and enhance the success rate of surgical resection and long-term survival [32,33]. However, there is currently a paucity of research exploring the optimal timing for initiating postoperative chemotherapy in patients with LAGC who have undergone NACT followed by gastrectomy. Thus, this study aims to utilize real-world multicenter data to elucidate the impact of various postoperative chemotherapy initiation times on the prognosis of patients with NLAGC. The objective of this study is to provide clinical practitioners with valuable insights to aid in treatment decision-making.
Materials and methods
Patient population
This retrospective study analyzed the clinicopathological data of 524 LAGC patients who underwent D2 radical gastrectomy following NACT between January 2010 and December 2021 at two centers: Fujian Medical University Union Hospital (FJMUUH) and Zhangzhou Affiliated Hospital of Fujian Medical University (ZAHFMU). Patients were selected based on the following criteria: (1) Diagnosis of locally advanced gastric cancer with a clinical stage of cT2–T4, N×, M0 before neoadjuvant chemotherapy; (2) No coexisting or previous malignancies; (3) Absence of distant metastasis or direct invasion into adjacent organs confirmed by imaging and clinical evaluation; (4) Completion of gastrectomy following neoadjuvant chemotherapy. Exclusion criteria included: (1) Previous history of gastric resection; (2) Recent (<3 months) cardiovascular events, including cerebrovascular or coronary artery disease; (3) Undergoing emergency surgical intervention; (4) Failure to receive adjuvant chemotherapy postoperatively; (5) Incomplete data on chemotherapy regimen; (6) Inadequate follow-up information or loss to follow-up. The relevant inclusion and exclusion criteria have been described in our previous studies conducted [34,35]. After applying the exclusion criteria, 451 patients were included in this study. A flowchart depicting this process is shown in Figure 1.
Flow chart of the charge and arrangement standard.
Due to the long study period, chemotherapy regimens evolved with advancements in clinical guidelines and the needs for individualized treatment. Supplemental Figure 5 presents a comparison of chemotherapy regimen differences across different time periods, and the results show that: 2010–2013y: Platinum-based regimens (78.8%) (e.g. ECF and XELOX) were predominant. 2014–2017y: While platinum-based regimens (62.0%) remained widely used, the proportion of paclitaxel-based regimens (3.8→15.5%) and other regimens (17.3→22.5%) gradually increased. 2018–2022y: The proportion of paclitaxel-based regimens and other regimens further increased (21.1→38→71%).
This study was conducted in accordance with the ethical principles outlined in the World Medical Association’s Declaration of Helsinki. Informed consent was obtained from all patients and their legal guardians. The study protocol was approved by the Ethics Board of both hospitals (2024KY039), and written informed consent was obtained from all participants.
Treatments
In this study, all patients received neoadjuvant chemotherapy (NACT) centered on fluorouracil-based regimens. The most commonly combined agents included platinum compounds (cisplatin, oxaliplatin, or loplatin) and taxanes (paclitaxel or docetaxel). Postoperative adjuvant chemotherapy (AC) was routinely recommended, comprising three general categories: (1) platinum-based regimens (e.g. platinum plus capecitabine, S-1, or 5-FU); (2) taxane-based combinations (e.g. paclitaxel with capecitabine, S-1, or 5-FU); (3) other regimens, such as paclitaxel-platinum or single-agent S-1. Standardized regimens included SOX/XELOX protocols, administered as two preoperative and six postoperative cycles at 3-week intervals. In these regimens, S-1 (40–60 mg/m^2^) or capecitabine (1000 mg/m^2^, twice daily, days 1–14) was combined with oxaliplatin (130 mg/m^2^, day 1). Alternatively, FOLFOX4 was used in three preoperative and six postoperative cycles every 2 weeks, consisting of oxaliplatin (85 mg/m^2^, day 1), folinic acid (200 mg/m^2^, 2-h infusion), followed by a bolus of fluorouracil (400 mg/m^2^) and a 22-h continuous infusion of fluorouracil (600 mg/m^2^). The chemotherapy regimens and doses aforementioned have been previously documented [34,36]. Paclitaxel regimens, platinum-based regimens, and other regimens were evenly distributed across the entire patient cohort (39.9 vs. 39.9 vs. 20.2%) (see Supplemental Figure 1A). All perioperative chemotherapy regimens and doses were tailored based on tumor response and chemotherapy toxicity.
The surgical procedure entailed gastrectomy with D2 lymph node dissection, the extent of which was determined in accordance with the Japanese gastric cancer treatment guidelines 2021 (version 6th) [7]. The R status was evaluated through intraoperative frozen section analysis of surgical margins and postoperative pathological reports [34].
Data collection
Clinical, pathological, and follow-up information were retrospectively extracted from the Gastric Cancer Databases maintained by two tertiary medical centers in China. The dataset included demographic parameters, such as sex, age at diagnosis, body mass index (BMI), and American Society of Anesthesiologists (ASA) physical status classification. Tumor-related and perioperative variables were also collected, including tumor size and location, pathological ypTNM stage, resection margin status (R0/R1), presence of lymphovascular and perineural invasion, surgical duration, intraoperative blood loss, occurrence of postoperative complications, and hospital length of stay. In addition, we retrieved treatment-specific data, such as the number and regimen of neoadjuvant chemotherapy (NACT) cycles, whether postoperative adjuvant chemotherapy (AC) was initiated, total AC cycles, and the corresponding regimens administered. These variables were selected based on prior studies linking them to long-term outcomes in patients undergoing perioperative treatment for gastric cancer.
Definition and patient groups
TTC was defined as the interval from the date of surgery to the initiation of adjuvant chemotherapy (see Supplemental Figure 2). According to the 6th edition of the Japanese Gastric Cancer Treatment Guidelines (updated in 2021) [7], it is clearly recommended that postoperative chemotherapy should be initiated within 6 weeks to achieve optimal efficacy. Additionally, several high-quality studies [15,18] have shown that starting chemotherapy within 8 weeks postoperatively significantly improves survival rates, while starting chemotherapy after 8 weeks is associated with poorer prognosis. These studies provide scientific evidence for using 8 weeks as the upper boundary. Furthermore, studies on other cancers [16] have also indicated that the 6–8 week period is a critical timeframe for initiating chemotherapy. Thus, based on the TTC, patients were divided into three groups: within 6 weeks (TTC < 6w), within 6–8 weeks (6w ≤ TTC ≤ 8w), and after 8 weeks (TTC > 8w).
Primary outcomes were GCSM (death due to gastric cancer, with censoring of other causes of death and survivors) and all-cause mortality (ACM) (death from any cause, with censoring of survivors). Recurrence-free survival (RFS) was defined as the time from the end of surgery to the first recorded instance of cancer recurrence, metastasis, or occurrence of a new cancer.
The tumor regression grade (TRG), representing the histopathological response to neoadjuvant chemotherapy, was evaluated based on the criteria outlined in the 8th edition of the AJCC Cancer Staging Manual. Similarly, the post-treatment T (tumor) and N (lymph node) stages were determined according to the AJCC 8th edition TNM classification system [37].
Follow-up
Postoperative follow-up was conducted at regular intervals: every three months during the first two years and biannually thereafter until five years post-surgery. The routine surveillance protocol included periodic physical assessments, hematologic testing, and cross-sectional imaging (chest X-ray and abdominal CT scans) every six months for the initial three years. In addition, annual upper gastrointestinal endoscopy was performed for up to three years postoperatively. PET/CT was selectively employed in cases where tumor recurrence was clinically suspected [35,36,38].
Statistical analysis
Correlation analysis was performed using SPSS version 25 (IBM, Armonk, NY, USA) and R version 4.3.3 (http://www.r-project.org). Continuous variables were expressed as mean ± standard deviation (SD) if normally distributed; otherwise, they were represented as median (interquartile range, IQR). The chi-square test or Fisher’s exact test was used to analyze categorical variables, presented as percentages. Kernel density curves assessed the peak recurrence time across different TTC groups. The Cox proportional hazards model was employed to identify independent risk factors associated with the patient’s long-term prognosis, with all variables from the univariate analysis with p < 0.05 included in the multivariate analysis. Competing risk models (Fine and Gray) were employed to account for the potential impact of competing events, such as recurrence and death from other causes, on survival outcomes. This model was used to assess the cumulative incidence of gastric cancer-specific mortality (GCSM) and all-cause mortality (ACM) while adjusting for key confounding factors. By incorporating this approach, we ensured that the influence of competing events on the relationship between chemotherapy timing and survival outcomes was appropriately controlled [39]. Cox regression analysis assessed hazard ratios (HRs) and 95% confidence intervals (CIs) for ACM and GCSM.
Results
Baseline characteristics
Table 1 presents the baseline characteristics of three groups of patients: TTC < 6 weeks, 6w ≤ TTC ≤ 8w, and TTC > 8 weeks, with 451 patients included. TTC < 6w comprises 318 cases (70.5%), while 66 cases (14.7%) fall within the range of 6w ≤ TTC ≤ 8w, and 67 cases (14.8%) exceed TTC > 8w. In the comparison of baseline data across the three groups, statistically significant differences were observed only in age and postoperative AC Cycles. No significant statistical differences were observed in Sex, BMI, ASA classification, ypTNM stage, tumor location, tumor size, TRG grade, lymphovascular invasion, neural invasion, R status, number of neoadjuvant chemotherapy cycles. In addition, we found that there were no significant statistical differences among the groups regarding postoperative recovery: the results showed no notable differences in postoperative hospital stay, postoperative complications (yes or no), or Clavien–Dindo classification (All p > 0.05).
In the different TTC subgroups, the distribution of chemotherapy regimens showed relatively consistent patterns [6w ≤ TTC ≤ 8w: Platinum-based regimens: 26 (33.3%); Paclitaxel regimens: 29 (37.2%); Other regimens: 11 (14.1%). TTC < 6w: Platinum-based regimens: 121 (38.4%); Paclitaxel regimens: 129 (41.0%); Other regimens: 68 (21.6%). TTC > 8w: Platinum-based regimens: 33 (46.5%); Paclitaxel regimens: 22 (31.0%); Other regimens: 12 (16.9%)] (see Supplemental Figure 1B). In terms of chemotherapy cycles, 4 cycles dominated both neoadjuvant and postoperative adjuvant chemotherapy, accounting for 40.1 and 22.8%, respectively. Neoadjuvant chemotherapy patients were more concentrated in 3–4 cycles, while postoperative adjuvant chemotherapy showed a more even distribution, with relatively more patients concentrated in 4 cycles. Overall, 4 cycles of chemotherapy were the most common in both treatment phases (see Supplemental Figure 3).
Supplemental Table 1 shows the intergroup distribution of variables across different chemotherapy regimens and chemotherapy initiation times (TTC < 6w, 6w ≤ TTC ≤ 8w, TTC > 8w). The results indicated that the overall distribution of variables was relatively balanced between the groups, with most variables showing no significant differences in p-values across the groups. Patients with different chemotherapy regimens and initiation times were generally similar in baseline characteristics. Additionally, except for the p-value for age in the Other regimens group (0.04), no statistically significant differences were observed in the variables for the Platinum-based regimens and Paclitaxel regimens groups, indicating a generally homogeneous distribution of characteristics between the groups.
There were no significant differences in the incidence of chemotherapy-related adverse events among the different TTC groups (p = 0.978). The most commonly observed adverse events across all groups included leukopenia, hypoalbuminemia, electrolyte disturbances, fever, diarrhea, abnormal liver function, myelosuppression, allergy, vomiting, peripheral neuropathy, palpitations, thrombocytopenia, and neutropenia. The incidence of adverse events was comparable among the groups, with no statistically significant differences (Supplemental Table 6).
Survival outcomes and mortality risk
The median follow-up time for patients in this retrospective cohort study was 44.5 months. During this follow-up period, 150 deaths were observed, of which 139 were attributed to gastric cancer-related deaths. Cumulative competing risk curve analysis revealed that patients in the 6w ≤ TTC ≤ 8w group exhibited significantly lower 3-year ACM compared to the TTC < 6w group and the TTC > 8w group (3-year ACM: 19.7 vs. 37.2 vs. 39.7%, p = 0.009) (see Figure 2A). Regarding GCSM, patients in the 6w ≤ TTC ≤ 8w group showed significantly lower 3-year GCSM compared to the TTC < 6w group and the TTC > 8w group (3-year GCSM: 19.7 vs. 35.2 vs. 38.8%, p = 0.019) (see Figure 2B).
All-cause mortality (A) and gastric-cancer specific mortality (B) associated competitive risk assessed by TTC in this study population.
Further evaluation using the Cox regression model to assess independent prognostic factors associated with patient ACM, recurrence-free survival (RFS), and GCSM revealed that the American Society of Anesthesiologists (ASA) classification, ypTNM stage, tumor size, lymphovascular/neural invasion, TTC, and tumor regression grade (TRG) were prognostic factors for ACM in the univariate analysis. Upon inclusion of significant indicators (p < 0.05) from the univariate analysis into the multivariate analysis using the Cox regression model, it was found that ASA (ASA 3: HR: 2.391, 95% CI [1.329–4.299], p = 0.004), ypTNM stage (ypIII: HR: 2.747, 95% CI [1.409–5.358], p = 0.003), AC (AC (yes): HR: 0.641, 95% CI [0.455–0.904]), and TTC (TTC < 6w: HR: 3.102, 95% CI [1.559–6.171], p = 0.001; TTC > 8w: HR: 2.786, 95% CI [1.297–5.988], p = 0.009) were identified as independent prognostic risk factors for ACM (see Table 2). The same results were observed in the correlation analysis between GCSM and RFS (see Supplemental Tables 2 and 3).
TTC and adjusted models
Upon adjusting for demographic and preoperative characteristics (Model A), patients with TTC < 6w exhibited a 2.395-fold increased risk of GCSM (95% CI [1.204–4.766], p = 0.011) and a 2.736-fold increased risk of ACM (95% CI [1.380–5.425], p = 0.004) compared to those with 6w ≤ TTC ≤ 8w. Further adjustment for clinical factors and treatment modalities (Model C) strengthened and sustained the association between TTC < 6w and increased risk of GCSM and ACM relative to 6w ≤ TTC ≤ 8w (GCSM: HR: 2.792, 95% CI [1.382–5.641], p = 0.004; ACM: HR: 3.102, 95% CI [1.545–6.230], p = 0.001). Similarly, compared to the 6w ≤ TTC ≤ 8w group, patients with TTC > 8w had a 2.343-fold increased risk of GCSM (95% CI [1.060–5.180], p = 0.035) and a 2.719-fold increased risk of ACM (95% CI [1.255–5.892], p = 0.011) (see Table 3).
TTC and mortality risks in subgroup analyses
Supplemental Table 4 illustrates the correlation between TTC and the risk of GCSM and ACM among patients with NLAGC after stratification into different subgroups based on tumor pathological stage, tumor size, lymphovascular invasion, neural invasion, and TRG grade. After adjusting for all confounding factors, no significant correlation between the risk of death and TTC was observed in patients with stage ypCR/I/II disease. However, among patients with stage III gastric cancer, those with TTC < 6w or >8w showed a 2.626-fold (95% CI [1.186–5.814], p = 0.017) and 2.875-fold (95% CI [1.139–7.252], p = 0.025) increased risk of GCSM, respectively, and a 2.908-fold (95% CI [1.323–6.391], p = 0.008) and 3.045-fold (95% CI [1.234–7.516], p = 0.016) increased risk of ACM, respectively. Similar results were also found in subgroups of patients with gastric cancer with tumor size > 5 cm, positive lymphovascular and neural invasion, and TRG 2/3 grade.
Correlation of TTC with overall survival under different regimens and correlation of TTC with time to relapse
We conducted a stratified analysis based on different chemotherapy regimens to evaluate the impact of TTC on prognosis within each regimen group. The analysis showed that in the Paclitaxel regimens group, patients with a TTC of 6–8 weeks had significantly better 3-year overall survival compared to those with TTC < 6 weeks and TTC > 8 weeks (3-year OS: 96.6 vs. 79.5 vs. 64.1%; p = 0.026). Although similar results were not observed in the Platinum-based regimens and Other regimens groups, we found a trend toward better 3-year overall survival in the Platinum-based regimens group for patients with a TTC of 6–8 weeks compared to those with TTC < 6 weeks and TTC > 8 weeks (3-year OS: 79.9 vs. 57.6 vs. 59.9%; p = 0.109) (see Supplemental Figure 4).
Simultaneously, in comparing the peak time of recurrence across different TTC stratifications within the entire population, we observed that the recurrence peak period in the 6w ≤ TTC ≤ 8w group was significantly prolonged compared to the TTC < 6w and TTC > 8w groups (Peak months: 9.7 vs. 4.3 vs. 3.1) (see Figure 3).
Whole-population comparison of time to relapse peaks stratified by TTC.
Clinical implications of chemotherapy timing
Our study found that initiating chemotherapy within the 6–8 week window was associated with improved survival outcomes and delayed recurrence. This timeframe may serve as a reference for clinicians in determining the optimal timing for postoperative chemotherapy in gastric cancer patients, particularly those who have undergone neoadjuvant chemotherapy for locally advanced disease. These findings may contribute to the development of more personalized treatment strategies and potentially improve patient prognosis by reducing the risk of mortality.
Discussion
Surgical intervention remains the primary approach for patients with LAGC, yet the 5-year survival rate for those solely undergoing surgery stands at a mere 20–30% [40]. Extensive prospective studies have underscored the clinical significance of perioperative chemotherapy, establishing it as the standard treatment for LAGC. In studies on other cancers, such as breast cancer [41,42] and ovarian cancer [43,44], it has been shown that initiating postoperative chemotherapy within an appropriate time window has a positive effect on patients receiving neoadjuvant therapy, helping to reduce recurrence and improve survival rates. However, with an increasing cohort of gastric cancer patients undergoing neoadjuvant therapy [4,5], the optimal timing for commencing postoperative adjuvant chemotherapy after neoadjuvant chemotherapy remains ambiguous regarding its impact on patient prognosis.
In this study, we identified a potentially applicable range of time for initiating postoperative adjuvant chemotherapy in patients with LAGC, namely within 6 to 8 weeks after surgery (6w ≤ TTC ≤ 8w). We found that patients who initiated postoperative chemotherapy within this range had significantly lower ACM and GCSM scores than those with TTC < 6w and TTC > 8w. After adjusting for all confounding factors, the TTC remained an independent prognostic factor for ACM and GCSM. To the best of our knowledge, this is the first study to explore the optimal timing for initiating postoperative maintenance chemotherapy in patients with locally advanced gastric cancer following neoadjuvant chemotherapy.
According to extant research, the initiation time of postoperative adjuvant chemotherapy significantly impacts the survival prognosis of various cancers, including LAGC [32,45]. This influence also extends to patients undergoing neoadjuvant therapy, with effects varying among different patient populations. Currently, published studies exhibit discrepancies in selecting the cutoff time for initiating postoperative chemotherapy. The management plan outlined in the Japanese Gastric Cancer Treatment Guidelines suggests that S-1 (adjuvant chemotherapy) should commence within 6 weeks post-surgery, following sufficient recovery from surgical intervention [3]. Both CRC and gastric cancer are malignant tumors of the digestive system. According to Dienstmann et al., an alternative cutoff point for TTC is reported to be 8 weeks post-CRC surgery for commencing adjuvant chemotherapy [46]. Due to both centers’ standard recommendation for patients to commence adjuvant chemotherapy within 6 weeks post-surgery, there was a higher proportion of patients in the TTC < 6w group (70.5%; 318/451) in the study. Our study revealed that patients who initiated chemotherapy within six weeks postoperatively exhibited significantly higher ACM and GCSM values than those within 6w ≤ TTC ≤ 8w. After adjusting for demographic and preoperative characteristics, patients with a TTC < 6w had a 2.395-fold increased risk of GCSM and a 2.736-fold increased risk of ACM. With further adjustments for tumor-related factors and treatment modalities, this relationship strengthened and remained significant.
The recovery of postoperative physiological function in patients with malignant gastric tumors necessitates time. Initiating postoperative adjuvant chemotherapy before a patient’s physiological function fully recovers may exacerbate harm to the patient [47]. Substantial evidence from RCTs confirms the efficacy of NACT in reducing the LAGC stage and improving patient prognosis [48]. However, NACT may elevate postoperative complications [49,50], and the recovery of physiological function after NACT may be inferior to that of patients who did not receive NACT. Therefore, we posit that a reasonable delay in postoperative chemotherapy is appropriate for patients undergoing NACT. Furthermore, in our study, we observed a 2.719-fold increase in the risk of ACM in patients with TTC > 8w compared to those with 6w ≤ TTC ≤ 8w (95% CI, 1.255–5.892; p = 0.011), along with an earlier recurrence peak (recurrence peak time: 3.1 vs. 9.7 months, respectively). This suggests that an excessive delay in initiating postoperative chemotherapy could have adverse prognostic implications for patients.
Previous studies, for instance, Carbognin et al. [51] used sensitivity analysis to evaluate the interaction between paclitaxel and docetaxel in terms of treatment efficacy and adverse effects, concluding that paclitaxel demonstrated a higher pathological complete response (pCR) rate and a lower incidence of severe neutropenia and febrile neutropenia, thereby strengthening the reliability of their findings. Similarly, Mueller et al. [52] applied sensitivity analysis to clarify the advantages of selectively using neoadjuvant chemoradiotherapy under different survival assumptions in locally advanced rectal cancer. Their study provided important clinical decision-making insights, showing that selective treatment strategies could balance efficacy while reducing costs. In this study, we conducted sensitivity analyses across different subgroups, including tumor pathological stage, tumor size, lymphovascular invasion, perineural invasion, and tumor regression grade (TRG), to evaluate the relationship between TTC and survival outcomes in LAGC patients (Supplemental Table 4). Among stage III gastric cancer patients, both TTC < 6 weeks and TTC > 8 weeks were associated with significantly higher risks of gastric cancer-specific mortality (GCSM) and all-cause mortality (ACM) compared to the standard 6–8 week window. Specifically: TTC < 6 weeks: GCSM risk increased by 2.626-fold (95% CI [1.186–5.814], p = 0.017); ACM risk increased by 2.908-fold (95% CI [1.323–6.391], p = 0.008). TTC > 8 weeks: GCSM risk increased by 2.875-fold (95% CI [1.139–7.252], p = 0.025); ACM risk increased by 3.045-fold (95% CI [1.234–7.516], p = 0.016). A similar trend was observed in patients with: Tumor size > 5 cm; Positive lymphovascular invasion and perineural invasion; TRG 2/3. These results suggest that sensitivity analysis further validates the impact of chemotherapy timing on survival outcomes in stage III gastric cancer patients and those with adverse tumor characteristics, thereby providing additional evidence for clinical decision-making.
Furthermore, we found that patients who initiated chemotherapy within 6–8 weeks had a lower risk of recurrence, whereas those who started chemotherapy earlier than 6 weeks or later than 8 weeks exhibited a relatively higher risk. This phenomenon may be associated with the following biological and clinical mechanisms: Firstly, the primary objective of postoperative adjuvant chemotherapy for gastric cancer is to mitigate the risk of tumor recurrence by eradicating residual malignant cells and inhibiting micrometastasis growth, thereby enhancing patient survival. The longer the interval between surgery and adjuvant chemotherapy, the greater the chance of micrometastasis amplification [11,12,53]. The rapid proliferation of residual cancer cells could render adjuvant chemotherapy beyond a certain time threshold minimally impactful on survival outcomes [54]. Animal model studies have also suggested that surgery may increase the number of circulating tumor cells, which could enhance metastatic growth and be associated with reduced angiogenesis and elevated oncogenic growth factors [13,14]. Secondly, Previous studies have indicated that gastric cancer patients require a certain period for physiological recovery after surgery. Initiating chemotherapy too early, before sufficient recovery, may impose an excessive burden on patients, leading to suboptimal treatment outcomes. In particular, early chemotherapy could excessively suppress the immune system, impairing immune recovery and negatively impacting long-term survival and recurrence [45]. However, not all patients voluntarily delay chemotherapy. Previous studies have indicated that advanced age, socioeconomic status, insurance coverage, and postoperative complications, influence chemotherapy timing [15,55,56]. Park et al. [22] reported that the most common reason for delayed chemotherapy beyond 8 weeks in gastric cancer patients was postoperative complications, while Datta et al. [57] found that most patients who experienced unplanned postoperative readmissions did not receive adjuvant treatment. These factors can affect subsequent treatment and indirectly impact patient prognosis. In this study, we adjusted for potential confounders using multivariate Cox regression analysis, including patient characteristics: age (≥65 vs. <65 years), sex (male vs. female), and BMI (≥25 vs. <25 kg/m^2^); perioperative status: ASA score (1/2/3), reflecting baseline health status and perioperative tolerance; tumor characteristics: ypStage (pathological stage), tumor size (≥5 vs. <5 cm), tumor location (upper/middle/lower/mixed), lymphovascular invasion, neural invasion, and R0/R1 resection status; and treatment-related factors: postoperative chemotherapy cycles (≥4 vs. <4 cycles), chemotherapy initiation time (TTC <6, 6–8, >8 weeks), and tumor regression grade (TRG 0/1 vs. 2/3). Through multivariate analysis, we eliminated these potential confounding factors and found that TTC remained an independent prognostic factor. Initiating chemotherapy within 6–8 weeks may provide an optimal time window that balances sufficient recovery with effective tumor suppression.
To further clarify the reasons for delayed chemotherapy, we compared the incidence of postoperative complications between the TTC > 8w and TTC ≤ 8w groups (see Supplemental Table 5). The results showed that the incidence of postoperative complications was higher in the TTC > 8w group compared to the TTC ≤ 8w group (15.3 vs. 14.9%), and the incidence of Clavien-Dindo grade ≥ II complications was also higher in the TTC > 8w group (6.5 vs. 11.9%). Therefore, the delay in TTC may be potentially associated with the occurrence of postoperative complications. Thus, avoiding excessive delays in initiating chemotherapy and selecting the appropriate time to commence postoperative chemotherapy is imperative.
In this study, we also found that the timing of postoperative chemotherapy initiation had a stronger impact on prognosis than R0 resection. However, when we compared the R1 resection rates and R0 resection rates among the three groups (TTC < 6w, 6w ≤ TTC ≤ 8w, and TTC > 8w), we found that the R1 resection rates were 10.1, 15.2, and 14.9%, respectively, which were significantly lower than the R0 resection rates in each group (89.9, 84.8, and 85.1%, respectively) (see Table 1). It is likely that the large difference in sample sizes between patients with R0 and R1 resections led to a relatively weaker association between R0 resection and postoperative prognosis, whereas the impact of the timing of postoperative chemotherapy initiation was more significant in the statistical analysis. In the multivariate analysis, we also found no significant differences in the efficacy of preoperative chemotherapy (TRG grade) among patients, but differences were observed in the timing of chemotherapy initiation. This may be because TRG primarily assesses tumor response to NACT, reflecting the effectiveness of preoperative chemotherapy. However, TRG does not directly involve postoperative treatment or control of tumor recurrence. A study by Kim et al. indicated that although patients with complete pathological response (TRG1a) are expected to have favorable survival outcomes, those with TRG1b had worse survival outcomes than patients with TRG2. Therefore, the association between pathological response and survival outcomes is not entirely consistent [58]. Similar results have been observed in other studies [35,59]. Thus, while TRG is a good predictor of response to NACT, other direct prognostic indicators, such as the timeliness of postoperative treatment (chemotherapy), may be more important for long-term survival [60].
Our study presents several limitations. Firstly, being a retrospective study, it is subject to selection bias. However, this study minimized bias as much as possible by adopting consecutive patient enrollment and conducting multivariable analysis. Secondly, there were relatively few cases within the 6 to 8-week timeframe after initiating postoperative chemotherapy among patients with LAGC who received NACT. However, these real-world clinical data analyses provide valuable insights into the optimal timing of postoperative chemotherapy across different cancer types. Thirdly, due to the retrospective nature of data collection in this study, we did not adequately collect and comprehensively record relevant data on genetic factors and socioeconomic variables. Further discussion on their relevance is needed in future research. Retrospective studies like ours remain crucial for identifying trends and generating hypotheses that guide future research. As the first study focusing on the optimal timing for postoperative chemotherapy initiation in LAGC patients receiving NACT, we hope it provides valuable reference for future study. Since this study is based on a Chinese patient cohort, the global applicability of our findings may be somewhat limited. Therefore, future research should aim to validate these results through large-scale, multicenter, and prospective studies to enhance the generalizability of the conclusions.
Conclusion
Patients with NLAGC and a TTC between 6 and 8 weeks may have lower GCSM and ACM compared to those with TTC < 6 weeks or more than 8 weeks. Efforts should be made to initiate postoperative adjuvant chemotherapy at appropriate times, especially for high-risk patients with ypTNM stage III, tumor size of 5 cm or larger, positive lymphovascular/neural invasion, and TRG 2/3 grades.
This study has significant implications for clinical practice, highlighting that the timing of postoperative adjuvant chemotherapy should be considered a critical factor in treatment decision-making. The findings provide preliminary evidence to support potential revisions to current treatment guidelines for gastric cancer patients receiving neoadjuvant chemotherapy. Since this study is retrospective, large-scale, multicenter, prospective clinical trials are needed to further validate the impact of different chemotherapy timing strategies on survival outcomes in stage III gastric cancer patients and those with specific adverse tumor characteristics.
Supplementary Material
IANN-2024-5913.R1-Supplementary Table clean copy.docx
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi: 10.3322/caac.21660.33538338 · doi ↗ · pubmed ↗
- 2Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries [published correction appears in CA Cancer J Clin. 2020 Jul;70(4):313]. CA Cancer J Clin. 2018;68(6):394–424. doi: 10.3322/caac.21492.30207593 · doi ↗ · pubmed ↗
- 3Nakanishi K, Kanda M, Ito S, et al. Delay in initiation of postoperative adjuvant chemotherapy with S-1 monotherapy and prognosis for gastric cancer patients: analysis of a multi-institutional dataset. Gastric Cancer. 2019;22(6):1215–1225. doi: 10.1007/s 10120-019-00961-9.30955110 · doi ↗ · pubmed ↗
- 4Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006;355(1):11–20. doi: 10.1056/NEJ Moa 055531.16822992 · doi ↗ · pubmed ↗
- 5Ychou M, Boige V, Pignon JP, et al. Perioperative chemotherapy compared with surgery alone for resectable gastroesophageal adenocarcinoma: an FNCLCC and FFCD multicenter phase III trial. J Clin Oncol. 2011;29(13):1715–1721. doi: 10.1200/JCO.2010.33.0597.21444866 · doi ↗ · pubmed ↗
- 6Al-Batran SE, Homann N, Pauligk C, et al. Effect of neoadjuvant chemotherapy followed by surgical resection on survival in patients with limited metastatic gastric or gastroesophageal junction cancer: the AIO-FLOT 3 trial. JAMA Oncol. 2017;3(9):1237–1244. doi: 10.1001/jamaoncol.2017.0515.28448662 PMC 5824287 · doi ↗ · pubmed ↗
- 7Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2021 (6th edition). Gastric Cancer. 2021;24(1):1–19.36342574 10.1007/s 10120-022-01331-8PMC 9813208 · doi ↗ · pubmed ↗
- 8Ajani JA, D’Amico TA, Almhanna K, et al. Gastric cancer, version 3.2016, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2016;14(10):1286–1312. doi: 10.6004/jnccn.2016.0137.27697982 · doi ↗ · pubmed ↗