Recurrent MDM2 Amplification in the Spectrum of HMGA2-Altered Pleomorphic Adenoma, Atypical Pleomorphic Adenoma and Carcinoma Ex Pleomorphic Adenoma
Kimberly S. T. Burghout, G. E. Breimer, S. Koppes, H. M. Hazelbag, M. L. Ooft, G. M. Raicu, A. M. Cleton-Jansen, T. van Wezel, R. van Eijk, D. Terlouw, S. L. van Egmond, V. T.H.B.M. Smit, N. J. Rupp, D. Cohen

TL;DR
This study finds that MDM2 amplification is more common in HMGA2-altered pleomorphic adenomas that progress to cancer, suggesting a role in malignant transformation.
Contribution
The study identifies a link between MDM2 amplification and malignancy in HMGA2-altered pleomorphic adenomas.
Findings
MDM2 amplification was present in 78% of carcinoma ex pleomorphic adenoma cases.
MDM2 amplification was enriched in HMGA2-altered pleomorphic adenomas compared to benign PLAG1-altered neoplasms.
MDM2 analysis could help confirm malignancy in HMGA2-altered cases with cytonuclear atypia.
Abstract
Pleomorphic adenoma is the most common neoplasm of the salivary glands. While the overall risk of malignancy is relatively low, a distinct molecular sub-group harboring HMGA2 alterations seems to show an increased risk of malignant progression to carcinoma ex pleomorphic adenoma. This study investigates MDM2 amplification in HMGA2-altered pleomorphic adenoma, atypical pleomorphic adenoma, and carcinoma ex pleomorphic adenoma. In this multicenter, retrospective case series analysis, we examined 37 cases of HMGA2-altered pleomorphic adenoma, carcinoma ex pleomorphic adenoma, and pleomorphic adenoma with atypical features. A total of 18 cases were included from our institutional archives, with 19 additional cases derived from published literature. The cases from our institutes were analyzed for MDM2 amplification using a stepped approach by immunohistochemistry and FISH. Collectively,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
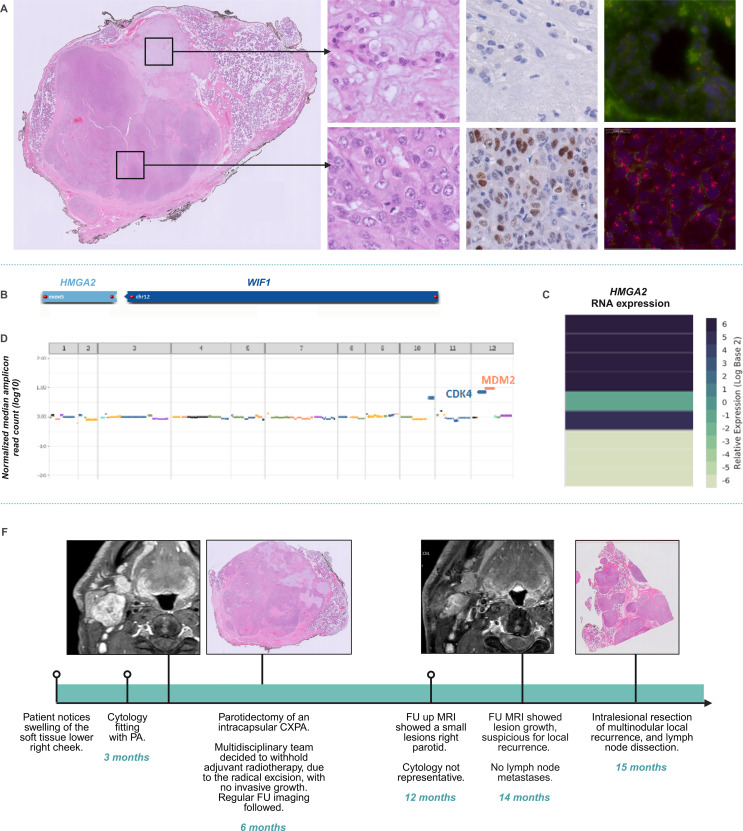 Figure 1
Figure 1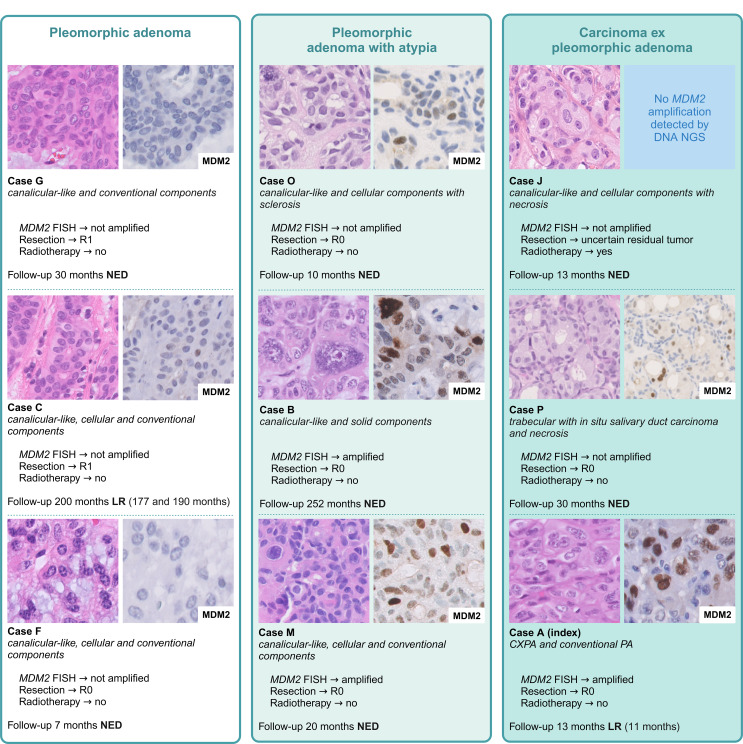 Figure 2
Figure 2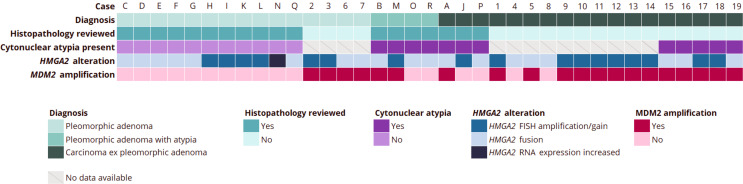 Figure 3
Figure 3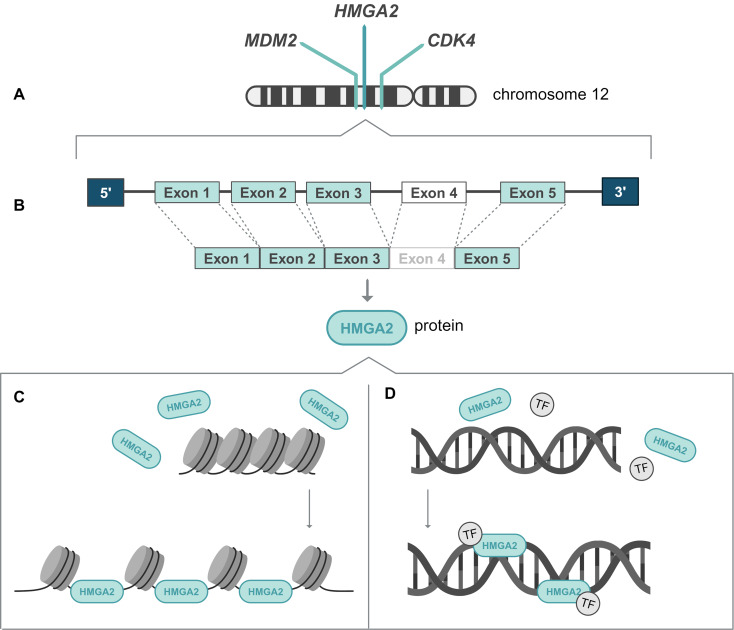 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalivary Gland Tumors Diagnosis and Treatment · Ear and Head Tumors · Oral and Maxillofacial Pathology
Introduction
Pleomorphic adenoma (PA) and carcinoma ex pleomorphic adenoma (CXPA) are characterized by translocations involving the HMGA2 and PLAG1 genes [1–3]. Progression to CXPA occurs in approximately 1.5–9.5% of PA [4, 5]. However, recent findings in small case series indicate that PA harboring HMGA2::WIF1 translocations seem to have a higher rate of regional recurrence, metastasis, and malignant transformation [6]. The observed higher rate of adverse clinical outcomes in these neoplasms calls for routine investigation and recognition by pathologists. However, most pathology laboratories do not have (unlimited) access to FISH and/or RNA-NGS analysis to identify HMGA2 alterations. Several studies have described morphological features that could characterize HMGA2-altered neoplasms. Firstly, Agaimy et al. observed a distinct canalicular adenoma-like growth pattern in HMGA2-altered PA [7]. Though potentially helpful in identifying HMGA2-altered lesions, the growth pattern itself is not necessarily indicative of unfavorable biological behavior, as the described neoplasms were benign and limited follow-up data to observe local recurrence was available.
More recently, Alsugair et al. reported four (intracapsular) CXPA with HMGA2 alterations showing striking cytonuclear atypia [8]. Besides the recurrent morphological feature of cytonuclear atypia, these lesions all showed MDM2 amplifications. The co-amplification of MDM2 has been described previously in salivary gland neoplasms by Persson et al., identifying MDM2 as an amplification target in both PA and CXPA [8]. In neoplasms originating from other tissues (e.g. liposarcoma) HMGA2 alteration and MDM2 amplification have also been described [9, 10]. The question arises whether MDM2 analysis could serve as a similar, widely accessible marker for identifying HMGA2-altered PA with unfavorable biological behavior.
In this study we aim to describe the relationship between HMGA2-altered lesions and MDM2 amplification in a cohort of PA, atypical PA and CXPA, in a large case series derived from our institutional archives and published literature. Additionally, by highlighting morphological (e.g. striking cytonuclear atypia), immunohistochemical, and molecular characteristics of HMGA2-altered salivary gland tumors, we strive to facilitate recognition in daily diagnostic practice. To illustrate the diagnostic and clinical challenges posed by HMGA2-altered neoplasms neoplasms, we first present an index case involving an HMGA2 alteration and MDM2 co-amplification.
Index Case
A 52-year-old male presented with a lesion in the right parotid gland, reporting a minimal progression in size over time. The patient had no relevant medical history and is a never-smoker. Magnetic resonance imaging revealed a solitary, well-defined lesion of 34 mm in the deep parotid lobe. There was no clinical evidence of lymph node or distant metastases. Cytological analysis of the lesion showed a background of myxoid matrix containing grouped and individually organized cells without cytonuclear atypia, consistent with PA. Subsequent histopathological analysis of the parotidectomy specimen revealed a sharply demarcated, mostly encapsulated, multi-lobular lesion with capsular invasion and two morphological components. Firstly, the hypocellular component of the lesion consisted of chondromyxoid stroma, uniform spindle cells, and uniform epithelial cells arranged in fields and glandular structures. Secondly, the predominant component of the lesion consisted of a hypercellular population of epithelial cells with enlarged, irregularly shaped nuclei with prominent nucleoli and substantial eosinophilic cytoplasm, in a background of thick hyalinized stroma. In this component, there was increased mitotic activity, including atypical mitoses, and areas of necrosis. Immunohistochemical analysis confirms the biphasic architecture of the lesion, with the epithelial cells expressing keratin AE1/AE3 and keratin 7 and the myoepithelial cells expressing S100, calponin and p63. In the hypercellular component of the lesion, a more variable staining pattern was observed with a partially retained biphasic immunohistochemical pattern and areas of myoepithelial differentiation. Ki-67 showed a proliferation rate of 1–2% in the conventional component and an increased proliferation rate of up to 20% in the hypercellular component, showing striking cytonuclear atypia. No invasive growth in surrounding salivary gland tissue was observed, and no perineural or vascular invasion was found. Molecular analysis was performed using fusion-analysis (Archer FusionPlex USZ Zurich Salivary Gland Panel v2 [11]), detecting the same HMGA2(exon 5)::WIF1(intron 2) fusion in both the conventional and atypical component. The re-arrangement involved a full-length HMGA2 gene, fused to an inversed intronic sequence of WIF1, resulting in an overexpression of the HMGA2 gene. Next Generation Sequencing (NGS AmpliSeq LUMC Cancer Hotspot Panel version 6) of the isolated DNA of the atypical component showed no pathogenic variations (e.g. TP53 mutation) but copy number variation analysis revealed the presence of MDM2 and CDK4 co-amplification. The MDM2 amplification in the atypical component was visualized using immunohistochemistry, showing no staining in the conventional component and strong nuclear expression in the atypical component. Amplification was confirmed by MDM2 FISH analysis. Based on the prominent atypical component with increased mitotic activity, the multi-lobular growth and the molecular findings, the lesion was classified as an intracapsular CXPA. Eleven months after the complete resection with a 1 mm margin, the patient developed multinodular local disease recurrence that was surgically resected with positive margins. The case, including the timeline, is highlighted in Fig. 1.
Fig. 1. Index case. (A) Representative H&E slides with an overview of the lesion, and detailed images of conventional and atypical components, followed by the immunohistochemistry of MDM2 and MDM2 FISH analysis in both components. (B) The HMGA2::WIF1 fusion as analyzed by the Archer FusionPlex USZ Zurich Salivary Gland Panel v2 [11]. (C) The HMGA2 gene expression is depicted in a heatmap, showing an overexpression (dark blue). (D) The copy number variation analysis of the atypical component showed amplification of MDM2 and CDK4. (E) A timeline provides the details on the clinical course of the index case, highlighting the lesion’s recurrence within a year of the primary resection
Materials and Methods
Literature Case Selection
The literature study followed the PRISMA guideline for systematic reviews [12]. An inquiry of the PubMed database was performed using search terms related to “pleomorphic adenoma”, “carcinoma ex pleomorphic adenoma”, “salivary gland”, “HMGA2” and “MDM2”. Abstracts of the retrieved articles were screened and selected for full-text review when describing cases of adults with HMGA2 rearranged salivary gland neoplasms. For the final selection, the following exclusion criteria were used: (1) lack of essential clinical and pathological details (e.g. histopathological diagnosis), (2) outdated molecular analysis (e.g. karyotyping), and (3) metastases of carcinoma ex pleomorphic adenoma. Cases published multiple times were included only once in the case series. Eligible study designs for this literature analysis included case-control series, case reports, cohort studies, and cross-sectional studies. A database was composed of the HMGA2-rearranged, MDM2-analyzed PA and CXPA described in literature, detailing patient sex, age, and histopathological diagnosis. When available the details on tumor location, size, morphology, and follow-up were also collected. The histological diagnosis of literature-derived cases was not reviewed due to limited availability histological images.
Case Series Analysis
Medical ethical approval was granted by the ethics committee Leiden-Den Haag-Delft. Due to the retrospective design of the study, informed consent was waived. However, written informed consent was obtained from the patient described in the index case. Clinical details, including age, sex, lesion size and location, and molecular characteristics, were collected. All specimens were routinely processed using formalin-fixation and paraffin embedding (FFPE) for histopathological and molecular analysis, and data was collected retrospectively. In addition to the index case, PA, atypical PA and CXPA with known HMGA2 alterations were retrospectively selected and included from six hospitals (Leids Universitair Medisch Centrum, Universitair Medisch Centrum Utrecht, Erasmus Medisch Centrum Rotterdam, Rijnstate Ziekenhuis Arnhem, St. Antonius Ziekenhuis Utrecht and Gelre Ziekenhuis Apeldoorn). The final diagnosis was made according to the definitions of the WHO Head and Neck Tumours classification (5th edition). Distinguishing between an atypical PA and an intracapsular CXPA remains a challenge, as a universally accepted diagnostic definition has yet to be established. The literature describes several histomorphological, immunohistochemical and molecular features of the often cellular, non-invasive lesions with potentially different biological behavior [13–15]. Based on these descriptions the following definitions were applied in this study: atypical PA were defined as lesions showing significant cytonuclear atypia, not reaching the extend of cytonuclear atypia observed in CXPA, with preserved architecture of layered ductal and myoepithelial components. Additionally, lesions showed no worrisome immunohistochemical or molecular features such as p53 mutation or HER2 amplification. Lesions with significant cytonuclear atypia, increased mitotic activity (typically > 2 per 10HPF, abnormal mitotic figures, high proliferation index in ki67), areas of disturbed architecture and/or presence of a distinct malignant component, were classified as intracapsular CXPA. These lesions were reviewed independently by two experienced Head and Neck pathologists (DC, NJR, GEB),
Immunohistochemistry
Immunohistochemical analysis for MDM2 was performed on 3-µm thick FFPE sections, automatically stained with the MDM2 monoclonal IF2 antibody clone on the Dako Omins stainer in Leiden University Medical Center. The remaining cases were analyzed by immunohistochemical staining for MDM2 (Invitrogen, clone IF-2), conducted using a pretreatment protocol involving 24 min of CC1 buffer, followed by a 32-minute incubation with the primary antibody and staining carried out on the Ventana Benchmark Ultra platform. Two observers reviewed the MDM2 staining (KSTB and DC). When possible, all cases were additionally analyzed for MDM2 amplification using MDM2 FISH or NGS Cancer Hotspot analysis. As a control group, 12 cases of PA, atypical PA and CXPA with known PLAG1 fusion were also analyzed using MDM2 immunohistochemistry, followed by FISH analysis if any amount of nuclear staining was present.
FISH Analysis
In Leiden, the MDM2 FISH was performed on FFPE sections of 4µM, processed using the Vysis MDM2/CEP12 FISH probe to confirm MDM2 amplification, and FISH was performed using the Histology Fish Accessory Kit (Dako, Glostrup, Denmark) as per the manufacturer’s description. Nuclei were counterstained with 10 µl of 4′,6-diamidino-2-phenylindole (DAPI). The FISH for MDM2 and HMGA2 performed elsewhere used the Zytovision probe kit (Zytovision.GmbH, Bremerhaven, Germany), as per the manufacturer’s description.
Molecular Analysis
HMGA2 alterations were detected using RNA sequencing. RNA was extracted from FFPE blocks, and samples were analyzed using the SalvGlandDx RNA Fusion Panel on the Illumina MiSeq system [11]. Additional analysis of MDM2 amplification was performed on DNA isolates using the in-house developed NGS Ampliseq Cancer Hotspot Panel on the Genexus Ion Torrent S5 platform (Thermo Fisher Scientific, Canada).
Statistical Analysis
Statistical analysis was performed using IBM SPSS software (version 29). The PA-group and CXPA-group were compared on MDM2 status using the Fishers’ exact test. The atypical PA were excluded from the analysis due to the uncertain biological behavior and small sample size. Statistical significance was set at a p-value of < 0.05. To assess the strength of the association between MDM2 amplification and malignant histopathological diagnoses in the HMGA2-altered lesions, the odds ratio (OR) was calculated. For this, PA with atypical features were included in the benign category. Additionally, a logistic regression analysis was performed to assess whether histological diagnosis (benign/malignant) and MDM2 amplification status were associated with the occurrence of a clinical event (e.g. local recurrence, metastasis, malignant transformation). For the logistic regression and OR analysis, PA with atypical features were included in the benign category.
Results
Literature Cases
From the literature search a total of five studies detailing 19 cases of HMGA2-altered, *MDM2-*analyzed salivary gland neoplasms were included [6, 8, 16–18]. The studies were published between 1998 and 2024. Various molecular investigations were used, including NGS analysis, RNA sequencing, MDM2 FISH analysis, array-comparative genomic hybridization (aCGH), and Southern blot analysis. Further case-specific characteristics are described in the next Sect. (4.2 case series analysis).
Case Series Analysis
Clinical and Demographic Features
Retrospectively an additional 18 cases with HMGA2 alteration were identified from six different hospitals. Combining the cases derived from literature and the additional cases from our clinical practice, a total of 37 HMGA2-altered salivary gland neoplasms analyzed for MDM2 amplifications were collected for this analysis. The cohort included 24 female patients (65%) and 13 male patients (35%), with ages ranging from 25 to 86 years old (mean 62 years) at the time of diagnosis. A total of 31 lesions derived from the parotid gland (84%), 2 from the parapharyngeal space (5%), one from the hard palate (3%), one from the mandibular tonsil lodge (3%), and one of unknown origin (3%). The lesion size varied between 7 and 53 mm (mean 25 mm). Among the cohort, there were 15 pleomorphic adenomas, 4 pleomorphic adenomas with atypical features, 1 intracapsular carcinoma ex pleomorphic adenoma, 1 carcinoma ex pleomorphic adenoma with minimal invasion, and 16 carcinoma ex pleomorphic adenoma. An overview of patient and lesion characteristics can be found in Table 1.
Table 1. Characteristics of 37 HMGA2-altered cases from literature and clinical practice with investigated MDM2 statusCaseAgeGenderLocationHistopathological diagnosisSubtype / growth patternHMGA2 alterationHMGA2 analysisMDM2 amplificationMDM2 analysis A52MParotid glandCXPA intracapsularepithelial-myoepithelial carcinoma HMGA2::WIF1 RNA-NGSYesFISHB32FParotid glandPA atypical featurescanalicular-like with solid areas HMGA2::WIF1 RNA-NGSYesFISHC75MMandibula tonsilPAsolid HMGA2::WIF1 RNA-NGSNoFISHD80MParotid glandPAcanalicular-like HMGA2::RAP1B RNA-NGSNoDNA-NGSE77MParotid glandPAcanalicular-like HMGA2::WIF1 RNA-NGSNoDNA-NGSF71MParotid glandPAtrabecular HMGA2::WIF1 RNA-NGSNoFISHG42MParotid glandPAcanalicular-like with conventional component HMGA2::WIF1 RNA-NGSNoFISHH68FParapharyngealPAcanalicular-like with conventional and solid componentHMGA2 lossFISHNoFISHI53FParotid glandPAcanalicular-likeHMGA2 ampl.FISHNoFISHJ76FParotid glandCXPA minimal invasionsalivary duct carcinomaHMGA2 ampl.FISHNoDNA-NGSK68FParapharyngealPAcanalicular-like with conventional componentHMGA2 ampl.FISHNoFISHL72MParotid glandPAcanalicular-likeHMGA2 ampl.FISHNoFISHM76FPalatum durumPA atypical featurescanalicular-likeHMGA2 ampl.FISHYesFISHN80MParotid glandPAcanalicular-likeHMGA2 RNA overexpressionRNA-NGSNoIHCO54FParotid glandPA atypical featurescanalicular-like with solid component and sclerosis HMGA2::WIF1 RNA-NGSNo (single cells)FISHP70MParotid glandCXPAsalivary duct carcinoma HMGA2::FLJ41278 RNA-NGSNo (single cells)FISHQ41FParotid glandPAconventional with sclerosis HMGA2::WIF1 RNA-NGSNoIHCR69MParotid glandPA atypical featuresin situ salivary duct carcinoma HMGA2::FLJ41278 RNA-NGSNo (single cells)FISH125 F
NDA CXPA NDA HMGA2 ampl./gainaCGHYesFISH255FParotid glandPA NDA HMGA2 ampl./gainFISHYesFISH385FParotid glandPA NDA HMGA2 ampl./gainFISHYesFISH486FParotid glandCXPA NDA
HMGA2::WIF1 RT-PCRNoFISH576MParotid glandCXPA NDA
HMGA2::WIF1 RT-PCRYesFISH674FParotid glandPA NDA
HMGA2::WIF1 RT-PCRYesFISH737FParotid glandPA NDA
HMGA2::WIF1 aCHGYesFISH873MParotid glandCXPA NDA
HMGA2::WIF1 RT-PCRNoFISH935FParotid glandCXPA NDA HMGA2 ampl./gainFISHYesFISH1040FParotid glandCXPA NDA HMGA2 ampl./gainFISHYesFISH1170FParotid glandCXPA NDA HMGA2 ampl./gainFISHYesFISH1269MParotid glandCXPA NDA HMGA2 ampl./gainFISHYesFISH1366FParotid glandCXPA NDA HMGA2 ampl.DNA-NGSYesDNA-NGS1430FParotid glandCXPA minimal invasion NDA HMGA2 ampl.DNA-NGSYesDNA-NGS1532FParotid glandCXPAhypercellular and monomorphic HMGA2::GRIP1 RNA-NGSYesFISH1651FParotid glandCXPAhypercellular and eosinophilic HMGA2::PLXNC1 RNA-NGSYesFISH1789FParotid glandCXPAconventional with infiltrationHMGA2 ampl.IHCYesFISH1867FParotid glandCXPAhybrid with infiltrationHMGA2 ampl.IHCYesFISH1960FBuccal mucosaCXPAbasaloid features HMGA2::WIF1 RNA-NGSYesDNA-NGSPA = pleomorphic adenoma, CXPA = carcinoma ex pleomorphic adenoma, NDA = no data available, NGS = Next Generation Sequencing, FISH = Fluorescence In Situ Hybridization, aCGH = arary Comparative Genomic Hybridization,* PCR = Polymerase Chain Reaction*
Follow-up and survival data were collected when available, with FU ranging between 5 and 854 months in PA, 1-252 months in PA with atypical features and 4-192 months in CXPA [6, 8, 16]. Adverse outcomes (local recurrence, metastases, death due to the disease) were reported in 4 of 37 cases. Case A (CXPA with MDM2 amplification) showed local recurrence 11 months after the primary radical resection. Case C (PA without MDM2 amplification) showed LR after a primary R1 resection. Case 8 (CXPA without MDM2 amplification) showed LR. Case 19 (CXPA with MDM2 amplification) showed LR after 5 months, distant metastasis after 31 months, and death due to the disease after 73 months. A complete overview of follow-up and survival data can be found in Table 2.
Pathological Features
Within the cohort there were 15 PA, 4 PA with atypical features, and 18 CXPA. The PA showed morphological variety with conventional chondromyxoid stroma, with varying cellular solid growth, trabecular and canalicular-like growth. Immunohistochemically, the lesions showed a bilayered architecture, with an inner epithelial cell layer and outer myoepithelial cell layer. In one case (case Q), cytonuclear atypia was seen in a background of extensive regressive changes, without other malignant features. The histological type of the malignant component of CXPA included epithelial-myoepithelial carcinoma and salivary duct carcinoma. Four PA with atypical features were included, showing some cytonuclear atypia and uncertain invasive growth, insufficient for a diagnosis of CXPA. In case R, a small 7 mm lesion showed invasive growth and in situ salivary duct carcinoma. An overview of the H&E, histological sub-type/growth pattern, MDM2 staining pattern, MDM2 amplification, and molecular alteration of cases A-R can be found in Supplementary Fig. 1. In the PLAG1-altered control group of 12 PA, PA with atypia and CXPA there was no immunohistochemical staining of MDM2, as can be seen in Supplementary Fig. 2.
Table 2. Follow-up and survival dataCaseHistopathological diagnosisMDM2 amplificationFollow-up (months)SurvivalDetailsACXPA intracapsularYes13LRLR (multi-nodular) at 11 monthsBPA atypical featuresYes252NED-CPANo200LRLR (multi-nodular) 2x at 177 and 190 monthsDPANo10NED-EPANo11NED-FPANo6NED-GPANo30NED-HPANo18DOCLiver cancerIPANo NDA
NDA
NDA JCXPA minimal invasionNo13NED-KPANo19NED-LPANo26NED-MPA atypical featuresYes20NED-NPANo12NED-OPA atypical featuresNo10NED-PCXPANo30NED-QPANo5NED-RPA atypical featuresNo1NED-1CXPAYes NDA
NDA
NDA 2PAYes204NED-3PAYes854DOC-4CXPANo60NED-5CXPAYes36DOC-6PAYes36NED-7PAYes36NED-8CXPANo84LRLocal recurrence9CXPAYes156NED-10CXPAYes72NED-11CXPAYes192NED-12CXPAYes96DOC-13CXPAYes NDA
NDA
NDA 14CXPAYes NDA
NDA
NDA 15CXPAYes5NED-16CXPAYes4NED-17CXPAYes5NED-18CXPAYes4NED-19CXPAYes73DODLR 5 months, metastases 31 months, DOD 73 monthsPA = pleomorphic adenoma, CXPA = carcinoma ex pleomorphic adenoma, NDA = no data available, NED = no evidence of disease, LR = local recurrence, DOC = died of other causes, DOD = died of disease, AWDM = alive with distant metastases
Molecular Analysis
Molecular analysis showed 19 cases with a confirmed HMGA2 rearrangement, paired with a variety of fusion partners, including WIF1 (n = 14), RAP1B (n = 1), FLJ41278 (n = 2), GRIP1 (n = 1), and PLXNC1 (n = 1). Case N showed increased RNA expression of HMGA2 without a confirmed fusion. Two cases showed immunohistochemical overexpression of HMGA2 without a confirmed fusion [16]. Six cases showed a break apart signal of HMGA2 in FISH analysis. The remaining nine cases showed amplification or gain of HMGA2.
Fig. 2. An overview of nine cases, showing the morphological spectrum of benign, atypical and malignant HMGA2-altered cases analyzed for MDM2 amplification and providing additional data on the residual tumor classification, radiotherapy, follow-up and survival. Additional high power images of all nine cases can be found in Supplementary Fig. 3
MDM2 amplification was present in 20 of 37 cases (54%); respectively in 4 of 15 PA (27%), in 2 of 4 PA with atypical features (50%), and in 14 of 18 CXPA (78%) (p-value 0.003). The odds ratio OR was 7.6, indicating a strong association between a malignant histopathological diagnosis and the presence of MDM2 amplification. However, further logistic regression analysis showed a non-significant association between clinical outcome event and MDM2 amplification (OR = 2.16; 95% CI, 0.20-22.96; p-value 0.522), and a non-significant association between clinical outcome event and malignant classification (OR = 0.17; 95% CI, 0.01–2.31; p-value 0.183).
Example cases of benign, atypical, and malignant cases with the MDM2 immunohistochemical staining pattern and clinical data can be found in Fig. 2. Three cases (case O, P and R) showed MDM2 immunohistochemical positivity of single atypical cells, in which MDM2 amplification could not be confirmed by FISH analysis. Similar to the index case, some cases in literature showed amplification of both MDM2 and CDK4. A schematic representation of all cases can be found in Fig. 3.
Fig. 3A schematic overview of all n = 37 cases included in the case series anlaysis, detailing the final histopathological diagnosis, the presence of cytonuclear atypia, the detected HMGA2 alteration and the presence of the MDM2 amplification. The histopathological diagnosis of cases derived from the literature was not reviewed
Discussion
This retrospective, multicenter case series analysis combines 18 cases from our clinical practice with an additional 19 cases from the literature, providing a cohort of 37 benign, intermediate, and malignant HMGA2-altered salivary gland neoplasms analyzed for MDM2. We found an MDM2 amplification in 27% of the PA, as opposed to 78% of the CXPA (p-value 0.003). This finding highlights the correlation between HMGA2 alteration and MDM2 amplification in salivary gland neoplasms, as has been described in other neoplasms (e.g. well-differentiated and dedifferentiated liposarcoma, rhabdomyosarcoma, lipoma, uterine leiomyoma, spindle cell sarcoma) [19–23].
Due to the enriched presence of MDM2 amplification in CXPA with HMGA2 alteration, recognition of this molecular sub-group of salivary gland neoplasms could be potentially informative in the pathologists’ assessment. Previous studies have indicated potential morphological clues like the presence of cytonuclear atypia and a canalicular-like growth pattern [7, 16]. In the current analysis, PA with a HMGA2 fusion often showed a cellular morphology, sometimes with canalicular, trabecular and/or conventional PA growth pattern (Supplementary Fig. 1). Notably, canalicular-like architecture was a common but not an exclusive morphological feature in this case series (canalicular-like growth in 11 of 18 HMGA2-altered lesions versus 1 of 12 PLAG1-altered lesions) and should therefore be used with care when identifying HMGA2-altered lesions.
Cytonuclear atypia, described by Alsugair et al. (2024) in CXPA was a more reproducible feature in this analysis, potentially indicating an underlying MDM2 amplification [16]. Interestingly, in the PLAG1 control group, a mix of both benign, intermediate, and malignant lesions, no immunohistochemical positivity for MDM2 was found, despite the occasional presence of cytonuclear atypia (Supplementary Fig. 2). This suggests that MDM2 immunohistochemical positivity may be a potential diagnostic feature for identifying the underlying HMGA2 alterations in PA and CXPA. However, when suspected, MDM2 amplification should be evaluated using FISH. Like analysis of Human Epidermal growth factor Receptor 2 (HER2), Androgen Receptor (AR) and p53 staining, MDM2 analysis could be added to the pathologists’ toolbox for difficult to classify salivary gland neoplasms, as a surrogate for the underlying molecular alteration [24–26]. Although MDM2 amplification was more frequently observed in HMGA2-altered PA with atypia and CXPA, our clinical outcome data, albeit limited, do not show a different clinical outcome in these tumors. With exception of the index case, in most cases, including in the MDM2-amplified tumors, no local recurrence or other adverse clinical outcome was observed. Therefore it is important to note that while MDM2 analysis may serve as a helpful tool in explaining cytonuclear atypia, it should not be interpreted as a definitive marker of malignancy or poor prognosis at this point. Conversely, a lack of MDM2 amplification may further reassure the pathologist when they are faced with a diagnostically challenging case, as it supports a benign classification.
In this analysis the consequence for PA with atypical features and the relevance of MDM2 amplification remains unclear. We included four PA with striking atypical features (case B, M, O and R) lacking invasive growth after extensive tissue sampling. This could be interpreted as lesions potentially transitioning from benign to malignant neoplasms. Case B and M showed cytonuclear atypia and MDM2 amplification, with no evidence of disease after extensive follow-up periods of respectively 252 and 20 months. Case O and R, showed cytonuclear atypia with staining of single, atypical cells in MDM2, with no proven MDM2 amplification and no evidence of disease after respectively 10 months and 1 month. However, immunohistochemical expression could certainly be indicative of otherwise altered signaling pathways independent of amplification [27]. The limited number of cases did not allow further interpretation of the implication of MDM2 amplification in the atypical but not overt malignant lesions. Strikingly, however, nuclear staining of single, atypical cells was observerd in case O and Case R. In the PLAG1 control group no staining of MDM2 staining of single atypical cells was encountered, emphasizing the connection between HMGA2 alteration and MDM2 amplification in PA. For daily practise, this implies, that despite atypical features and MDM2 expression and/or amplification, the growth pattern and cytology still remain the primary diagnostic criteria of CXPA.
The exact relationship between MDM2 and HMGA2 alterations in salivary gland neoplasms remains unclear, however, we propose a potential mechanism. The HMGA2 gene is located on the long arm of chromosome 12 and consists of five exons, of which the first three exons encode for an adenine-thymine (AT)-hook binding domain that enables the HMGA2 protein to interact with the minor grooves of the DNA. Physiologically the gene is expressed during early life, with a role in DNA repair by facilitating the binding of transcription factors and altering the chromatin structure (Fig. 4) [28]. Rearrangement of HMGA2 is suggested to drive tumorigenesis by the (dis-)regulatory effect of the HMGA2 protein on PLAG1 and IGF2 expression, a suggestion based on the downregulation of IGF2 expression in patients with Silver-Russel syndrome. This syndrome involves mutations in HMGA2 or the HMGA2 regulated gene PLAG1 [3]. The observed coamplification of MDM2 in HMGA2-rearranged PA and CXPA may result from the ability of the HMGA2 protein to alter chromatin structure, thereby increasing chromosomal instability with subsequent DNA fragmentation, inaccurate repair, and gene amplifications located downstream of HMGA2 on chromosome 12 [29–31]. Further molecular studies and cell biological studies might unravel this complex relationship.
Fig. 4A schematic overview of HMGA2 gene expression. (A) The HMGA2, MDM2 and CDK4 genes are located on chromosome 12. (B) The HMGA2 gene consists of five exons, encoding the HMGA2 protein. (C) The HMGA2 protein binds to AT-rich domains of DNA and influences gene expression of the DNA by altering chromatin compactness, (D) and by facilitating the binding of transcription factors to the acidic C-terminal tail of the HMGA2 protein and the DNA
To create a larger case series and explore the correlation between molecular alteration and clinical outcome, cases from previous literature and clinical practice were combined. A key limitation is the lack of morphological review of the literature-derived cases, including four lesions classified as PA with MDM2 amplification. This precluded the assessment of atypia/atypical features, potentially overestimating the occurrence of an MDM2 amplification in HMGA2-altered PA. Furthermore, RNA fusion analysis of cases derived from our institutional archives was mostly performed when canalicular-like/cellular morphology, cytonuclear atypia, or invasive growth were encountered. This selective approach introduced bias, resulting in 42% CXPA, a high percentage compared to the overall risk of malignant transformation in PA, which is reported to be between 1.5 and 9.5%, and up to 20% in HMGA2::WIF1 altered cases [2, 4, 5]. Due to the current limited use of molecular analysis of PA and CXPA, a high-quality, prospective cohort of HMGA2-altered neoplasms is difficult to collect. This is a common limitation in salivary gland neoplasm research, partly owing to the rarity of (malignant) tumors, underscoring the need for close collaborations in the future.
In conclusion, we found that immunohistochemical MDM2 expression and MDM2 amplifications are frequent in HMGA2-altered salivary gland tumors with cytonuclear atypia, potentially playing a role in the progression towards malignancy. MDM2 could be a valuable immunohistochemical staining in the head and neck pathologist’s immunohistochemical toolbox to identify the HMGA2-altered lesions and may explain the presence of cytonuclear atypia. However, the ‘trias’ of striking cytonuclear atypia, HMGA2-alteration and MDM2 amplification is currently insufficient evidence to diagnose CXPA in the absence of the classical diagnostic criteria, and no significant association between MDM2 status and clinical outcome was confirmed in this analysis.
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
Supplementary Material 3
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1de Lima-Souza RA, Bělohlávková K, Michal M, Altemani A, Mariano FV, Skálová A (2025) Atypical and worrisome histological features in pleomorphic adenoma: challenging and potentially significant diagnostic pitfall. Virchows Arch 18. 10.1007/s 00428-024-04015-z 10.1007/s 00428-024-04015-z 39827206 · doi ↗ · pubmed ↗
- 2Alsugair Z, Fieux M, Descotes F, Lopez J, Cordonnier C, Russel J et al (2024) Peculiar nuclear atypia associated with MDM 2 gene amplification in carcinoma ex-pleomorphic adenoma harbouring an alteration of HMGA 2. Histopathology. 6. 10.1111/his.1520910.1111/his.1520938708906 · doi ↗ · pubmed ↗
- 3Mansoori B et al (2021) HMGA 2 as a critical regulator in Cancer development. Genes (Basel) 12(2). 10.3390/genes 1202026910.3390/genes 12020269 PMC 791770433668453 · doi ↗ · pubmed ↗