Integra Dermal Regeneration Template in Reconstruction of Primary Oncologic Defects in the Lower Extremities: A Case Series
Katie Ross, Nicholas Zinck, David Wilson, Jack Rasmussen, Michael Biddulph, Jason Williams

TL;DR
This case series shows how a dermal regeneration template helps reconstruct complex leg defects after tumor removal, allowing for easier later revisions.
Contribution
The study demonstrates the novel use of IDRT in oncologic lower extremity reconstruction with uncertain tissue margins.
Findings
IDRT successfully facilitated neodermis growth to support skin grafting in all four cases.
Use of IDRT allowed surgical revision of positive margins without losing graft tissue in a single procedure.
Negative pressure wound therapy improved neodermis quality for skin graft acceptance.
Abstract
This article presents a case series of 4 patients who underwent primary reconstruction of oncologic defects in the lower extremities using Integra Dermal Regeneration Template (IDRT). The patients had either primary or recurrent tumors, which resulted in exposure of deep underlying structures including tendon, nerve, muscle, and bone. IDRT was selected to manage these defects due to the uncertain malignant potential of tissue margins and its ability to facilitate later margin revision without sacrificing tissue. The use of IDRT allowed for the growth of a neodermis that supported subsequent split-thickness skin grafting in all cases. Additionally, for those with positive margins, surgical revision and skin graft application was able to be performed in a single procedure, maximizing operating room use and patient convenience. This case series highlights the potential of IDRT in managing…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2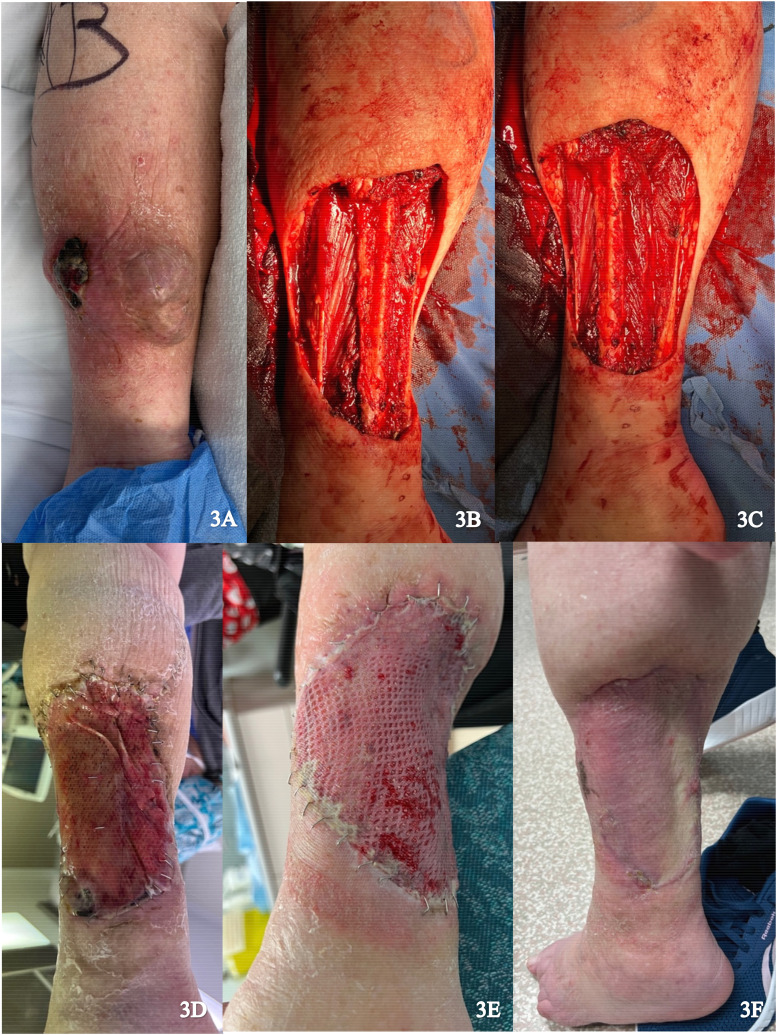 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReconstructive Surgery and Microvascular Techniques · Wound Healing and Treatments · Surgical Sutures and Adhesives
When faced with a challenging defect, the reconstructive surgeon has various closure techniques and materials available, ranging from the simple to the very complex. One unique option is Integra Dermal Regeneration Template (IDRT).^1,2^
The use of IDRT in reconstructive surgery has significantly expanded over the past decade with case reports describing its use in burn injuries, flap donor defects, and traumatic injuries.^1,3????????–12^ In some of these cases, the defects exposed deeper tissues such as muscle, tendon, and bone; despite this, positive outcomes were achieved.^5,11^ Traditionally, deep defects have required free autologous tissue transfer. While these remain a critical part of the reconstructive ladder, they are not without obstacles including flap failure, donor site morbidity, long operative times, and the need for a prolonged hospital stays for flap monitoring. Although there has been increased use of IDRT in recent years, there is a lack of literature assessing its benefit for reconstruction of oncologic defects exposing deep tissues in the lower extremities.
This article describes 4 cases in which IDRT has been used in the primary reconstruction of deep oncologic defects of the lower extremities with the aim of demonstrating the efficacy in this specific context.
A 41-year-old female presented with recurrence of a previously excised pleomorphic hyalinizing angiectatic tumor on the dorsum of the right foot. Re-excision was performed with circumferential dissection of the tumor, raising fascia and paratenon of extensor hallucis longus, with exposure of deep tissues (Figure 1A). Local skin advancement was performed to reduce the wound size and IDRT was applied (Figure 1B and C). The wound was sealed with a negative pressure wound therapy (NPWT). Formation of a neodermis was achieved 3 weeks following IDRT application (Figure 1D). Under local anesthetic, a spilt thickness skin graft (STSG) (0.0012 inches) measuring 8 × 10 cm was harvested from the right proximal thigh and secured to the wound after removal of the silicone layer (Figure 1E). NPWT was applied and there was complete graft take at 1 week. No complications were noted on follow up (Figure 1F).
A 56-year-old female presented with multifocal myxoinflammatory fibroblastic sarcoma of the medial right foot (Figure 2A). Resection was performed with neurolysis of the posterior tibial nerve and deep peroneal nerve, dissection of the posterior and anterior tibial arteries, and dissection of fascia and paratenon from surrounding structures (Figure 2B). Local tissue advancement was performed followed by IDRT application (Figure 2B and C). The wound was sealed with NPWT.
Approximately 2 weeks after the procedure, histopathology confirmed a positive posterior margin requiring revision. IDRT was continued as the patient indicated a strong preference to avoid flap surgery due to the potential donor site morbidity and the anticipated bulk of a flap that could interfere with wearing shoes. Revision of the positive margin, removal of the silicone layer, and application of an STSG (0.0012 inches) from the right lateral thigh was performed 5 weeks after the initial procedure (Figure 2E). The final wound size measured appropriately 18 × 8 cm. NPWT was applied and there was successful graft take at 1-week follow up (Figure 2F).
A 92-year-old female presented with a large myxofibrosarcoma on the posterior aspect of the left lower leg (Figure 3A). Excision of the tumor involved resection of portions of the medial gastrocnemius and soleus muscles. In addition, periosteum was dissected from the fibula and the peroneal nerve was exposed (Figure 3B and C). Muscle flaps were used to cover the exposed fibula and peroneal nerve and skin flaps were advanced to reduce wound size. IDRT was applied to the wound and sealed with NPWT (Figure 3D). Complete revascularization and formation of neodermis was achieved after 3 weeks, with exception of a small distal area. An STSG (0.0012 inches) was harvested from the left proximal lateral thigh and applied over the 10 × 15 cm wound after removal of the IDRT silicone layer (Figure 3E). NPWT was reapplied and there was complete graft take after 2 weeks (Figure 3F).
A 49-year-old male presented with a verrucous squamous cell carcinoma on the plantar aspect of the left foot (Figure 4A). Excision of the tumor resulted in exposure of the flexor tendons over the metatarsophalangeal joint capsule (Figure 4B). An IDRT sheet measuring 6 × 6 cm was applied over the wound (Figure 4C). The wound was sealed with an NPWT dressing and reapplied weekly (Figure 4D). Histopathology confirmed a close positive lateral margin. Four weeks later, the margin was revised and an STSG from the left thigh was applied to the neodermis following removal of the IDRT silicone layer (Figure 4E). NPWT was reapplied and there was 100% graft take after 1 week with no complications on follow up (Figure 4F).
We report a case series of 4 patients managed for reconstruction of primary oncologic defects of the lower extremities using IDRT. The patients range from 41 to 92 years of age with either primary growth or local recurrence of tumors in a variety of regions of the lower extremities.
In each of the cases presented, initial reconstruction utilizing IDRT was selected partly due to the unknown malignant potential of tissue margins. In contrast to a primary skin flap closure, initial management with IDRT allowed for later revision of positive margins without sacrificing graft or flap tissue, while at the same time allowing for growth of a neodermis capable of accepting an STSG. In each case, revision was able to be performed in the same procedure as final closure via skin grafting, minimizing patient inconvenience and use of operating room time.
The timing for removing the silicone layer is typically between 3 to 4 weeks, based on neodermis formation.^ 13 ^ In our case series, 3 patients were ready for skin grafting within this time frame, whereas 1 patient required prolonged grafting until an appropriate wound bed had formed. When managing these patients, our experience showed that the NPWT dressing is an important adjunct in achieving good results. NPWT dressings were used throughout the entire process and were changed at weekly appointments which also allowed for frequent assessment of neodermis formation. Splinting was not routinely required but was considered in cases where joint motion could interfere with graft adherence and cause shearing.
In all cases, tumor excision resulted in exposure of deep structures. NPWT has been used alone to manage wounds by removing excess fluid, enhancing angiogenesis, and fibroblast migration.^ 14 ^ While this process can facilitate formation of granulation tissue matrix, it typically is not be placed it directly on exposed tendon, bone, or nerve.^15,16^ In these situations, using a dermal regeneration template like Integra can provide a layer that provides protection and is effective in regenerating tissue that can accept a delayed skin graft. In our cases, combining the 2 was considered superior to using either alone for complex wounds with exposed deep structures.
IDRT is a commercially available product with significant costs, varying based on size. Institutions should account for this when considering IDRT in their reconstructive algorithm. Handling and storage guidelines recommend maintaining the product in a temperature-controlled environment and ensuring proper hydration before application.^ 17 ^
The reconstructive surgeon has many considerations when faced with challenging defects. The choice of reconstructive technique will depend on the nature of the defect, available donor sites, and patient factors. With the successful use of IDRT in complex oncologic defects, we identify another viable option to add to the list of available techniques.
Supplemental Material
sj-docx-1-psg-10.1177_22925503251336254 - Supplemental material for Integra Dermal Regeneration Template in Reconstruction of Primary Oncologic Defects in the Lower Extremities: A Case SeriesSupplemental material, sj-docx-1-psg-10.1177_22925503251336254 for Integra Dermal Regeneration Template in Reconstruction of Primary Oncologic Defects in the Lower Extremities: A Case Series by Katie Ross, Nicholas Zinck, David Wilson, Jack Rasmussen, Michael Biddulph and Jason Williams in Plastic Surgery
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rehim SA Singhal M Chung KC . Dermal skin substitutes for upper limb reconstruction. Hand Clin. 2014;30(2):239–252. doi:10.1016/j.hcl.2014.02.00124731613 PMC 4158916 · doi ↗ · pubmed ↗
- 2Chang DK Louis MR Gimenez A Reece EM . The basics of Integra dermal regeneration template and its expanding clinical applications. Semin Plast Surg. 2019;33(03):185–189. doi:10.1055/s-0039-169340131384234 PMC 6680073 · doi ↗ · pubmed ↗
- 3Pilkington RJJ Bhatia SK . Acellular dermal regenerative matrix material “Integra TM” as an adjunct for radial forearm free flap donor site closure. Br J Oral Maxillofac Surg. 2020;58(6):726–727. doi:10.1016/j.bjoms.2020.01.03432409130 · doi ↗ · pubmed ↗
- 4Roels N Van den hof B . Integra ® dermal regeneration template as an alternative technique to treat degloving injury of fingers. Acta Chir Belg. Published online June 28. 2023:586–5588. doi:10.1080/00015458.2022.209355935762177 · doi ↗ · pubmed ↗
- 5Shah A Taupin P . Single-stage extremity reconstruction through the use of dermal matrices: The power of Integra ® bilayer wound matrix in the face of medical comorbidities, patient preference and non-compliance. Case Rep Plast Surg Hand Surg. 2022;9(1):75–83. doi:10.1080/23320885.2022.2047052 PMC 892882035308805 · doi ↗ · pubmed ↗
- 6Patel KB Williams JV Baxter EM Chengot P Parmar JD . Surgical management of advanced pleomorphic dermal sarcoma of the occipital scalp. Ann R Coll Surg Engl. 2022;104(1):e 9–e 11. doi: 10.1308/rcsann.2021.0052 PMC 1033524834730407 · doi ↗ · pubmed ↗
- 7Mogedas-Vegara A Agut-Busquet E Yébenes Marsal M Luelmo Aguilar J Escuder de la TorreÒ . Integra as firstline treatment for scalp reconstruction in elderly patients. J Oral Maxillofac Surg. 2021;79(12):2593–2602. doi:10.1016/j.joms.2021.07.00934391723 · doi ↗ · pubmed ↗
- 8Romano G Bouaoud J Moya-Plana A Benmoussa N Honart JF Leymarie N . Integra® dermal regeneration template for full thickness carcinologic scalp defects: our 6 years’ experience retrospective cohort and literature review. J Stomatol Oral Maxillofac Surg. 2021;122(3):256–262. doi:10.1016/j.jormas.2020.06.01632629168 · doi ↗ · pubmed ↗