Classification of central facial paralysis: an agreement analysis
Nathallie Angel Conceição da Silva Andrade, Raquel Karoline Gonçalves Amaral, Laélia Cristina Caseiro Vicente, Aline Mansueto Mourão, Nathallie Angel Conceição da Silva Andrade, Raquel Karoline Gonçalves Amaral, Laélia Cristina Caseiro Vicente, Aline Mansueto Mourão

TL;DR
This study compares two scales for classifying central facial paralysis and finds that the Sunnybrook Facial Grading System is preferred by experts for its better interrater agreement.
Contribution
The study evaluates and compares the reliability of two facial paralysis classification scales using expert assessments.
Findings
The HB scale showed considerable interrater and excellent intrarater agreement.
The SFGS had good interrater and intrarater agreement and was preferred by all experts.
Both scales are useful, but the SFGS is considered more appropriate for classifying central facial paralysis.
Abstract
To identify whether there is interrater and intrarater agreement in the classification of the degree of central facial paralysis using two scales and verify which one is more appropriate to classify the severity of facial expressions according to experts’ opinion. Observational, prospective, cross-sectional study of agreement analysis of the House & Brackmann (HB) scale and the Sunnybrook Facial Grading System (SFGS). Five speech-language-hearing pathologists with clinical experience analyzed post-stroke facial expression of 30 adults for interrater agreement. They were evaluated in two stages, with a 10-day interval; the second stage involved 20% of the initial sample for intrarater agreement. The study used weighted kappa coefficient for the HB scale and the intraclass correlation coefficient for the SFGS classification. The HB scale indicated considerable interrater and excellent…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
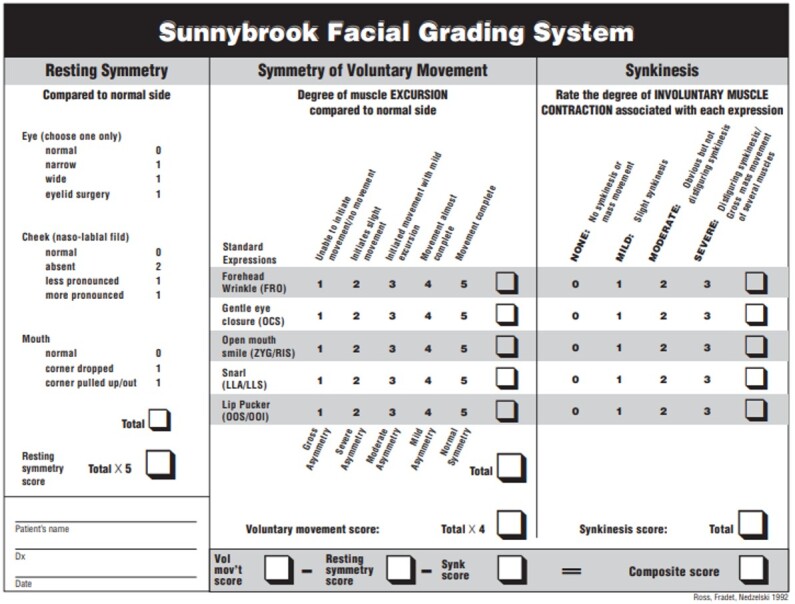 Figure 1
Figure 1|
|
|
|
|
|---|---|---|---|
| I | Normal | Symmetry | Normal facial function |
| II | Mild dysfunction | Normal symmetry and tone | |
| III | Moderate dysfunction | Normal symmetry and tone | |
| IV | Moderately severe dysfunction | Normal symmetry and tone | |
| V | Severe dysfunction | Asymmetry | |
| VI | Total paralysis | Asymmetry | No movement |
| 1. Which scale is the most appropriate for assessing central facial paralysis? |
| ( ) House & Brackmann (HB) |
| ( ) Sunnybrook Facial Grading System (SFGS) |
| 2. Please, share the reason(s) for your choice |
|
|
|
| ||||
|---|---|---|---|---|---|---|
|
|
|
|
|
|
|
|
|
| 0.321 | 0.202 | 0.445 | 0.817 | 0.616 | 0.917 |
|
| 0.245 | 0.132 | 0.356 | 0.791 | 0.598 | 0.883 |
|
| 0.315 | 0.232 | 0.428 | 0.882 | 0.558 | 0.956 |
|
| 0.414 | 0.371 | 0.562 | 0.807 | 0.710 | 0.938 |
|
| 0.315 | 0.232 | 0.428 | 0.789 | 0.601 | 0.894 |
|
|
|
| ||||
|---|---|---|---|---|---|---|
|
|
|
|
|
|
| |
|
| 0.854 | 0.733 | 0.929 | 0.887 | 0.756 | 0.956 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFacial Nerve Paralysis Treatment and Research · Ear Surgery and Otitis Media · Orthopedic Surgery and Rehabilitation
INTRODUCTION
Central facial paralysis (CFP) is one of the most common consequences in patients after a stroke, affecting more than half of them^(1)^. This condition causes facial asymmetry and muscular incapacity, mainly for facial movements in the lower face, influencing the patient’s functioning, aesthetic, social, and emotional aspects^(1,2)^.
CFP differs from peripheral facial paralysis (PFP) mainly in the location of the lesion and the type of movements and third of the face affected. PFP involves voluntary and involuntary movements in the entire hemiface ipsilateral to the lesion and is caused by lesions of the facial nerve (infranuclear innervation) or the nucleus of the facial nerve (nuclear). CFP lesion, in turn, occurs above the nucleus of the facial nerve in the brainstem, usually due to lesions or dysfunctions in the cerebral cortex, in the corticobulbar pathway or adjacent areas. In this case, it affects the voluntary muscles of the lower and midface contralateral to the lesion, due to the nucleus of the facial nerve that innervates the lower hemiface and receives corticonuclear fibers (supranuclear innervation) from the contralateral hemisphere. The facial nucleus that innervates the upper segment of the face receives corticonuclear fibers from both cerebral hemispheres, preserving facial expressions of the upper hemiface in lesions of the corticonuclear tract^(2)^.
It is important to note that PFP usually results from a stroke in the middle cerebral artery or its branches. However, strokes in other arteries, such as the basilar or middle meningeal arteries, can also cause PFP, as they help irrigate the facial nerve^(3)^.
Several protocols in the literature classify PFP, including the House & Brackmann (HB) (1985)^(4)^, Chevalier (1987)^(5)^, and Yahanagihara (1976)^(6)^ scales, and the Sunnybrook Facial Grading System (SFGS) (1994)^(7)^. However, research did not find exclusive scales for classifying facial expressions in CFP. The HB scale evaluates the three thirds of the face at rest and in movement, and its classification consists of six degrees. According to the literature, it is the most used in both types of paralysis in clinical practice and scientific research^(8)^, being adapted to CFP cases^(9)^. The SFGS analyzes the face in three clinical parameters: symmetry at rest, symmetry in movement, and the occurrence of contractures and synkineses. Its main objective is to classify paralysis based on facial functioning^(7)^.
In health professionals’ experience, assessment is fundamental in identifying and defining the patient's clinical conditions and the resources available to determine the appropriate intervention for functional performance^(10)^. Being able to analyze abnormal movements correctly is essential for evaluating patients with functionally impaired movements^(10)^.
Hence, using specific scales to measure the degree of CFP can have a major impact on prioritizing interventions and monitoring patient progress^(11)^. It is extremely important in clinical speech-language-hearing (SLH) practice to use scales with a high degree of reliability and trustworthiness to improve the quality of care and optimize the professionals' time^(11)^. Therefore, CFP may require a more targeted assessment, requiring the professional to pay specific attention to abnormal movements that compromise facial expressions. Therefore, verifying whether the scales validated for PFP can be applied to CFP is important for clinical SLH practice because it corroborates the correct diagnosis and feasible intervention based on the patient's functional performance.
Thus, this study aimed to identify 1) whether there is interrater and intrarater agreement in the classification of the degree of CFP, using two scales (HB and SFGS) and 2) whether either of these is more appropriate for CFP according to experts’ opinion.
METHODS
This cross-sectional observational study was approved by the Research Ethics Committee of the Federal University of Minas Gerais under evaluation report no. 5.019.519. The study invited five SLH pathologists with experience in facial paralysis rehabilitation to evaluate 30 clinical cases of patients with post-stroke CFP. They agreed to participate in the research and signed an informed consent form.
Their evaluation was based on photographs and videos collected from the healthcare database of patients with post-stroke CFP at the Stroke Unit of the Risoleta Tolentino Neves Hospital. They contained the following facial expressions: “at rest”, “scared face”, “angry face”, “close eyes gently”, “close eyes tightly”, “open smile”, “closed smile”, “sad face”, “bad smell”, “pouting”, and “pursed lips”.
The five SLH pathologists evaluated each patient’s photographs and videos using two different scales: HB (1985) (4), which has not been adapted or validated for Brazilian Portuguese, and SFGS (1994) (7), which was translated, adapted, and validated for Brazilian Portuguese in 2022^(12)^.
The HB scale (Chart 1) assesses facial expressions at rest and in movement, classifying facial paralysis according to the level of paralysis affected by the thirds of the face, graded into six levels^(4)^. The adapted HB scale assesses CFP patients at rest (analyzing facial symmetry in the three thirds of the face) and in movement (approaching only the lower face)^(4)^.
Chart 1: Facial movement assessment according to House & Brackmann (1985)
The SFGS (Figure 1) assesses facial expressions regarding symmetry at rest and of voluntary movements and considers synkineses with the movements tested^(7,12)^. The main differences between the scales are that the SFGS offers a broader and more detailed numerical result, considering the function of specific facial muscles, and verify the occurrence of synkineses.
Sunnybrook Facial Grading System (2022)
The SLH pathologists participating in the study did not habitually use the HB and SFGS scales, although they had experience in monitoring patients with facial paralysis. Therefore, they were initially trained online to set a standard technical basis to assess facial paralysis with the two scales. The training presented the scales and clarified the forms of assessment, as they are not specific to CFP, and professionals could use them in different ways, making the results agreement analysis and the study unfeasible. Hence, the training equipped professionals with tools on how to use the scales and not how to interpret facial expressions.
The training used three CFP cases other than the 30 cases presented for analysis. The latter were selected from the database of photos and videos through stratified sampling according to the HB classification performed by an experienced SLH pathologist to balance the severity levels of the paralysis.
After training, the SLH pathologists received photographs and videos of the 30 clinical cases for interrater agreement. They were given 20 days to evaluate the cases as many times as necessary using the two scales (HB and SFGS), but they could not discuss them with peers.
The process of researching intrarater agreement began through the second assessment, 10 days after they submitted the first one. To this end, the five SLH pathologists received 20% of the initial sample (six cases), categorized differently from the first assessment, so that they could re-evaluate them using the same criteria established in the first assessment, likewise using the two scales.
In addition to evaluating the cases, the SLH pathologists were asked to answer the Facial Paralysis Classification Preference Questionnaire (Chart 2), developed by the authors with two questions, one defining the best scale for this assessment and the other explaining the reasons for the choice.
Chart 2: Facial Paralysis Classification Preference Questionnaire
The SLH pathologists' responses were tabulated, and the results were subjected to statistical analysis using SPSS, version 20. The interrater and intrarater agreement analyses were performed with the weighted kappa coefficient (K) for the HB classification (as it is an ordinal categorical variable) and the intraclass correlation coefficient (ICC) for the SFGS classification (as it is measured as a continuous variable). The analyses measured the agreement between two or more raters^(13,14)^. The intrarater agreement was verified considering the first and second assessments with a reproducibility of 20% of the total sample.
Kappa values equal to 0 were considered as poor agreement, from 0 to 0.20 as slight, from 0.21 to 0.40 as considerable, from 0.41 to 0.60 as moderate, from 0.61 to 0.80 as substantial, and above 0.80 as excellent agreement^(13)^. ICC values < 0.50 were considered as poor, from 0.50 to 0.75 as moderate, from 0.75 to 0.90 as good, and > 0.90 as excellent agreement^(14)^.
The questions on the evaluators' opinions underwent descriptive analysis.
RESULTS
The study included five SLH pathologists with a mean age of 36 years, standard deviation (SD) of 10.6, and a mean experience in facial paralysis rehabilitation of 8.8 years (SD = 3.2). All of them (100%) had a specialist title in Health Professional Residency (Multiprofessional), and two had a master's degree (40%). The 30 patients evaluated had flaccid phase CFP, with a mean of 2.75 days (SD = 1.41) since stroke onset, in the acute phase of the disease.
The interrater agreement results regarding the degree of CFP impairment with the HB scale indicated considerable agreement among most SLH pathologists (kappa between 0.21 and 0.40). Only one rater had moderate agreement, with kappa = 0.41. The interrater agreement results with the SFGS found good agreement among all SLH pathologists, with an ICC value between 0.75 and 0.90 (Table 1).
The intrarater investigation regarding the evaluation and re-evaluation with a 10-day interval found an excellent agreement with the HB scale (kappa = 0.854) and a good agreement with the SFGS (ICC = 0.887) (Table 2).
The qualitative analysis results showed that all SLH pathologists considered the SFGS the most appropriate scale for assessing and classifying CFP. The following aspects were described as motivations for choosing the scale: it can be used for any phase of facial paralysis (flaccid and sequelae, with or without synkineses); its detailed and quantitative analysis helps measure the evolution of the case based on facial function; it assesses rest, movement, and synkineses/contractures separately; and it is easier to complete than the HB scale, although more laborious.
DISCUSSION
The results of this study revealed that the SFGS had better interrater agreement than the HB because the latter proved to be more subjective, as it depends on the observation of all segments of the affected hemiface. The agreement was considerable and moderate with the HB scale and good with the SFGS. The intrarater agreement, in turn, was high with both scales, indicating a substantial agreement between the repeated evaluations by the same rater.
Several scales developed to assess PFP are adapted and used to assess and classify CFP. This study chose HB and SFGS mainly because of their different approaches to assessing the patient (respectively general and functional facial aspects), the clinical practices in which they are employed (simple vs. detailed assessment), and how long ago they were developed (old vs. recent publication).
The HB scale was developed in 1985^(4)^ and is the most widely used scale for evaluating and classifying PFP and CFP, despite not being adapted or validated for Brazilian Portuguese^(15)^.
A study in the literature applied this scale for the medical monitoring of patients undergoing surgery for vestibular schwannoma^(16)^. Another study tabulated the evolution of patients with PFP who received physical therapy treatment, based on the evaluation with the HB scale^(17)^. Yet another study used this scale for the epidemiological analysis of patients with CFP in a rehabilitation hospital^(18)^. They demonstrate that different health professionals apply the HB scale, and its simple, objective, categorized form of evaluation is therefore of utmost importance.
The SFGS was translated into Portuguese and adapted to Brazilian culture in 2022 (12). It was developed to provide a reliable and valid method to assess facial function and examine the face separately in specific facial expressions. Moreover, it has a continuous, broad scoring range and is sensitive to small changes in facial movement patterns (7, 12^)^.
A study evaluated the intrarater and interrater agreement with the SFGS among experienced professionals from otorhinolaryngology, physiotherapy, and SLH services in patients with PFP, concluding that it was an easily reproducible scale^(19)^. Van Veen et al.^(20)^ conducted an observational study to analyze the learning curve of inexperienced evaluators using the SFGS in the evaluation of 100 patients with facial paralysis. As a result, the interrater agreement was initially good, but gradually improved over time, stabilizing after approximately 70 evaluations. Thus, the research concluded that the SFGS is a viable evaluation system even for inexperienced evaluators, as long as they receive adequate prior training. This highlights the relevance of the SFGS in clinical practice, as new studies add evidence about its effectiveness in various applications.
An integrative literature review on SLH practice in facial paralysis describes that the main role of these pathologists is to readjust functional aspects of the face, involving speech, chewing, and facial expressions^(21)^. Therefore, SFGS’ better interrater agreement can be explained by its more specific assessment of the thirds of the face and the greater influence of facial functions in its final result when compared to the HB scale.
Few studies have evaluated CFP classification with the agreement methods used here. However, a cross-sectional observational study performed a reliability analysis of the SFGS in 32 patients with subacute stroke and concluded, based on the significant test-retest correlation, that the SFGS is reliable for evaluating facial paralysis also in patients affected by cerebrovascular disease^(22)^.
Mat Lazim et al.^(23)^ conducted a comparative study of three classification systems (HB scale, SFGS, and Sydney Scale) for assessing facial paralysis (regardless of its type) and predicting neural recovery. According to the authors, the HB scale, despite its ease of clinical use, has stopped being used due to insufficient sensitivity to monitor the patients’ clinical evolution. In contrast, the SFGS has advantages by demonstrating high reproducibility of results, also highlighted in the present study and corroborated by the agreement result. Furthermore, according to the referenced research, the SFGS is reliable even for inexperienced evaluators. Neville et al.^(24)^ also identified that professionals unanimously applied the SFGS in cases of facial paralysis.
Several studies in the literature compare different scales applied only to PFP to verify whether they are practical and useful for assessing and classifying facial paralysis in clinical SLH practice. Thus, the present study innovated by analyzing which PFP assessment method would be most appropriate to classify CFP.
Using standardized assessment resources organizes communication between health professionals, directly affecting the order of importance and organization of treatment and the temporal complexity of the process^(25)^. Therefore, the instruments used in clinical and hospital practice should be as specific and reliable as possible.
Further studies are needed on the application of SFGS in patients with CFP, comparing them before and after SLH therapy to analyze its reliability of use and the results in PFP.
Despite this study’s agreement using the SFGS, it is important to emphasize that it was not originally designed to assess or classify CFP^(7)^. Therefore, the need to develop in the medium or long term a specific scale to assess CFP has not yet been ruled out.
CONCLUSION
This study found that the SFGS performed better in the interrater agreement analysis than the HB scale, although the latter had considerable merits in the intrarater assessment.
Since both presented interrater and intrarater agreements, it is concluded that both scales are suitably adaptable and useful for assessing and classifying CFP. However, the SLH pathologists indicated the SFGS as the most appropriate.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pimenta E Costa A Bule JM Reis G Recuperar a expressão facial após parésia facial central Revista Ibero-Americana de Saúde e Envelhecimento.2019511691170610.24902/r.riase.2019.5(1).1691 · doi ↗
- 2Calais LL Gomez MVSG Bento RF Comerlatti LR Avaliação funcional da mímica na paralisia facial central por acidente cerebrovascular Pro Fono 200517221322210.1590/S 0104-5687200500020001016909531 · doi ↗ · pubmed ↗
- 3Yoshino Y Gono Y Tsuboi K Acute peripheral facial paralysis caused by tegmental pontine infarction BMJ Case Rep 2024174 e 25953410.1136/bcr-2023-25953438670569 PMC 11057195 · doi ↗ · pubmed ↗
- 4House JW Brackmann DE Facial nerve grading system Otolaryngol Head Neck Surg 198593214614710.1177/0194599885093002023921901 · doi ↗ · pubmed ↗
- 5Lacôte M Chevalier AM Miranda A Bleton J Stevenin P Avaliação da função motora da face nas lesões periféricas e centrais. Lacôte M Chevalier AM Miranda A Bleton JP Stevenin P Avaliação clínica da função muscular.São Paulo Manole 19871335
- 6Stennert E Facial nerve paralysis scoring system. Fish U Facial Nerve Surgery.Amstelveen, The Netherlands Kugler Medical Publications 1977543547
- 7Ross BR Fradet G Nedzelski JM Development of a sensitive clinical facial grading system Eur Arch Otorhinolaryngol 1994 S 180110.1007/978-3-642-85090-5_6310774344 · doi ↗ · pubmed ↗
- 8Garcia LRS de Almeida JJ Junior Souza HAO Neto Garcia LRS Acupuntura no tratamento da paralisia facial periférica: uma revisão sistemática Revista Recien.20211133536310.24276/rrecien 2021.11.33.53-63 · doi ↗