Retrospective Evaluation of the Efficacy of Combined Antiviral Therapy Versus Monotherapy in High-Risk Hospitalized COVID-19 Patients
Hind Khalid Goresh, Aisha K Almutiri, Abeer O Hadari, Raghdaa M Alzain, Shatha K Altewajri, Manar Almutairi

TL;DR
This study compares the effectiveness of combined antiviral therapy versus monotherapy in high-risk hospitalized COVID-19 patients.
Contribution
The study provides new evidence on the benefits of combining remdesivir and favipiravir for treating high-risk hospitalized patients.
Findings
Combined therapy showed better symptom improvement and oxygen saturation compared to monotherapy.
Patients on combined therapy had longer survival times and lower mortality rates.
One-third of participants experienced side effects, with renal and hepatic side effects being most common.
Abstract
The COVID-19 pandemic has led to a variety of clinical symptoms, ranging from mild respiratory problems to severe pneumonia and multi-organ failure. Remdesivir and favipiravir are approved to treat COVID-19 and are used as single agents in the Ministry of Health (MOH) protocol. However, there is limited research available on the effectiveness of their combined use. The aim of this cross-sectional study is to evaluate the efficacy and safety of remdesivir and favipiravir in reducing disease severity, hospitalization duration, and mortality rates among high-risk patients who have been hospitalized with COVID-19. A retrospective, cross-sectional study was conducted in adult patients who were treated with the MOH treatment protocol. The study period was from January 2021 to January 2022, and it included 47 patients treated with favipiravir or a combination of remdesivir and favipiravir. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
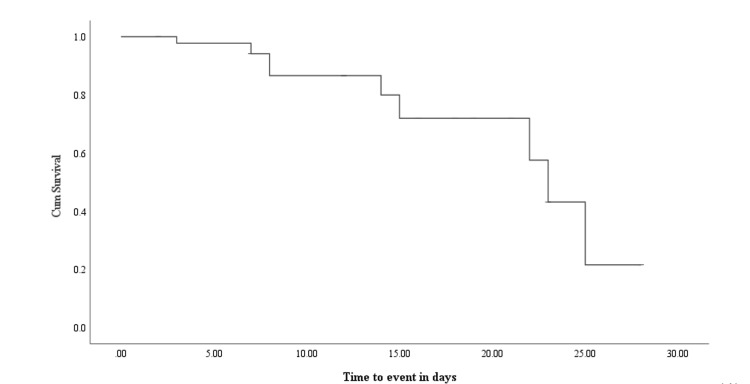 Figure 1
Figure 1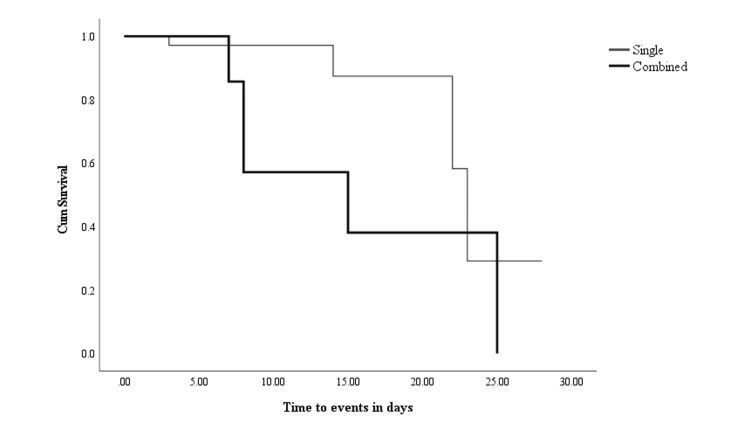 Figure 2
Figure 2| Variable | n = 47 | % |
| Age | ||
| 30-39 | 3 | 6.4 |
| 40-49 | 10 | 21.3 |
| 50-60 | 9 | 19.1 |
| Above 60 | 25 | 53.2 |
| Gender | ||
| Male | 26 | 55.3 |
| Female | 21 | 44.7 |
| Comorbidity | ||
| Hypertension | 28 | 59.6 |
| Diabetes mellitus | 23 | 48.9 |
| COPD/asthma | 6 | 12.8 |
| Obesity | 13 | 27.7 |
| Antiviral regimen | ||
| Single | 23 | 50 |
| Combined | 23 | 50 |
| Outcome | ||
| Alive | 37 | 78.7 |
| Death | 10 | 21.3 |
| Symptoms on admission | n = 47 | % |
| Fever | 33 | 70.2 |
| Cough | 40 | 85.1 |
| Chest pain | 6 | 12.8 |
| Shortness of breath | 28 | 59.6 |
| Fatigue | 2 | 4.3 |
| Current medications | ||
| Antihypertensive | 18 | 38.3 |
| Anticoagulant | 40 | 85.1 |
| Antiplatelet | 8 | 17 |
| Antidiabetic | 20 | 42.6 |
| Bronchodilator | 38 | 80.9 |
| On admission, renal/cardiac/hepatic function | ||
| Impaired renal function | 12 | 25.5 |
| Impaired liver function | 16 | 34 |
| Impaired cardiac function | 8 | 17 |
| Organ functions on completion of antiviral therapy | ||
| Cardiac function improvement | 9 | 19.1 |
| Pulmonary function improvement | 21 | 44.7 |
| Overall function improvement | 33 | 70.2 |
| Variable | Alive (n) | Died (n) | P-value |
| Fever | 25 | 8 | 0.45 |
| Cough | 32 | 8 | 0.61 |
| Chest pain | 5 | 1 | 0.77 |
| Shortness of breath | 23 | 5 | 0.49 |
| Fatigue | 1 | 1 | 0.38 |
| Obesity | 11 | 1 | 0.54 |
| Impaired renal function | 7 | 5 | 0.04* |
| Impaired liver function | 12 | 4 | 0.7 |
| Hypertension | 20 | 8 | 0.11 |
| Diabetes | 15 | 8 | 0.02* |
| Asthma/COPD | 5 | 1 | 0.76 |
| Combined antiviral | 5 | 6 | 0.002* |
| Antihypertensive | 10 | 8 | 0.001* |
| Anticoagulant | 31 | 9 | 0.45 |
| Antiplatelet | 3 | 5 | <0.001* |
| Antidiabetic | 13 | 7 | 0.013 |
| Bronchodilator | 28 | 10 | 0.74 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 Clinical Research Studies · Long-Term Effects of COVID-19 · SARS-CoV-2 and COVID-19 Research
Introduction
Coronaviruses are a group of respiratory viruses that cause diseases such as COVID-19, Middle East respiratory syndrome (MERS), and severe acute respiratory syndrome (SARS). SARS-CoV-2, which is a new coronavirus from the Coronavirus family, is believed to have originated in Wuhan, China. The leading hypothesis about its origin suggests that it became more pathogenic through a zoonotic event [1]. The rapid transmission of the infection was made possible by its ability to spread quickly, even through individuals who were asymptomatic. Furthermore, the limited capacity for testing, inefficient treatment methods, and the failure to implement early contact tracing and quarantine measures all contributed to the unprecedented global spread of the infection. The SARS-CoV-2 virus had an impressive ability to spread quickly among people worldwide through respiratory droplets, even when individuals did not exhibit any symptoms [1,2]. The COVID-19 outbreak quickly overwhelmed a significant number of hospitals and healthcare facilities globally, affecting almost every nation and demographic. Despite this unprecedented challenge, countries developed innovative treatments and created vaccines while also implementing measures to reduce the transmission of the virus between people. These measures included widespread quarantine and isolation, mandatory mask-wearing, and comprehensive stay-at-home orders in combination with the closure of businesses and gatherings [3]. In March 2020, the World Health Organization declared COVID-19 a global public health emergency. As of August 2021, there have been almost 200 million confirmed cases of SARS-CoV-2 worldwide and over 4.2 million deaths. This makes COVID-19 one of the deadliest epidemics in recorded human history [2]. This protocol offers evidence-based strategies for managing COVID-19 cases and includes a national treatment plan covering supportive care and medicines for all case levels. The Ministry of Health (MOH) monitors adherence to the protocol and provides guidelines for its implementation and reducing adverse effects [4]. Asymptomatic patients can end their self-isolation after 10 days, provided that they have been fever-free for at least three days and there has been a clinical improvement in symptoms. Pharmacotherapy is unnecessary for those who do not exhibit any symptoms, while mild to severe cases will be categorized based on clinical assessment and need urgent therapy for COVID-19 complications [5]. Remdesivir can cause infusion reactions, diarrhea, anemia, hyperglycemia, and elevated alanine aminotransferase (ALT)/serum glutamate pyruvate transaminase (SGPT) and aspartate aminotransferase (AST) levels on long-term treatment. It can affect kidney function, which might consequently lead to acute kidney injury (AKI) [6]. Favipiravir can cause liver impairment on long hospitalization, gastrointestinal effects, nausea, stomach discomfort, and rare instances of thrombocytopenia [7]. Studies show that antiviral drugs reduce mortality rates and shorten hospitalization durations. Single medicines like remdesivir or favipiravir are primarily used, and there is limited research on combined therapies, which are not yet approved [8,9].
Materials and methods
Patients and settings
This study was a retrospective cross-sectional study performed on the medical registry, from January 2021 to January 2022, of governmental tertiary hospitals. Adult patients diagnosed with COVID-19 were identified after the study was ethically approved. This study consisted of two groups of patients using either favipiravir 1600 mg or a combination of remdesivir 100 mg and favipiravir 1600 mg once daily. The study gathered information on clinical characteristics and comorbidity. All patients who used combined therapy (remdesivir plus favipiravir) for managing the complications of COVID-19 were identified from the hospital registry in the period mentioned above. An equal number of patients using monotherapy (favipiravir) was identified based on match criteria. The study encompassed all adult patients who were hospitalized and had high-risk characteristics, such as chronic obstructive pulmonary disease (COPD), asthma, renal impairment, liver impairment, diabetes, and any cardiovascular illness. Pediatric patients, pregnant patients, non-hospitalized patients, and hospitalized patients without any risk factors were excluded from the study.
Study variables and outcomes
The primary outcome showed that the combination of remdesivir and favipiravir is more effective than using favipiravir alone in treating high-risk hospitalized COVID-19 patients, leading to reduced mortality rates and shorter hospital stays. COVID-19 patients taking combined therapy had significantly longer survival times compared to those taking a single agent (15 and 23 days, P > 0.05, respectively). On independent t-test, oxygen saturation improvement was found significantly correlated with combined anti-viral regimen (P = 0.04). However, paired t-test showed significant improvement in oxygen saturation level for combined and single antiviral group (P = 0.01 and less than 0.001, respectively).
Data analysis
Data analysis was undertaken using the IBM SPSS Statistics for Windows, Version 24 (Released 2017; IBM Corp., Armonk, New York, United States). Continuous variables were presented as mean and standard deviation (SD). Categorical variables were presented by percentages and frequencies. Hypothesis testing was carried out, as appropriate, to determine whether there was a statistically significant difference between the variables of interest using α = 0.05.
Results
Demographic characteristics and outcomes
A total of 47 hospitalized COVID-19 patients were recruited for the study. The demographic data showed that half of the study participants were male (55%). Moreover, the age of the study participants ranges from 30 to 90 years (Table 1). The existence of comorbidities like hypertension, diabetes, renal impairment, and asthma or COPD was addressed to be 59.6% (n = 28), 48.9% (n = 23), 4.3% (n = 2) and 12.8% (n = 6), respectively (Table 1). The mean body weight of patients at admission was 75.9 ± 16.5 kg (mean ± SD).
Clinical characteristics and symptoms
All admitted cases presented with at least one COVID-19 symptom. The frequency of symptoms such as fever, cough, chest pain, shortness of breath, and fatigue was noted to be 70.2% (n = 33), 85.1% (n = 40), 12.8% (n = 6), 59.6% (n = 28) and 4.3% (n = 2), respectively (Table 2). The duration of antiviral therapy was noted to be a median of seven days. In addition, one-third (31.9%) of study participants developed side effects due to anti-viral administration. Proportions of renal and hepatic side effects were found to be comparable (25.5% and 21.3%, respectively). Furthermore, the frequency of overall symptom improvement on completion of antiviral therapy was found to be 70.2% (Table 2).
Association of clinical factors with COVID-19 treatment outcomes
On Chi-square and Fischer's exact test, impaired renal function, diabetes, and combined antiviral regimens were concluded to be significantly correlated with the treatment outcomes of COVID-19. Similarly, co-administration of antihypertensive and antiplatelet was significantly associated with the treatment outcomes. In contrast, fever, cough, chest pain, shortness of breath, and obesity were not associated with treatment outcome. Likewise, no adequate evidence to conclude a significant association with liver impairment, hypertension, asthma or COPD, antihypertensive, antidiabetic, and bronchodilator. Moreover, an insignificant difference was noted with regard to the adverse effect of antiviral regimens (P = 0.08). Oxygen saturation was measured on admission and at the end of treatment. On independent t-test, oxygen saturation improvement was found significantly correlated with combined antiviral regimen (P = 0.04). However, paired t-test showed significant improvement in oxygen saturation level for combined and single antiviral group (P = 0.01 and less than 0.001, respectively) (Table 3).
Table 3: Association of sociodemographic and clinical factors with treatment outcome.Statistical significance was determined using the Chi-square test, Fisher's exact test, and an independent t-test for categorical variables. The paired t-test was used to assess oxygen saturation improvement. Statistically significant at p < 0.05.COPD: Chronic obstructive pulmonary disease*
The probability of survival of COVID-19 patients
All study participants were followed in the hospital for a median of eight days with a total of 455 person-days (Figure 1).
Kaplan-Meier curve showing the survival probability of COVID-19 patients from the start of treatment to the end of the follow-up period.
A total of 10 death events were reported during the study period that yielded 22 poor outcomes per 1000 person-days. COVID-19 patients taking combined therapy had insignificantly shorter survival times compared with those taking single agents (15 and 23 months, P > 0.05, respectively). The cumulative probability of survival at the end of the study period among single and combined therapy was found to be 29% and 38%, respectively (Figure 2).
Kaplan-Meier survival probability curve comparing single and combined antiviral treatment groups.
Discussion
We believe that this study provides information regarding the efficacy and safety of single versus combined antiviral therapy among COVID-19 patients in Saudi Arabia to help evaluate treatment protocol in the country. Combination and single antiviral regimens are included in the treatment protocol of COVID-19 in the Kingdom.
The COVID-19 pandemic is a worldwide public health threat that yielded higher rates of mortality and affected the health of the elderly and people with comorbidities [10] and impacted morbidity and mortality. In our study, we found that 10 out of 47 (21.3%) developed poor outcomes (death). This value is lower than some studies conducted in Belgium (29.9%) [11] and China (28.3%) [12] and higher than that of Ethiopia (15.3%) [13]. These disparities could be attributed to the differences in the study sample, settings, study time, and study design.
Oxygen saturation improvement was found to be significantly associated with combined antiviral use; however, combined therapy was found to be significantly correlated with poor treatment outcomes (Table 3). Moreover, diabetes comorbidity, impaired renal function, antiplatelet use, and antihypertensives use were reported to be significantly associated with poor treatment outcomes (Table 3). To our knowledge, this is the first study in Saudi Arabia where combined versus single antiviral protocol is evaluated among hospitalized COVID-19 patients. Per protocol, in our study, our primary treatment outcomes were patient survival, whereas many secondary outcomes were evaluated to assess the efficacy and safety of the treatment regimen.
Improvement in clinical status, like oxygen saturation in our study, improved significantly with combined antiviral over monotherapy. This finding is consistent with related studies where combined antiviral therapy showed clinical improvement [14-16]. In contrast, Cai et al. reported that single antiviral showed chest improvement in computed tomography (CT) over combined therapy [17]. In addition, one study concluded that monotherapy had no benefit in improving clinical outcomes [18]. This contradiction could be attributed to the difference in the designs of these studies.
The adverse effects of antiviral regimens (combined versus single) showed an insignificant difference. A published article reported that combined antiviral therapy had fewer side effects compared to monotherapy [14,19], whereas Li et al. concluded that the adverse effect of combined therapy was higher compared with monotherapy [18]. On the other hand, Gao and his team addressed that the number of antiviral drugs had not predicted the occurrence of side effects [20].
Our study assessed the risk factors of poor outcomes (mortality) among hospitalized COVID-19 patients. Different published studies have assessed the existence of diabetes mellitus [21,22], COPD and asthma [23-25], HIV/AIDS, and chronic kidney disease [26]. Diabetes comorbidity was reported to be significantly associated with poor treatment outcomes in our study. Likewise, diabetes was reported to be a predictor of poor outcomes [21]. In addition, antihypertensive users predicted the occurrence of poor outcomes. Patients with cardiovascular disease like hypertension were found to be independent predictors of poor outcomes [21,27,28]. Impaired renal function was noted to be correlated with poor outcomes. Similarly, Tiwari et al. had concluded that renal impairment is an independent determinant of poor outcomes [29]. Furthermore, antiplatelet use was reported to be a risk factor of poor treatment outcome in our study, whereas a published retrospective cohort study reported that the use of anticoagulants had improved clinical outcomes [23].
In summary, diabetes comorbidity, impaired renal function, antiplatelet use, and antihypertensives use were concluded to be correlated with poor treatment outcomes. Consequently, addressing concerns with high blood glucose levels, renal impairment, and high blood pressure will be crucial in improving morbidity and mortality.
Study limitations
A cross-sectional study design was employed. Although this type of design is prone to selection bias, which is the main drawback, it was the most feasible option in this case. Additionally, the limited sample size may affect the study’s statistical power. Despite these limitations, we believe our findings are robust and can inform future research steps.
Conclusions
The findings of this study indicate that the concurrent use of remdesivir and favipiravir demonstrates a greater efficacy compared to the administration of favipiravir alone in treating high-risk hospitalized patients with COVID-19. These results emphasize the significant clinical benefits of utilizing combined antiviral regimens, which enhance patient outcomes, reduce mortality rates, and shorten the duration of hospital stays. The implications of this research support the adoption of dual treatment strategies in clinical practice to optimize patient care in this critical context. Further studies with adequate sample sizes can be employed to highlight the efficacy and safety of different COVID-19 antiviral protocols. In addition, case-control or retrospective cohort designs can be adopted to address the predictors of poor treatment outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Coronaviruses (COVID-19) 10 2024 2024 https://www.nfid.org/infectious-disease/coronaviruses/
- 2COVID-19: epidemiology Coronavirus Disease 2019 (COVID‐19): A Clinical Guide Quiroz P Rutherford GW Dube MP 121Wiley 2022
- 3Therapeutic strategies for COVID-19: progress and lessons learned Nat Rev Drug Discov Li G Hilgenfeld R Whitley R De Clercq E 4494752220233707660210.1038/s 41573-023-00672-y PMC 10113999 · doi ↗ · pubmed ↗
- 4COVID-19 in Saudi Arabia: the national health response East Mediterr Health J Khan A Alsofayan Y Alahmari A 111411242720213492771610.26719/emhj.21.048 · doi ↗ · pubmed ↗
- 5Saudi Mo H protocol for patients suspected of/confirmed with COVID-19 10 2024 2023 https://www.moh.gov.sa/en/Ministry/Media Center/Publications/Documents/MOH-therapeutic-protocol-for-COVID-19.pdf
- 6Clinical benefit of remdesivir in rhesus macaques infected with SARS-Co V-2Nature Williamson BN Feldmann F Schwarz B 27327658520203251679710.1038/s 41586-020-2423-5PMC 7486271 · doi ↗ · pubmed ↗
- 7Lippincott Illustrated Reviews: Pharmacology Whalen K Wolters Kluwer 2022 https://shop.lww.com/Lippincott-Illustrated-Reviews--Pharmacology/p/9781975170554?srsltid=Afm B Ooput VZ Xebb 1Zx Mff 2y Fh 7AA 9i 1d 6Ds H Uwsc 5Ul G Jz Yol Jdhs-w 5
- 8Effectiveness and safety of favipiravir compared to supportive care in moderately to critically ill COVID-19 patients: a retrospective study with propensity score matching sensitivity analysis Curr Med Res Opin Alamer A Alrashed AA Alfaifi M 108510973720213389054410.1080/03007995.2021.1920900 PMC 8146299 · doi ↗ · pubmed ↗