Consensus on core competencies for simulation training in ultrasound-guided renal biopsy
Andrea J. Doyle, Colin P. Cantwell, Claire Mulhall, Richard Arnett, Claire M. Condron

TL;DR
This paper outlines essential skills for performing ultrasound-guided kidney biopsies and proposes a simulation-based training approach for radiology trainees.
Contribution
The study identifies 23 core competencies and proposes a simulation curriculum for ultrasound-guided renal biopsy training.
Findings
24 competencies were identified across seven procedural domains, with one removed due to disagreement.
Simulation strategies included three domains using simulated participants and four using hybrid methods.
A blueprint for a simulation curriculum was developed to meet training requirements for radiologists.
Abstract
To define the competencies in ultrasound knowledge and skills that are essential for interventional radiology trainees to master when performing ultrasound-guided renal biopsy, and to design simulation-based training to develop these competencies. A whole-task training and competency-based assessment methodology was adopted. 42 fellowship-trained interventional radiologists were contacted to participate in the process. An anonymous three-round modified Delphi process was used to identify and assess the crucial procedural steps in performing an ultrasound-guided renal procedure. The primary survey round allowed free text submission of the procedure steps. The primary survey was analysed to identify the common key tasks and these were grouped in procedural domains. For rounds two and three consensus on key steps was evaluated. 75% agreement was required to progress to the final task…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
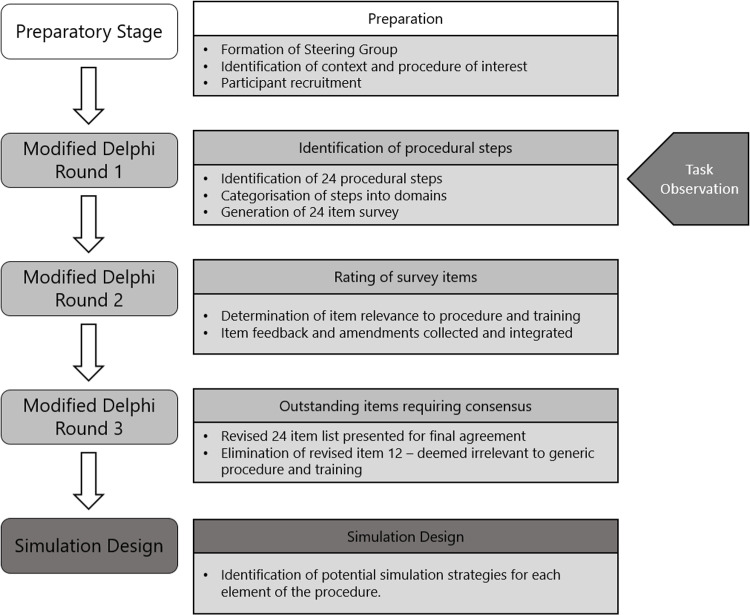 Fig 1
Fig 1- —http://dx.doi.org/10.13039/501100002081Irish Research Council
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUltrasound in Clinical Applications · Surgical Simulation and Training · Radiology practices and education
Introduction
Ultrasound-guided renal procedures are widely performed by an interventional radiologist and are an effective and minimally invasive alternative to conventional surgery. Ultrasound-guidance is used extensively in procedures including focal and non-focal renal biopsy, cyst aspiration, nephrostomy catheter insertion, and renal tumour ablation. The advantages and benefits of this ultrasound-guided approach include a reduction in complications (including infection and blood loss), less pain (due to the small incision sites), patient convenience (minimally invasive, and often an outpatient procedure) and lower costs [1]. However, these benefits are only assured if the interventional radiology (IR) services have a highly trained workforce.
The success of IR procedures relies on the interventional radiologist’s ability to interpret ultrasound images in real-time to guide and manipulate a needle in the body to a target [2]. All ultrasound-guided procedures in the kidney require significant dexterity and cognitive decision-making skills to manage the ultrasound image, identify the target, identify the non-target organs and obstructions, optimise image quality, mitigate image artefacts, and guide the applicator or needle to the correct location in the body [3].
There is an identified need to develop simulation-based training to assist with training interventional radiologists to perform renal procedures [4]. There is an increasing demand for trained interventional radiologists in the UK and Ireland to keep staffing levels in line with European averages [1,5]. In 2020, a European-wide needs assessment was conducted to reach consensus on the technical procedures in radiology to include in simulation-based training for residents. A Delphi working group of international radiology and medical education experts highlighted the need for basic ultrasound operation as the top ranked procedure for simulation-based training, with ultrasound kidney imaging and ultrasound guidance for interventional procedures ranking third and sixth respectively [4].
The optimal implementation of simulation-based medical education (SBME) remains poorly reported and while best practice is yet to be defined, studies have begun to characterise and evaluate factors that would impact the quality of SBME curricular implementation [6,7]. The need for training identified through problem identification and a general needs assessment is recognised as the first step in the systematic design in curricular development [8]. A needs assessment involving stakeholders with contextual expertise is pertinent to problem identification and definition, and in distinguishing the critical clinical competencies associated of the intended intervention [9]. In this study, we employ a modified Delphi consensus process to define the critical procedural steps associated with ultrasound guided kidney interventional radiology biopsy procedures. Though the consensus process we aim to define the competencies in ultrasound knowledge and skills that are essential for trainees to master performing ultrasound-guided renal biopsy.
Materials and methods
This study was approved by the RCSI University of Medicine and Health Sciences Research Ethics Committee REC202207005.
Steering group
A steering group was formed with members with expertise in interventional ultrasound, medical education, simulation and curriculum development. AJD convened the steering group and led the modified Delphi investigation with collaboration from other authors (CPC, CM, RA, and CMC).
Participant recruitment
Participants were canvased to enrol in the study via email through the national network of fellowship trained IR consultants, the Irish Society of Interventional Radiology (https://isir.i.e.,) their participation was voluntary and their anonymity was maintained throughout the process. Participants were recruited from 22^nd^ November through to 22^nd^ December 2023. Participants were provided with an information leaflet when they were invited to participate. On conformation of their interest to participate, participants were sent an electronic consent form to complete and sign before the study began. CM acted as a gatekeeper for participant data and corresponded with the participants through email and de-identified the study data before other members of the steering group accessed data.
Study design
Modified Delphi [10] and task analysis [11] processes were integrated in this study to identify the critical procedural steps associated with ultrasound guided kidney biopsies, see Fig 1. This dual approach enabled the lead investigator (AJD) to better understand the contextual information returned in each round of the modified Delphi process, by observing ultrasound guided kidney biopsy procedures at a clinical site.
Overview of the modified Delphi process including task observation, data collection and analysis summaries.
Participants were not required to convene in person; instead, their anonymous responses were shared with the group in subsequent rounds for further exploration until a consensus was achieved. Data collection was performed using an online Microsoft Form. The initial list of procedural steps was generated by the panellists in the first round of data collection, in subsequent rounds these list items were rated in terms of their importance, modified for utility, and categorised into domains [12]. This data was then presented to the participants in subsequent rounds, and participants expressed their level of agreement concerning the significance of each item in relation to the procedure and consequently training, choosing from ‘Strongly Disagree,’ ‘Disagree,’ ‘Neither Agree nor Disagree,’ ‘Agree,’ and ‘Strongly Agree.’ An a priori threshold of 75% agreement between panellists was established [13]. The identified procedure domains were further interrogated by the research team to determine potential simulation strategies that could be incorporated into a SBME training intervention.
Data collection and analysis
Round 1.
The first Delphi round presented panellists with an open-ended question, designed to capture their collective expertise and identify the skills required to perform ultrasound guided kidney biopsy.
“Your patient has arrived in the radiology suite for a scheduled renal focal lesion biopsy interventional radiology procedure. Please describe the process for an ultrasound guided interventional radiology procedure of the kidney. In as much detail as possible*, please include the steps you would take and the order in which you do them. There is no limit to the length of your response.”*
Panellists were encouraged to provide free-text descriptors and there was no word limit associated with their responses. During this first Delphi round, ultrasound guided kidney procedures performed by IR consultants at clinical sites were observed by AJD. Data from the first Delphi round captured the panellists’ approaches to the kidney biopsy procedure, and were grouped and sequenced (see Appendix) by AJD with support of CPC, a Consultant Interventional Radiologist and CMC, Director of Simulation Education.
Round 2.
In the second Delphi round, panellists were then asked to review the list of items generated in the previous round, and were required to report their agreement regarding the importance of each listed item in terms of its relevance to the procedure. Participants indicated their agreement level regarding the importance of each item concerning the procedure, and thus, training, by selecting from ‘Strongly Disagree,’ ‘Disagree,’ ‘Neither Agree nor Disagree,’ ‘Agree,’ and ‘Strongly Agree.’ Additionally, participants contributed supplementary information they considered essential by utilizing free-text boxes provided at the conclusion of each section in the Microsoft Form.
Round 3.
The items that reached consensus as important in round 2 were included in the third Delphi round, however participants were only required to rate an outstanding item. After this final Delphi round the research team, including RA, Director of Psychometrics, reviewed the data and finalised the competency list.
Simulation design.
The final competency list was reviewed by the steering group. The group specified the simulation based educational training intervention that is the most effective simulation strategies for each element of the procedure.
Results
Of the 42 interventional radiologists invited to complete the process, nine completed the three-round modified Delphi process (21%). The median participant age was 51 (34–63) years, with years of professional practice (outside of training) ranging from ≤1–28 years. Table 1 presents the demographic profiles of the participants in the Delphi process.
Table 1: Participant demographic information.
Round 1.
During the initial Delphi round, AJD observed three ultrasound-guided kidney procedures conducted by IR consultants. AJD documented each step as the consultant verbally outlined their approach and organized the procedural tasks in sequence. Clarifying questions were posed to gain insight into the event sequencing and to observe the interactions between IR consultants and other healthcare professionals participating in the procedure. Using descriptive analysis, the task observation data was integrated with the first-round data, and supported the categorisation of a list of items into domains for ultrasound guided kidney biopsy procedures.
The 24-item list categorised into seven domains generated in round 1 is included in the Appendix. This categorised list was sent to the participants in the second round.
Round 2.
In the second Delphi round, panellists reviewed the 24-item list. The results of participant rating that in round two are presented in Table 2. 23 items reached consensus, with 75% agreement, with minor additional amendments suggested from participants.
Table 2: Participant agreement Delphi Round 2 and Round 3.
Item 12 from the domain Prepare Interventional Radiology Suite & Communicate with Colleagues caused dissensus, related to local policies. One participant shared the following rationale for disagreeing with this statement, “If blood pressure is too high, I would not waste time trying to get it to a normal level. I would discuss with referring doctor and just postpone the procedure until they can optimise the BP” [P4]. Another commented “High BP has always dropped with sedation” [P4]. CPC the expert IR consultant in the steering group, advised this statement should be revised based on participant feedback and was changed to “If the patient’s blood pressure exceeds 160/100mmHG after conscious sedation and antihypertensive medications, postpone the procedure and seek a medical review.” CPC also advised this is not integral to the IR kidney biopsy procedure and if dissensus remained after the third round of data collection, this item could be removed. The updated item list presented in table 2, revised to include participant feedback, was sent to the participants in the third round.
Round 3.
Participants were presented with the revised competency list for final agreement and to capture outstanding feedback. Agreement was reached on 23 items. one outstanding item, item 12 (see Table 2), did not receive consensus and was removed. There was no additional free text feedback.
Results from each round of the modified Delph process and the amendments made at each stage are included in Appendix.
Simulation design.
AJD & CMC with the support of CPC, identified the procedure domains that could be incorporated into a simulation based educational training intervention, identifying the most effective simulation strategies, see Table 3.
Table 3: Simulation Strategies for each procedural domain.
Discussion
There is a need to train large numbers of radiologists to deliver radiology procedures. The UK and Ireland are experiencing a rising demand for well-trained radiologists to align staffing levels with European averages [1,5]. A 2017 report from the Royal College of Radiologists (RCR) indicated a widening gap between the supply and demand for radiology services. The shortage of 1,000 consultants in 2017 was projected to grow to approximately 1,600 consultants by 2022, posing a significant challenge to radiology services.
Radiology training currently follows the apprenticeship model, which requires significant resources, including mentored training time, may result in longer operative times, and has the potential harm to patients. Simulation-based medical education (SBME) successfully contributes to quality health professions education [14] and radiology training [15]. It is an effective approach to acquire, retain and transfer skills to clinical practice, at a minimum equivalent to that achieved through the traditional apprenticeship model [16]. SBME in radiology training is cost effective [17], improves trainee’ skills [18] and significantly improves patient outcomes through reduction in infections [19], fewer errors and less time on the procedure [20].
Many studies have reported positively on the role of SBME in sonography, noting the benefits of this type of training; the reduction of stress and risk to the patient and improvement in skill acquisition and procedural technique in an unpressurised or “lower stakes” environment [21,22]. In this lower stakes environment, SBME contributes to the psychological aspects of IR procedure performance, including increased confidence and reduced anxiety in trainees [23].
The goal is to prepare individuals not only for the specific context training but also to enable the transfer of acquired skills to real-world scenarios [24]. While the RCR IR curriculum includes simulation as a teaching and learning methodology [25], there is no guidance on how best to implement SMBE and what approaches should be considered.
The design and implementation of SBME should address the current training needs. Often individual clinical skills are developed in isolation on task trainers in low fidelity environments. Whole-task training recognizes that effective learning involves more than just mastering individual components in isolation. It emphasizes the interconnectedness of various skills and the need to develop a holistic understanding of tasks or challenges. We must consider the full spectrum of skills that are required, as opposed to those specifically related to model based procedural activities. It is specifically important in this context for radiology trainees who are intrinsically motivated to become clinically competent [26], and whole-task training will prepare trainees for their clinical role to meet the current staffing demand, and to provide the opportunity to practice and hone the full spectrum of skills associated with a procedure.
There are a range of strategies that can be incorporated into SBME interventions including part task simulation trainers to develop and hone specific technical components of clinical tasks, high-fidelity scenarios including multiple professionals, working with simulated participants to develop communication skills, and virtual and augmented reality training. Research suggests the benefit of whole-task training, especially in routine procedures such as kidney biopsy, when the discrete clinical steps are highly integrated [27]. Whole-task training is a comprehensive approach to learning that encompasses the integrated acquisition of knowledge, skills, and attitudes. In health professions education this method goes beyond isolated procedural skill development and focuses on the coordination of qualitatively different constituent skills.
Whole-task training and competency-based assessment in health professions education relies on simulation as an approximation of clinical practice in which to develop, hone and master procedural skills. A notable finding was the similarities in the descriptions of the procedure from all nine participants, which facilitated the initial identification of the 24 items. This suggests that whole-task training would be a suitable strategy for this type of training as the participants delineated discrete clinical steps that were highly integrated [27].
The main challenge associated with the consensus building activity in this study was related to individual organisational procedures and local practice. After three rounds of data collection, item 12 If the patient’s blood pressure exceeds 160/100mmHG after conscious sedation and antihypertensive medications, postpone the procedure and seek a medical review was removed from the itemised list as it had not reached the consensus threshold. Additionally, item 21 was revised to remove specific observation frequency and vital sign limits. While local context and adherence to local guidelines is an important aspect of training for IR trainees at a specific clinical site, ultimately these factors were deemed irrelevant to a national procedural description by the steering group.
Hybrid simulations, involving simulated participants and technology would facilitate whole-task training and an evaluation of competence. Hybrid simulations also emphasize the importance of all of the skills in a particular procedure; 1) those associated with the instruments and imaging technologies, and 2) those associated with patient consultation, interprofessional collaboration, communication and teamwork. The latter grouping of skills historically referred to as “bedside manner” is routinely taught in isolation during undergraduate training and is not routinely incorporated in training in clinical practice [28].
A limitation of the study was the potential gender bias associated with an all-male Delphi panel. The authors extended the initial recruitment period to try to include additional perspectives, however the documented gender imbalance in academic medicine, especially in procedure-oriented fields such as interventional radiology resulted in all male participants [29,30]. This study was also limited in that it was not designed to be an international survey, it was an all-Ireland survey to address a national need for formalised competency-based training. Finally, there was a low response rate to the survey, 21% of the network of Interventional Radiologists engaged with the consensus building activities. While this appears to be a low response rate, it is in line with surveys of this kind, and speaks to the demands and workload of the profession; the European Society of Radiology (ESR) and the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) developed an online survey in 2019, and the response rate was 8.3% [31].
Conclusion
In conclusion, this Delphi process has led to the identification of 23 competencies in a blueprint deemed essential for the development of a curriculum tailored to the training needs of radiologists performing ultrasound-guided renal biopsy. This blueprint offers a structured approach to integrating simulation-based education into radiology training programs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Marescaux J, Diana M. Inventing the future of surgery. World J Surg. 2014;39(3):615–22. doi: 10.1007/s 00268-014-2879-2 25413180 · doi ↗ · pubmed ↗
- 2Floridi C, Cellina M, Irmici G, Bruno A, Rossini N, Borgheresi A, et al. Precision Imaging Guidance in the Era of Precision Oncology: An Update of Imaging Tools for Interventional Procedures. J Clin Med. 2022;11(14).10.3390/jcm 11144028 PMC 932206935887791 · doi ↗ · pubmed ↗
- 3O’Neill WC. Renal relevant radiology: use of ultrasound in kidney disease and nephrology procedures. Clin J Am Soc Nephrol. 2014;9(2):373–81. doi: 10.2215/CJN.03170313 24458082 PMC 3913230 · doi ↗ · pubmed ↗
- 4Nayahangan LJ, Albrecht-Beste E, Konge L, BrkljačićB, Catalano C, Ertl-Wagner B, et al. Consensus on technical procedures in radiology to include in simulation-based training for residents: a European-wide needs assessment. Eur Radiol 2020 311 [Internet]. 2020 Jul 28 [cited 2021 Oct 9];31(1):171–80. Available from: https://link.springer.com/article/10.1007/s 00330-020-07077-010.1007/s 00330-020-07077-032725331 · doi ↗ · pubmed ↗
- 5Tibana TK, Adami V, Fornazari V, Gutierrez Junior W, Marchiori E, Szejnfeld D, et al. Interventional radiology in urology. Radiol Bras. Set/Out. 2019;52(5):331–6.10.1590/0100-3984.2018.0035 PMC 680861731656352 · doi ↗ · pubmed ↗
- 6Nayahangan LJ, Stefanidis D, Kern DE, Konge L. How to identify and prioritize procedures suitable for simulation-based training: Experiences from general needs assessments using a modified Delphi method and a needs assessment formula. Med Teach. 2018;40(7):676–83. doi: 10.1080/0142159 X.2018.1472756 29938547 · doi ↗ · pubmed ↗
- 7Nayahangan LJ, Konge L, Park C, Dubrowski A, Yudkowsky R. Development of a Rubric to Evaluate Implementation Quality of Simulation-Based Courses: A Consensus Study. Simul Healthc. 2023;18(6):351–8. doi: 10.1097/SIH.0000000000000684 36111989 · doi ↗ · pubmed ↗
- 8Khamis NN, Satava RM, Alnassar SA, Kern DE. A stepwise model for simulation-based curriculum development for clinical skills, a modification of the six-step approach. Surg Endosc. 2016;30(1):279–87. doi: 10.1007/s 00464-015-4206-x 25899812 · doi ↗ · pubmed ↗