Clinical features of talaromycosis in people living with HIV/AIDS (PWHA) and patients with anti-interferon-γ autoantibodies
Kawisara Krasaewes, Narootchai Patanadamrongchai, Quanhathai Kaewpoowat, Jiraprapa Wipasa, Saowaluck Yasri, Antika Wongthanee, Romanee Chaiwarith, Thuy Le, Thuy Le, Thuy Le, Marcio Rodrigues, Marcio Rodrigues

TL;DR
This study compares how talaromycosis affects HIV patients and those with anti-interferon-gamma autoantibodies, highlighting differences in symptoms and outcomes.
Contribution
The study identifies distinct clinical features of talaromycosis in patients with anti-IFN-γ autoantibodies compared to HIV/AIDS patients.
Findings
Patients with anti-IFN-γ autoantibodies had more skin and subcutaneous lesions and bone/joint infections.
PWHA showed more constitutional symptoms and umbilicated skin lesions.
Mortality rates were not significantly different between the two groups.
Abstract
Talaromycosis is increasingly reported in HIV-uninfected, immunocompromised individuals in an endemic area. The aim of this study was to compare the characteristics and mortality associated with talaromycosis in adult immunocompromised individuals caused by the anti-interferon-gamma autoantibody (anti-IFN- γ AAb) with those of people living with HIV/AIDS (PWHA). A retrospective cohort study was conducted at Maharaj Nakorn Chiang Mai Hospital, Thailand, in adults with confirmed HIV infection or anti-IFN- γ-AAbs diagnosed with talaromycosis. Thirty-two patients with anti-IFN- γ-AAbs and 235 PWHA were included. Patients with anti-IFN- γ-AAbs were older and more likely to have comorbidities. PWHA were more likely to have constitutional symptoms, cough, dyspnea, diarrhea, splenomegaly, umbilicated skin lesions, abnormal chest radiographs, and fungemia. Patients with anti-IFN- γ-AAbs were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
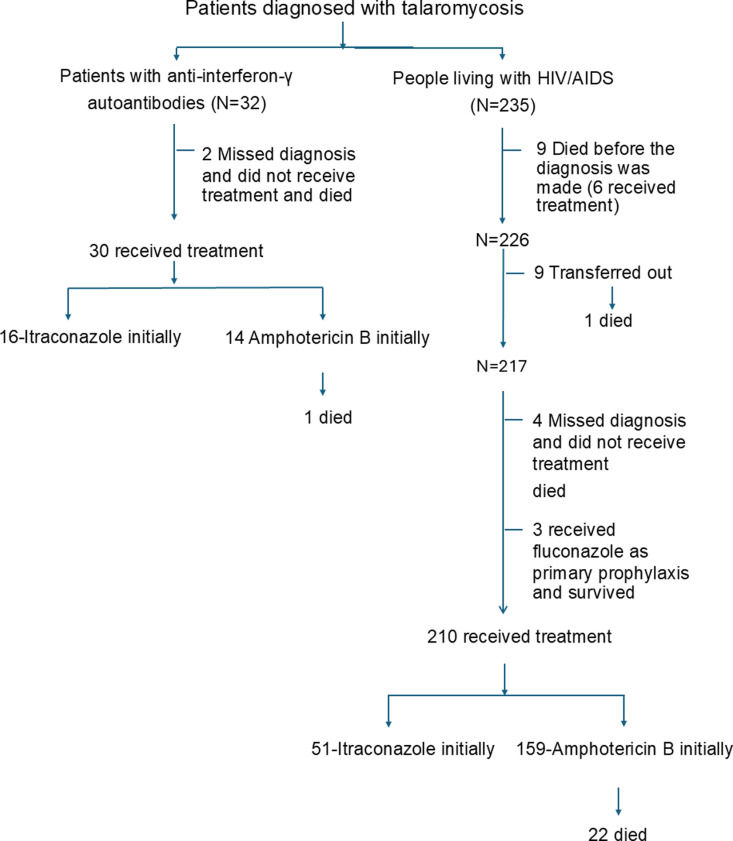 Fig 1
Fig 1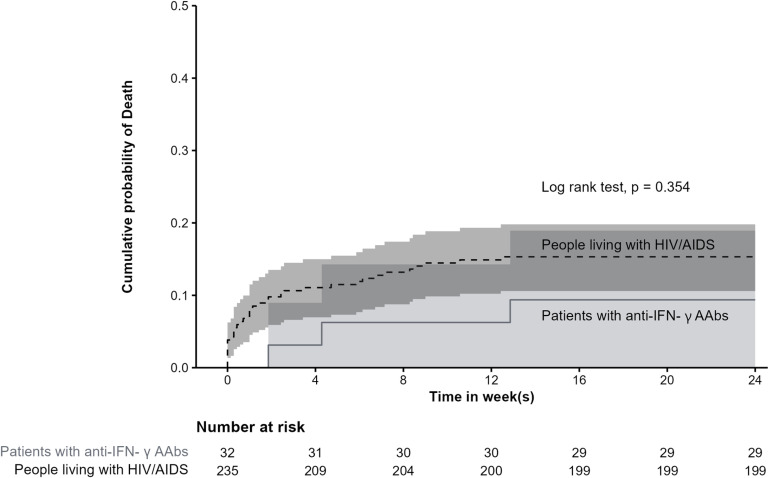 Fig 2
Fig 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFungal Infections and Studies · Mycobacterium research and diagnosis · Cytomegalovirus and herpesvirus research
Introduction
Talaromycosis, a disseminated infection caused by Talaromyces marneffei, is a common opportunistic endemic fungal infection in people with HIV/AIDS (PWHA) living in tropical and subtropical Asia, especially when the CD4 cell count is < 100 cells/µL. [1]. The clinical features of talaromycosis in PWHA are well described in the literature, with classic central necrotic (umbilicated) papules appearing on the face, trunk and extremities, fever, weight loss, hepatosplenomegaly, lymphadenopathy, respiratory and gastrointestinal abnormalities [1–3]. The incidence of talatomycosis in PWHA has decreased dramatically since the introduction of antiretroviral therapy [4]. However, talaromycosis has been increasingly observed in immunocompromised non-HIV hosts with an impaired cell-mediated immune response, such as those with autoimmune diseases, cancer and organ transplants, as well as those receiving immunosuppressive therapy [4]. Recently, there has been a growing number of studies of adult-onset immunodeficiency (AOID) caused by anti-interferon-γ autoantibodies (anti-IFN- γ AAbs) [5–8]. This condition is reported to be most prevalent in China and Southeast Asia, including Thailand, an area where T. marneffei is endemic. Talaromycosis has been reported to occur in these patients alongside other disseminated infections with tuberculous mycobacteria, non-tuberculous mycobacteria and other dimorphic fungal infections [5–8]. Data on the clinical features of talaromycosis in patients with anti-IFN- γ AAbs are limited [7,9]. We previously reported the clinical features of patients with talaromycosis in HIV-uninfected patients between 2007 and 2011; however, the cause of immunodeficiency was not fully investigated [10]. Here, we described clinical features and outcomes of talaromycosis in patients with confirmed anti-IFN- γ AAbs and PWHA in northern Thailand, where T. marneffei is endemic.
Methods
Ethics statement
The study was approved by the Research Ethics Committee, Number 4, of the Faculty of Medicine, Chiang Mai University. The approval certificate number is 224/2021. Due to the retrospective nature of the study, written/verbal informed consent was not obtained.
A retrospective cohort study was conducted at Maharaj Nakorn Chiang Mai Hospital, a teaching hospital of Chiang Mai University, Chiang Mai, Thailand. Patients aged 18 years and older with the ICD-10 code B48.4 (talaromycosis) attending Maharaj Nakorn Chiang Mai Hospital were studied. Those who met the definition of talaromycosis, defined by a positive culture of T. marneffei from sterile sites or proven by histopathology, with documentation of HIV infection according to the national standard guideline [11] or detection of anti-IFN- γ AAbs by ELISA [8], were included in the study. During the study period from January 1, 2012 to June 30, 2021, 32 patients with anti-IFN- γ AAbs and 235 PWHA diagnosed with talaromycosis were included in the analysis. The flow chart of the participants is shown in Fig 1.
Flow chart, treatment, and outcome of the study participants.
Demographic data, clinical characteristics, laboratory findings, treatment and treatment outcomes were reviewed and extracted from the medical and laboratory records. If a patient lost to follow up or transferred to another hospital, the patient’s status was obtained from the Thai civil registry. In the case of a deceased patient, the date of death was determined.
Laboratory test for antibody to IFN-γ using ELISA
The test for antibodies to IFN-γ was performed using an enzyme-linked immunosorbent assay (ELISA), which was modified from the methods previously described by Tang et al [12]. In brief, 2% skimmed milk in phosphate-buffer saline (PBS) was used in blocking buffer and diluent, replacing the 5% normal goat serum used in the original method. Additionally, o-phenylenediamine dihydrochloride (OPD) was utilized as the substrate instead of tetramethylbenzidine (TMB), as described by Tang et al [12].
Opportunistic infection definitions
Concurrent opportunistic infections (OI) and previous OI are OI diagnosed within 2 weeks and more than 2 weeks after the diagnosis of talaromycosis, respectively.
Data analysis
Data were expressed as number and persentage for categorial data, or mean and standard deviation (SD) or median (interquartile range; IQR) for continuous data. Comparisons between groups were performed using the chi-square test or Fisher’s exact test for categorical data and Student’s t-test or Mann-Whitney U test for continuous data. The cumulative probability of death was calculated and presented with Kaplan-Meier curves. The difference in mortality rate between 2 groups was compared using the log-rank test. Statistical analyses were performed with R software Ver.4.1.2. A two-sided test at a p-value of < 0.05 was used to indicate statistical significance.
A publicly available dataset, representing 25% of the total data and excluding potentially identifying or sensitive patient information, is accessible at http://datadryad.org/stash/share/6ZhPOCnttzu1dB5_dSPHjH2re1duibabSXtB3YOIXPI [13]. The remaining datasets are available from the corresponding author upon reasonable request.
Results
Thirty-two patients with anti-IFN- γ-AAbs had a median (IQR) age of 57.5 (52.8, 63.0) years, and 19 of them (59.4%) were male. Nineteen patients had comorbidities (59.4%). Two hundred and thirty-five PWHA had a median (IQR) age of 35.0 (29.0, 43.0) years, and 174 of them (74.0%) were male. Patients with anti-IFN- γ-AAbs were more likely to be older and to have underlying diseases, particularly hypertension, dyslipidemia, and chronic kidney disease. (Table 1)
Table 1: Demographic and clinical characteristics of patients with talaromycosis between patients with anti-IFN- γ AAbs and people with HIV/AIDS (PWHA).
Clinical characteristics
Compared to PWHA, patients with anti-IFN- γ AAbs had less frequent constitutional symptoms (fever, fatigue, weight loss, anorexia), cough, dyspnea, diarrhea, splenomegaly, and umbilicated skin lesions, but more frequent bone and joint involvement such as arthritis, osteomyelitis, spondylodiscitis, and paravertebral abscesses. The skin lesions commonly seen in patients with anti-IFN- γ AAbs were more diverse and include macules/patch, papules/plaques, nodules, abscesses and Sweet’s syndrome whereas PWHA were more likely to have central umbilicated skin lesions. (Table 1)
Laboratory and findings
Patients with anti-IFN- γ-AAbs more frequently had higher white blood cells, eosinophil, platelet counts and alkaline phosphatase level, less frequently transaminitis and fungemia than PWHA. Three PWHA had neither a CD4 count < 200 cells/ µ L nor a CD4 < 14%. The CD4 counts (%) of these 3 PWHA at the time of diagnosis of talaromycosis were 264 cells/ µ L (18%), 325 cells/ µ L (20%) and 527 cells/ µ L (23%) (30%). These 3 patients had no other immunosuppressive conditions. Patients with anti-IFN- γ AAbs were less likely to have an abnormal chest radiograph. Alveolar infiltration and pleural effusion were more common in patients with anti-IFN- γ AAbs, whereas interstitial infiltration was less common (Table 2).
Table 2: Laboratory findings and treatment outcome of patients with talaromycosis in patients with anti-IFN- γ AAbs and people with HIV/AIDS (PWHA).
Treatment and outcomes
Two patients with anti-IFN-γ autoantibodies (AAbs) were not diagnosed with talaromycosis, were not treated, and subsequently died. Among the 30 patients who received treatment, 29 (96.7%) were initially treated with itraconazole, and all survived. One patient, who was treated with amphotericin B followed by itraconazole, died of hospital-acquired pneumonia despite showing clinical improvement after treatment for talaromycosis.
Nine PWHA died before a diagnosis of talaromycosis was made; six of them received empirical treatment with amphotericin B, while three did not received any treatment. Among the remainder 217 patients, nine were transferred to another hospital, including one who died. Four patients missed the diagnosis of talaromycosis, were not treated, and died. Three patients missed the diagnosis of talaromycosis but received fluconazole as primary prophylaxis and survived. Of 216 patients who received treatment, 51 (53.3%) were initially treated with itraconazole and all survived. Ninety-seven patients were initially treated with amphotericin B, 22 of whom died. (Fig 1)
The time from first symptom to treatment and the time from diagnosis to treatment was longer in patients with anti-IFN- γ-AAbs. (Table 2).
Mortality.
Three patients with anti-IFN- γ AAbs and 36 PWHA died with a 24-week mortality of 9.4%% and 15.3%, respectively. The median time from diagnosis to death was 30 days (IQR 21.5-60.0) for patients with anti-IFN- γ AAbs and 7 days (IQR 0.8-35.0) for PWHA (p-value = 0.111). The probability of death is shown in Fig 2. The causes of death were attributed to talaromycosis in 18 patients, cryptococcosis in 1 patient, disseminated tuberculosis in 1 patient, salmonellosis in 1 patient, Pneumocystis pneumonia in 1 patient, and cytomegalovirus pneumonia in 1 patient. Additionally, 9 patients died from hospital-acquired infections, 4 from non-infectious causes, and 3 due to undetermined causes following referral to other hospitals.
Probability of death of patients with talaromycosis between patients with anti-IFN- γ AAbs and people living with HIV/AIDS.Note: The shading represents the 95% confidence interval (CI). Two 95% CIs overlap.
Comparisons of clinical characteristics of talaromycosis in patients with anti-interferon-γ autoantibody with other studies
There have been few reports of talaromycosis specifically in patients with anti-IFN-γ autoantibodies (AAbs). The details of studies conducted by Guo et al [7], and the present study are summarized in Table 3. A common finding across these studies is that the median age of patients was over 50 years, with the majority presenting with fever, weight loss, cough, and lymphadenopathy. The prevalence of skin lesions varied between studies, ranging from 26% to 69%.
Table 3: Comparisons of three studies of talaromycosis in patients with anti-interferon-γ autoantibody.
Discussion
Talaromycosis has been reported in HIV-uninfected patients with conditions such as anti-IFN-γ autoantibodies (AAbs), autoimmune diseases, organ transplantation, hematologic malignancies, and novel cancer therapies [4,14].
Comparison of the clinical features of talaromycosis between patients with anti-IFN- γ-AAbs and PWHA has rarely been reported. In this study, the clinical features of talaromycosis were directly compared between these two groups, and some differences were found. Patients with anti-IFN- γ-AAbs were older (all were ≥ 40 years old) and had a higher proportion of underlying disease. In contrast to PWHA, patients with anti-IFN- γ-AAbs had previous infections before the diagnosis of talaromycosis, and the most common previous/current infections were non-tuberculous mycobacteria, tuberculosis, salmonellosis, and Pneumocystis pneumonia. These findings are consistent with previous reports of OI in patients with anti-IFN- γ-Aabs [5,6,15]. In addition, patients with anti-IFN- γ-AAbs had bone and joint infections and a lower proportion of fungemia. Since T cell-mediated immune responses play an important role in fighting T. marneffei infection, the advanced stage of HIV infection, which leads to a loss of CD4 + T cells and subsequently a loss of activation of cellular signaling pathways, results in an inability to control the infection [16], and fungemia was observed more frequently in PWHA [1–3]. Leukocytosis and higher platelet counts were found in patients with anti-IFN- γ AAbs, which could be due to the inflammatory cascade [17]. Abnormal CXR was found in 30% of patients with anti-IFN- γ AAbs. Since the route of transmission of talaromycosis is through inhalation of T. marneffei spores from the environment, the pulmonary symptoms and abnormal CXR are not unexpected [18]. The time from diagnosis of taralomycosis to initiation of treatment was longer in patients with anti-IFN- γ-AAbs, because patients who were not critically ill, were not hospitalized, and had a treatment appointment at the outpatient clinic that may not have occurred on the same day that cultures or pathology reports were available. This may explain why patients with anti-IFN- γ-AAbs were more likely to receive itraconazole initially than PWHA.
Itraconazole has a low minimum inhibitory concentration (MIC) against T. marneffei [19,20] and has been shown to be effective in the initial treatment of talaromycosis with mild disease [21,22]. The archived guidelines (through October 22, 2019) for the prevention and treatment of opportunistic infections in HIV-infected adults and adolescents from the Centers for Disease Control and Prevention, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America suggest that initial treatment with itraconazole is the preferred therapy for patients with mild disease [23]. However, since the November 21, 2019, itraconazole is no longer recommended as induction therapy for talaromycosis, as the results of IVAP trial in PWHA, which showed the superiority of amphotericin B over itraconazole in the induction phase, regardless of disease severity and faster fungal clearance in blood culture [2,23]. Whether similar results apply to other populations, including patients with anti-IFN- γ-AAbs, and whether faster fungal clearance may influence clinical outcomes in patients with anti-IFN- γ-AAbs remains to be determined. Not surprisingly, all but one patient with anti-IFN- γ-AAbs initially received itraconazole because they were not ill enough to be hospitalized in a hospital with limited admission capacity and were willing to receive oral therapy and be closely monitored in the outpatient clinic as they were able to return to work.
The mortality rate in PWHA (14.8%) was in the range of previous studies (12.6% - 33%) [2,7,10,24–26]. The rate in patients with anti-IFN- γ AAbs was 9%, which was lower than the rate reported by Chen et al. (14%) [9] and Guo et al. (22%) [7]. In this study, the mortality rate of talaromycosis in patients with anti-IFN- γ-AAbs was not statistically different from PWHA. Our earlier study showed that the mortality rate in HIV-uninfected patients was 20.7%. However, the exact proportion of patients with anti-IFN-γ-AAbs was not known [10].
The strength of this study is that it is one of the few studies comparing clinical features and outcomes of talaromycosis in patients with anti-IFN- γ-AAbs and PWHA from an area where T. marneffei is endemic and HIV infection is prevalent. This study raised awareness among physicians caring for these patients, especially in the endemic area.
However, there were several limitations. First, the sample size may not be large enough to detect differences between groups, if any. Second, as the nature of retrospective study, which was not designed for systematic data collection, there were data missing, i.e., not all patients had performed blood cultures, not all PWHA had baseline CD4 count, and chest radiograph. Third, patients with anti-IFN- γ-AAbs may have concurrent infections, so the timing of first symptom onset may not be accurate.
Conclusions
The clinical features of talaromycosis in patients with anti-IFN- γ AAbs differed in some aspects from PWHA. Awareness of talaromycosis in patients with anti-IFN- γ AAbs, even in the absence of detection of T. marneffei in blood cultures, may shorten the time from initial symptoms to diagnosis and treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Supparatpinyo K, Khamwan C, Baosoung V, Nelson KE, Sirisanthana T. Disseminated Penicillium marneffei infection in southeast Asia. Lancet. 1994;344(8915):110–3. doi: 10.1016/s 0140-6736(94)91287-4 7912350 · doi ↗ · pubmed ↗
- 2Le T, Kinh NV, Cuc NTK, Tung NLN, Lam NT, Thuy PTT, et al. A trial of itraconazole or amphotericin B for HIV-associated talaromycosis. N Engl J Med. 2017;376(24):2329–40. doi: 10.1056/NEJ Moa 1613306 28614691 · doi ↗ · pubmed ↗
- 3Ying RS, Le T, Cai WP, Li YR, Luo CB, Cao Y, et al. Clinical epidemiology and outcome of HIV-associated talaromycosis in Guangdong, China, during 2011-2017. HIV Med. 2020;21(11):729–38. doi: 10.1111/hiv.13024 33369035 PMC 7978497 · doi ↗ · pubmed ↗
- 4Chan JFW, Lau SKP, Yuen K-Y, Woo PCY. Talaromyces (Penicillium) marneffei infection in non-HIV-infected patients. Emerg Microbes Infect. 2016;5(3):e 19. doi: 10.1038/emi.2016.18 26956447 PMC 4820671 · doi ↗ · pubmed ↗
- 5Angkasekwinai N, Suputtamongkol Y, Phoompoung P, Pithukpakorn M, Wongswat E, Umrod P, et al. Clinical outcome and laboratory markers for predicting disease activity in patients with disseminated opportunistic infections associated with anti-interferon-γ autoantibodies. P Lo S One. 2019;14(4):e 0215581. doi: 10.1371/journal.pone.0215581 31022229 PMC 6483193 · doi ↗ · pubmed ↗
- 6Browne SK, Burbelo PD, Chetchotisakd P, Suputtamongkol Y, Kiertiburanakul S, Shaw PA, et al. Adult-onset immunodeficiency in Thailand and Taiwan. N Engl J Med. 2012;367(8):725–34. doi: 10.1056/NEJ Moa 1111160 22913682 PMC 4190026 · doi ↗ · pubmed ↗
- 7Guo J, Ning X-Q, Ding J-Y, Zheng Y-Q, Shi N-N, Wu F-Y, et al. Anti-IFN-γ autoantibodies underlie disseminated Talaromyces marneffei infections. J Exp Med. 2020;217(12):e 20190502. doi: 10.1084/jem.20190502 32880631 PMC 7953730 · doi ↗ · pubmed ↗
- 8Wongkulab P, Wipasa J, Chaiwarith R, Supparatpinyo K. Autoantibody to interferon-gamma associated with adult-onset immunodeficiency in non-HIV individuals in Northern Thailand. P Lo S One. 2013;8(9):e 76371. doi: 10.1371/journal.pone.0076371 24086734 PMC 3785451 · doi ↗ · pubmed ↗