Public Awareness and Attitude Towards Stroke in the Southern Region of Saudi Arabia: A Cross-Sectional Study
Abdullah I Aedh, Naif H Ali, Awam A Alsulaiman, Saleh Y Alyami, Ali I Alquraisha, Hussain M AlSulaiman, Hajar A Al Mustanyir, Raghad A Alsaiari, Hamza A Alalhareth, Zuhair M Almalki, Aeshah S Alqahtani

TL;DR
This study examines how well people in southern Saudi Arabia recognize stroke risks and symptoms, finding gaps that suggest a need for better public education.
Contribution
The study provides novel insights into stroke awareness in southern Saudi Arabia and identifies demographic predictors of knowledge.
Findings
Only 56% of participants correctly identified stroke as a brain disease.
Hypertension was the most recognized risk factor, acknowledged by 87% of participants.
Educational campaigns are needed to improve symptom recognition and timely medical response.
Abstract
Introduction Stroke is a leading cause of morbidity and mortality globally. Recognizing risk factors, identifying warning signs, and seeking timely medical intervention are crucial for preventing stroke and improving outcomes. This study aims to assess stroke awareness and attitudes among residents in southern Saudi Arabia and determine predictors of stroke knowledge. Methods A cross-sectional study was conducted among residents aged ≥18 years in the southern region of Saudi Arabia excluding individuals with a history of stroke and healthcare workers. A sample size of 576 participants was calculated. Data were collected conveniently via a self-administered online Arabic questionnaire that was adopted from the literature. The questionnaire assessed demographic characteristics, stroke knowledge, attitudes, and symptom responses. Data analysis was performed using multiple linear…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
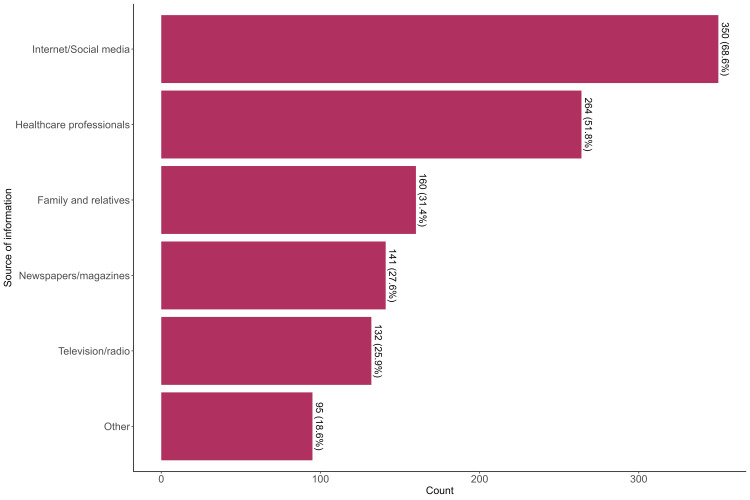 Figure 1
Figure 1| Characteristic | N = 5101 |
| Age | 29 (24, 40) |
| Gender | |
| Female | 222 (44%) |
| Male | 288 (56%) |
| Residence | |
| Abha region | 114 (22%) |
| Jazan region | 82 (16%) |
| Najran region | 314 (62%) |
| Marital status | |
| Single | 249 (49%) |
| Married | 218 (43%) |
| Divorced | 29 (5.7%) |
| Widowed | 14 (2.7%) |
| Nationality | |
| Non-Saudi | 40 (7.8%) |
| Saudi | 470 (92%) |
| Educational level | |
| Illiterate | 3 (0.6%) |
| Primary school | 6 (1.2%) |
| Secondary school | 7 (1.4%) |
| High school | 66 (13%) |
| University and above | 428 (84%) |
| Occupation | |
| Unemployed | 70 (14%) |
| Employed | 318 (62%) |
| Student | 122 (24%) |
| Income | |
| Less than 3000 RAS | 157 (31%) |
| 3000-10,000 RAS | 216 (42%) |
| More than 10,000 RAS | 137 (27%) |
| Family history of stroke | |
| Yes | 101 (20%) |
| No | 409 (80%) |
| Characteristic | Yes | No | I do not know |
| General knowledge of stroke | |||
| Stroke is a disease of the brain | 287 (56%) | 123 (24%) | 100 (20%) |
| Stroke is contagious | 8 (1.6%) | 457 (90%) | 45 (8.8%) |
| Stroke is an elderly person's disease | 73 (14%) | 353 (69%) | 84 (16%) |
| Stroke is a hereditary disease | 62 (12%) | 306 (60%) | 142 (28%) |
| Strokes can be prevented | 371 (73%) | 42 (8.2%) | 97 (19%) |
| Knowledge of stroke symptoms | |||
| Sudden dizziness | 332 (56%) | 69 (14%) | 109 (21%) |
| Sudden blindness or double vision | 347 (68%) | 60 (12%) | 103 (20%) |
| Sudden severe headache | 350 (69%) | 65 (13%) | 95 (19%) |
| Sudden onset of memory loss | 305 (60%) | 78 (15%) | 127 (25%) |
| Loss of consciousness or Fainting | 332 (65%) | 63 (12%) | 115 (23%) |
| Sudden weakness/numbness tingling of arm/leg | 365 (72%) | 49 (9.6%) | 96 (19%) |
| Sudden difficulty speaking or understanding speech | 399 (78%) | 40 (7.8%) | 71 (14%) |
| Knowledge of the consequences of stroke | |||
| Patients may encounter disabilities that persist long after the stroke is over | 418 (82%) | 92 (18%) | |
| Movement Functional problems (One-sided paralysis, Loss of ability to walk, tiredness, fatigue) after a stroke | 431 (85%) | 17 (3.3%) | 62 (12%) |
| Cognitive/Memory problems after a stroke | 412 (81%) | 34 (6.7%) | 64 (13%) |
| Visual problems (Loss of sight or blurred vision) after a stroke | 374 (73%) | 42 (8.2%) | 94 (18%) |
| Emotional personality changes (Depression, anger, or mood changes) after a stroke | 347 (68%) | 43 (8.4%) | 120 (24%) |
| Characteristic | Yes | No |
| Knowledge of stroke risk factors | ||
| High blood pressure | 443 (87%) | 67 (13%) |
| Smoking | 395 (77%) | 115 (23%) |
| Diabetes mellitus | 342 (67%) | 168 (33%) |
| High Cholesterol | 376 (74%) | 134 (26%) |
| Old age | 344 (67%) | 166 (33%) |
| Heart diseases | 397 (78%) | 113 (22%) |
| Obesity | 383 (75%) | 127 (25%) |
| Excessive alcohol | 425 (83%) | 85 (17%) |
| Psychosocial Stress | 442 (87%) | 68 (13%) |
| Physical inactivity | 362 (71%) | 148 (29%) |
| Characteristic | N = 510 |
| Identified symptoms of stroke | |
| 0 | 60 (12%) |
| 1-3 | 84 (16.5%) |
| ≥4 | 366 (71.6%) |
| Identified general information about stroke | |
| 0 | 28 (5.5%) |
| 1-2 | 216 (43%) |
| 3-5 | 266 (52.4%) |
| Identified risks of stroke | |
| 0 | 20 (3.9%) |
| 1-3 | 35 (6.8%) |
| 4-6 | 77 (15.1%) |
| 7-10 | 378 (74%) |
| Identified consequences of stroke | |
| 0 | 41 (8.0%) |
| 1-2 | 50 (9.8%) |
| 3-5 | 419 (82.2%) |
| Characteristic | N = 510 |
| Response to a person with symptoms of stroke | |
| Take him/her directly to the hospital | 459 (90%) |
| Call a doctor | 25 (4.9%) |
| I don't know what to do | 24 (4.7%) |
| Wait for spontaneous recovery | 2 (0.4%) |
| Interested in having more information about stroke | |
| No | 98 (19%) |
| Yes | 412 (81%) |
| Family care is helpful for early recovery of stroke patients after discharge | |
| No | 59 (12%) |
| Yes | 451 (88%) |
| General knowledge | Symptom knowledge | Risk knowledge | Consequence knowledge | |||||
| Characteristic | Beta1 | 95% CI2 | Beta1 | 95% CI2 | Beta1 | 95% CI2 | Beta1 | 95% CI2 |
| Age | 0.00 | -0.01, 0.01 | 0.02 | -0.01, 0.04 | 0.02 | -0.02, 0.05 | 0.02* | 0.00, 0.04 |
| Gender | ||||||||
| Female | — | — | — | — | — | — | — | — |
| Male | -0.03 | -0.22, 0.16 | -0.07 | -0.50, 0.36 | 0.50 | -0.01, 1.0 | -0.32* | -0.61, -0.03 |
| Residence | ||||||||
| Abha region | — | — | — | — | — | — | — | — |
| Jazan region | 0.23 | -0.06, 0.52 | 0.39 | -0.27, 1.0 | 0.48 | -0.30, 1.3 | 0.26 | -0.18, 0.70 |
| Najran region | -0.01 | -0.25, 0.23 | -1.0*** | -1.6, -0.49 | -0.80* | -1.4, -0.17 | -0.45* | -0.82, -0.09 |
| Marital status | ||||||||
| Single | — | — | — | — | — | — | — | — |
| Divorced | 0.49* | 0.03, 0.95 | 0.57 | -0.46, 1.6 | 0.71 | -0.51, 1.9 | 0.33 | -0.37, 1.0 |
| Married | 0.34* | 0.07, 0.61 | 0.22 | -0.39, 0.83 | 0.78* | 0.06, 1.5 | 0.10 | -0.30, 0.51 |
| Widowed | 0.35 | -0.26, 0.96 | 0.97 | -0.41, 2.3 | 1.5 | -0.08, 3.2 | 0.48 | -0.44, 1.4 |
| Nationality | ||||||||
| Non-Saudi | — | — | — | — | — | — | — | — |
| Saudi | -0.04 | -0.39, 0.32 | -0.70 | -1.5, 0.10 | -0.45 | -1.4, 0.49 | -0.32 | -0.85, 0.22 |
| Educational level | ||||||||
| Illiterate | — | — | — | — | — | — | — | — |
| High school | -0.11 | -1.3, 1.1 | -0.47 | -3.2, 2.2 | 0.65 | -2.6, 3.8 | 0.36 | -1.5, 2.2 |
| Primary school | 0.60 | -0.83, 2.0 | 1.2 | -2.1, 4.4 | 1.1 | -2.7, 4.9 | 0.54 | -1.6, 2.7 |
| Secondary school | 0.02 | -1.4, 1.4 | -0.50 | -3.6, 2.6 | 1.3 | -2.4, 5.1 | 1.1 | -1.0, 3.2 |
| University and above | 0.24 | -0.96, 1.4 | -0.01 | -2.7, 2.7 | 1.2 | -2.0, 4.4 | 0.79 | -1.0, 2.6 |
| Occupation | ||||||||
| Unemployed | — | — | — | — | — | — | — | — |
| Employed | -0.11 | -0.49, 0.26 | -0.50 | -1.3, 0.35 | -0.04 | -1.0, 0.96 | -0.19 | -0.75, 0.38 |
| Student | 0.33* | 0.01, 0.65 | 0.23 | -0.49, 0.95 | 0.74 | -0.11, 1.6 | 0.29 | -0.20, 0.77 |
| Income | ||||||||
| Less than 3000 RAS | — | — | — | — | — | — | — | — |
| 3000-10,000 RAS | 0.49** | 0.18, 0.81 | 0.82* | 0.11, 1.5 | 0.96* | 0.12, 1.8 | 0.44 | -0.03, 0.92 |
| More than 10,000 RAS | 0.38* | 0.03, 0.74 | 0.62 | -0.19, 1.4 | 0.63 | -0.32, 1.6 | 0.50 | -0.04, 1.0 |
| Family history of stroke | ||||||||
| No | — | — | — | — | — | — | — | — |
| Yes | 0.46*** | 0.22, 0.70 | 0.92*** | 0.38, 1.5 | 0.96** | 0.32, 1.6 | 0.45* | 0.09, 0.81 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Ischemic Stroke Management · Stroke Rehabilitation and Recovery · Neurological Disease Mechanisms and Treatments
Introduction
Stroke is a major cause of morbidity and mortality among the general population [1]. Its global impact highlights the need for a strong approach to reducing stroke risk [2]. Raising awareness and educating people about stroke is key to its prevention and management [3], which includes understanding risk factors, recognizing warning signs, and taking quick action when a stroke occurs [4]. Traditionally, prevention efforts have focused on increasing public knowledge, especially among high-risk groups [5].
In Riyadh, Saudi Arabia, the estimated stroke rate is about 43.8 per 100,000 people per year [6]. The average age of stroke onset in Gulf countries is relatively young, approximately 55 years, compared to developed countries [7] and compared to global figures, as a study on stroke characteristics in the Middle East and North Africa (MENA) region found the median age of stroke onset was 65 years, slightly younger than in non-MENA countries [8].
Increasing public awareness about stroke risk factors and warning signs can lead to faster responses and better treatment outcomes [9]. Community education programs are a key strategy in preventing strokes. These programs help assess people's knowledge about strokes and their risk factors [4, 10]. Educating the public not only improves their quality of life but also helps healthcare professionals manage stroke cases effectively in emergency settings [11]. Research suggests that 80% of stroke cases can be prevented through early action and precautions [12].
Studies among Lebanese adults show low awareness of stroke risk factors and the need to call emergency services quickly [13]. A study in Jordan found that stroke awareness is linked to education level and that factors like gender and socioeconomic status affect stroke outcomes [14]. In Riyadh, most people showed good knowledge of stroke risk factors and symptoms, but many did not understand the urgency of seeking emergency care [15]. Similarly, a study in Taif, Saudi Arabia, found that while people recognized stroke as a medical emergency, they struggled to identify its warning signs [16].
A study in Brazil found that 43.9% of people said they knew what a stroke was, 65% knew someone who had experienced it, 35% could name more than three risk factors, and 28.8% knew how to prevent it. Only 17.9% could list at least three stroke symptoms, 33.6% knew they should call emergency services, and just 3.1% said they would check when symptoms started [9]. However, studies have been conducted to assess stroke knowledge in the southern region of Saudi Arabia but they didn't target the general population [17-19]. Therefore, this study aims to assess stroke awareness and attitude among residents in the southern region of Saudi Arabia and to determine the predictors of awareness of stroke.
Materials and methods
Study design
This was a cross-sectional study conducted among residents of the southern region of Saudi Arabia aged 18 years and above. Individuals with a history of stroke and healthcare workers were excluded to avoid bias from experience and prior knowledge respectively. The study covered three major regions in southern Saudi Arabia: Jazan, Najran, and Aseer.
Sample size
The sample size was calculated using the formula: n = z² (p(1-p))/d²
where d is the margin of error (5%), p is the expected proportion (50%), and z is 1.96 for a 95% confidence interval. The initial calculated sample size was 384 participants. To account for a design effect of 1.5, the minimum required sample size was adjusted to 576 participants.
Sampling technique and study instrument
Data was collected conveniently through Google Forms distributed through social media platforms using an online, Arabic self-administered questionnaire. The questionnaire was developed based on literature [14] and underwent face validity evaluation by a panel of neurologists. A pilot study involving 20 participants was conducted to assess the clarity and comprehensibility of the questionnaire. Feedback from the pilot study led to minor refinements, and responses from the pilot study were excluded from the final analysis.
The finalized questionnaire consisted of four sections; the first included demographic characteristics such as age, gender, occupation, education, marital status, income, and family history of stroke. The second assessed the awareness of stroke signs and symptoms, risk factors, consequences, and sources of information about stroke. The third evaluated the attitude and perception and beliefs about stroke, while the fourth assessed the actions and behaviors in response to patients with stroke symptoms.
Statistical analysis
Data was gathered in Microsoft Excel (Microsoft Corp., Redmond, WA, USA), cleaned, and analyzed using SPSS version 26 (IBM Corp., Armonk, NY, USA). The normality of continuous variables was assessed using histograms and Kolmogorov-Smirnov test. Descriptive statistics included frequencies and percentages for categorical variables and median with interquartile range (IQR) for continuous variables. For the knowledge score, correct answers were coded one, incorrect and insured answers were coded zero, and the total score and score for each subtype was calculated. Multiple linear regression analysis was performed to identify predictors of stroke knowledge. Multicollinearity was assessed using the variance inflation factor (VIF). Statistical significance was set at P <0.05.
Ethical considerations
This study has been approved by the scientific research ethics committee of King Khalid Hospital at Najran Health Cluster (IRB registration number with KACST, KSA:H-11-N-136). Informed consent was obtained electronically via a mandatory consent checkbox in Google Forms before participants could proceed with the survey. Participants were informed of their right to withdraw at any time. Data confidentiality was maintained by anonymizing responses, with no personally identifiable information collected.
Results
The study included 510 participants with a median age of 29 years. More than half, 288 (56%), were males, 314 (62%) of participants primarily resided in the Najran region, and 249 (49%) were single. Most participants, 470 (92%), were Saudi nationals, and 428 (84%) had a university degree or higher. Regarding employment status, 318 (62%) were employed, 122 (24%) were students, and 70 (14%) were unemployed.
One hundred and fifty-seven (31%) earned less than 3000 RAS, 216 (42%) earned between 3000-10,000 RAS, and 137 (27%) earned more than 10,000 RAS. A family history of stroke was reported by 101 (20%) of participants (Table 1).
Regarding stroke knowledge, 287 (56%) recognized stroke as a brain disease, while only 8 (1.6%) believed stroke was contagious. Seventy-three participants (14%) agreed that stroke is an elderly disease. Similarly, 62 (12%) believed stroke is hereditary, and 371 (73%) recognized stroke as a preventable disease. Regarding stroke symptom knowledge, 332 (56%) identified sudden dizziness as a symptom. A total of 347 (68%) recognized sudden blindness or double vision, while 350 (69%) identified sudden severe headaches. Sudden memory loss was recognized by 305 (60%), loss of consciousness or fainting by 332 (65%), sudden weakness or numbness in the limbs by 365 (72%), and difficulty speaking or understanding speech by 399 (78%). Regarding stroke consequences, 418 (82%) acknowledged that stroke can cause persistent disabilities, while 431 (85%) identified movement-related issues. Cognitive or memory problems were recognized by 412 (81%), visual problems by 374 (73%), and emotional or personality changes by 347 (68%) (Table 2).
High blood pressure was the most recognized risk factor, identified by 443 (87%), while smoking was recognized as a risk factor by 395 (77%).
Diabetes mellitus was identified as a risk factor by 342 (67%), whereas 376 (74%) acknowledged high cholesterol as a risk factor. Old age was associated with stroke by 344 (67%), while 397 (78%) recognized heart disease as a risk factor. Obesity was acknowledged by 383 (75%), whereas excessive alcohol consumption was identified as a risk factor by 425 (83%). Psychosocial stress was recognized as a risk factor by 442 (87%), while physical inactivity was identified as a contributing factor by 362 (71%) (Table 3).
Regarding stroke symptoms, 60 (12%) could not identify any symptoms, while 84 (16.5%) recognized 1-3 symptoms, and 366 (71.6%) identified four or more. For general stroke knowledge, 28 (5.5%) had no correct knowledge, whereas 216 (43%) identified 1-2 key points, and 266 (52.4%) demonstrated knowledge of 3-5 aspects.
When evaluating stroke risk factors, 20 (3.9%) could not identify any, 35 (6.8%) recognized 1-3 factors, 77 (15.1%) identified 4-6 factors, and 378 (74%) were able to recognize 7-10 risk factors. For stroke consequences, 41 (8.0%) did not identify any, while 50 (9.8%) recognized 1-2 consequences and 419 (82.2%) identified 3-5 consequences (Table 4).
The majority, 459 (90%), indicated that they would take a person having stroke symptoms directly to the hospital, while 25 (4.9%) would call a doctor. Twenty-four (4.7%) reported not knowing what to do, and only 2 (0.4%) stated they would wait for spontaneous recovery.
Regarding stroke education, 412 (81%) expressed interest in obtaining more information about stroke, while 98 (19%) were not interested. Additionally, 451 (88%) of respondents believed that family care plays a crucial role in the early recovery of stroke patients after discharge, whereas 59 (12%) did not share this belief (Table 5).
The most cited sources of stroke information were Internet/social media which was cited by 350 (68.6%), 264 (51.8%) cited healthcare professionals and 160 (31.4%) cited family or relatives (Figure 1).
Source of information about stroke
Regarding general knowledge of stroke, age showed no significant association with general knowledge (Beta: 0.00, 95% CI: -0.01, 0.01). Males scored slightly lower than females, but the difference was insignificant (Beta: -0.03, 95% CI: -0.22, 0.16). Participants from the Jazan region scored higher (Beta: 0.23, 95% CI: -0.06, 0.52), though the difference was insignificant. Married participants (Beta: 0.34, 95% CI: 0.07, 0.61), divorced participants (Beta: 0.34, 95% CI: 0.07, 0.61) and those with a family history of stroke (Beta: 0.46, 95% CI: 0.22, 0.70) showed significantly better knowledge. Higher-income levels were also associated with better knowledge, with significant differences for participants earning 3000-10,000 RAS (Beta: 0.49, 95% CI: 0.18, 0.81) and more than 10,000 RAS (Beta: 0.38, 95% CI: 0.03, 0.74).
For symptom knowledge, age, gender, and nationality were not significantly associated. Participants from Najran had significantly lower knowledge (Beta: -1.0, 95% CI: -1.6, -0.49). A family history of stroke was strongly associated with better symptom knowledge (Beta: 0.92, 95% CI: 0.38, 1.5). Participants earning 3000-10,000 RAS also showed better knowledge (Beta: 0.82, 95% CI: 0.11, 1.5).
Regarding risk factors, knowledge, family history of stroke (Beta: 0.96, 95% CI: 0.32, 1.6) and earners of 3000-10,000 RAS (Beta: 0.96, 95% CI: 0.12, 1.8) were significantly associated with better risk knowledge. Participants from Najran had significantly lower scores (Beta: -0.80, 95% CI: -1.4, -0.17).
For consequence knowledge, older age (Beta: 0.02, 95% CI: 0.00, 0.04) and family history of stroke (Beta: 0.45, 95% CI: 0.09, 0.81) were significantly associated with better consequence knowledge. Males had significantly lower consequence knowledge scores than females (Beta: -0.32, 95% CI: -0.61, -0.03). Participants from Najran showed lower consequence knowledge (Beta: -0.45, 95% CI: -0.82, -0.09) (Table 6).
**Table 6: Determinants of knowledge of general information, symptoms, risk factors and consequences of stroke among the study participants1*p<0.05; **p<0.01; *p<0.001; beta = regression coefficientThe data has been represented as beta value and 95% confidence interval.2CI = Confidence Interval; P-value is significant at <0.05
Discussion
This cross-sectional study aimed to assess the knowledge and attitude of the general population regarding stroke. It included 510 participants, from different geographical areas in Saudi Arabia including Najran, Abha, and Jazan. The majority were educated at the university level.
Assessing stroke knowledge among the general population in more detail revealed that 56% are aware that stroke is a primary brain disease, the same percentages were evident in socio-demographically and economically different geography, as 55.8% of Italian populations are aware that stroke affects the brain [20]. Ninety percent of our participants know that stroke is not contagious, and 12% think stroke is hereditary. In Riyadh (the capital city), higher percentages were aware of this aspect of stroke, as 91% acknowledged that stroke is non-infectious.
Family history of stroke is associated with better knowledge, these findings are consistent with national literature. Similarly to these findings, another study among the Saudi population found that a history of risk factors (hypertension, obesity, and hyperlipidemia) is associated with better overall stroke knowledge and better awareness regarding stroke symptoms. This is probably due to the fact that stroke is long-lasting, and family members are likely to be involved in the rehabilitation and care of stroke patients. Also, frequent hospital visits will make their contact with healthcare providers more and hence more likely to get more education on stroke recognition and care. The same applies to patients with risk factors who are likely to be educated by their frequent follow-up visits [21,22].
The majority agree that stroke is a preventable disease. Regarding their knowledge about stroke symptoms, sudden dizziness was identified by 56% of the participants. Sudden blindness and sudden severe headache were identified by 68% and 69%, respectively. The most commonly known symptoms among the general population were difficulty speaking or understanding speech and sudden weakness or numbness in the limbs identified by 78% and 72%. In a different region, a study conducted in Al-Ahsaa, Saudi Arabia, the most recognized symptom was sudden numbness or weakness identified by 80% [23].
However, participants showed a good level of knowledge regarding stroke risk factors. High blood pressure, smoking, alcohol, diabetes mellitus, obesity and high cholesterol were identified as possible risk factors. Nevertheless, 78% appreciated that cardiac disease could be a major risk factor while 85% pointed to psychosocial stress as a possible risk factor. The same set of risk factors was also reported by participants from the Balqarn region of Arabia in a study conducted by Al Ameer et al. [24]. However, in different publications among the Saudi population, physical inactivity was the most identified risk factor for stroke [22,25]. Upon assessing predictors of stroke-related knowledge, there was no statistically significant association with age, gender, and geography. A significant association was evident among groups with a family history of stroke and those with higher incomes between 3000-10,000 and more than 10,000 RAS. Compared to international figures, in Portugal elderly and patients with hypertension showed higher stroke-related knowledge. Same as the study among the population in Italy, the most identified risk factor was hypertension and the most recognized symptom was hemiparesis [20,26].
Compared with another Arabic population, the overall stroke knowledge was similarly found to be low among Egyptians, however, higher income, educational level, and having risk factors of stroke were associated with better knowledge [27]. Generally, the overall level of knowledge and participants' ability to recognize different stroke symptoms seem to differ according to the method of questioning. A review found that 25% to 72% of participants were able to identify stroke symptoms when asked open-ended questions, compared to 95% to 100% when asked close-ended questions. In our case, close-ended questions were used in data collection [28]. A large-scale study in Japan recommended the use of mass media and personal communication to enhance general population knowledge [29].
Assessing participants’ attitude, the majority indicated that they would take a person exhibiting stroke symptoms directly to the hospital. And more than two-thirds of the population expressed their interest to enhance their knowledge regarding stroke. A study in the Tabuk region of Saudi Arabia revealed that despite population uncertainty about stroke treatment, 85% had a positive attitude toward stroke [30].
Limitation
The study has several limitations; first, the use of convenience sampling via online distribution may introduce selection bias, as it primarily targets individuals with internet access, which affects the generalizability of the findings. Future studies could consider alternative sampling methods, such as stratified or random sampling, to improve representativeness. Secondly, the study did not assess attitude more extendedly, and did not standardize an overall score for both knowledge and attitude. However, this didn’t affect the outcome of this study as the comparison was mainly to the individual elements of knowledge and attitude.
Conclusions
This study revealed a moderate knowledge of the general Saudi population regarding stroke symptoms and risk factors. A wider assessment of their source of information is needed to build baseline evidence for information dissemination in the future.
We recommend that more public educational campaigns be conducted to increase the population's overall knowledge of how to recognize stroke, how to deal with stroke patients acutely, and the possible first aid measurements that could be helpful in these situations. These programs should target, in the first place, the most at-risk population of stroke and their families. It could be delivered via television or social media as these are affordable, accessible and widely available. These campaigns can be governmentally funded and by healthcare workers.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Factors related to prehospital time in caring for patients with stroke Emergencias Soto-Cámara R González-Bernal J Aguilar-Parra JM Trigueros R López-Liria R González-Santos J 454463332021 https://revistaemergencias.org/wp-content/uploads/2023/09/Emergencias-2021_33_6_454-463-463_eng.pdf 34813193 · pubmed ↗
- 2Prevention of stroke: a global perspective The Lancet Pandian JD Gall SL Kate MP 126912783922018 https://www.thelancet.com/journals/lancet/article/PIIS 0140-6736(18)31269-8/abstract 10.1016/S 0140-6736(18)31269-830319114 · doi ↗ · pubmed ↗
- 3Recommendations for the establishment of stroke systems of care: recommendations from the American Stroke Association's Task Force on the Development of Stroke Systems Stroke Schwamm LH Pancioli A Acker JE 3rd 6907033620051568957710.1161/01.STR.0000158165.42884.4F · doi ↗ · pubmed ↗
- 4Knowledge of stroke risk factors, warning symptoms, and treatment among an Australian urban population Stroke Sug Yoon S Heller RF Levi C Wiggers J Fitzgerald PE 192612303220011148612710.1161/01.str.32.8.1926 · doi ↗ · pubmed ↗
- 5Association between stroke knowledge, stroke awareness, and preventive behaviors among older people: a cross-sectional study Nurs Health Sci Pothiban L Srirat C 3994052120193121921610.1111/nhs.12614 · doi ↗ · pubmed ↗
- 6Stroke awareness in the Saudi community living in Riyadh: prompt public health measures must be implemented J Stroke Cerebrovasc Dis Alaqeel A Al Ammari A Al Syefi N Al-Hussain F Mohammad Y 5005042320142368068010.1016/j.jstrokecerebrovasdis.2013.04.011 · doi ↗ · pubmed ↗
- 7The level of awareness of stroke risk factors and symptoms in the Gulf Cooperation Council countries: Gulf Cooperation Council stroke awareness study Neuroepidemiology Kamran S Bener AB Deleu D 2352422920071817608010.1159/000112856 · doi ↗ · pubmed ↗
- 8Stroke in the Middle-East and North Africa: a 2-year prospective observational study of stroke characteristics in the region-Results from the Safe Implementation of Treatments in Stroke (SITS)-Middle-East and North African (MENA)Int J Stroke Rukn SA Mazya MV Hentati F 7157221420193086045410.1177/1747493019830331 · doi ↗ · pubmed ↗