Adult Chiari Type I Malformation Presenting as Emergent Acute Respiratory Insufficiency: A Case Report and Literature Review
Pedro Ribeiro, João Nogueira, Maura Cambango, Leandro Oliveira, Frederica Coimbra

TL;DR
A rare case of Chiari type I malformation presented as sudden respiratory failure, requiring urgent surgery for recovery.
Contribution
Reports a rare presentation of Chiari type I malformation with acute respiratory insufficiency and successful surgical intervention.
Findings
Sudden respiratory insufficiency was caused by brainstem compression from Chiari type I malformation and syringomyelia.
Emergency posterior fossa decompressive craniectomy and C1 laminectomy led to clinical recovery.
No alternative causes were identified for the patient's acute symptoms.
Abstract
Chiari type I malformation (CM-1) is a condition that is often asymptomatic, though when symptoms occur, they commonly involve occipital headaches. Acute respiratory insufficiency as the presenting symptom requiring emergent surgical intervention is extremely rare. We present the case of a 51-year-old female who developed sudden-onset respiratory insufficiency due to CM-1 and syringomyelia affecting the brainstem, necessitating urgent surgical intervention. The patient, with a history of mild tetraparesis, arrived at the emergency department with an acute loss of consciousness, severe respiratory acidosis, and acidemia. Imaging revealed tonsillar herniation at the foramen magnum, significant compression of the bulbomedullary junction, and an extensive syringomyelic cavity extending from the cervical to the dorsal spine. The patient underwent a comprehensive evaluation, with no…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
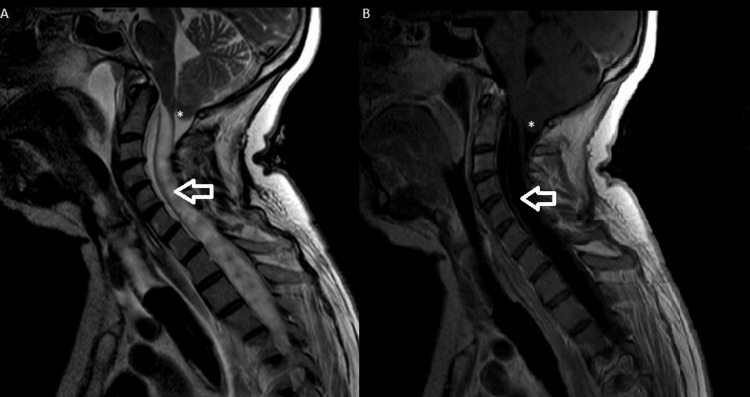 Figure 1
Figure 1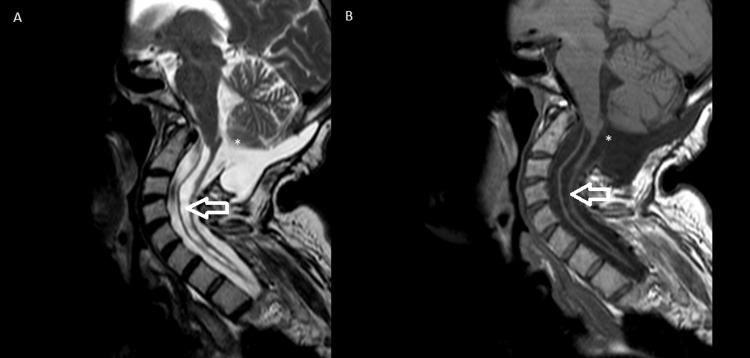 Figure 2
Figure 2| Author | Year | Age (years) | Gender | Previous Symptoms | Chiari Type | Syringomyelia/Syringobulbia | Surgery | Outcome |
| Bullock et al. [ | 1988 | 26 | Female | Dyspnea for two weeks | I | Yes | Decompressive suboccipital craniectomy and duroplasty | Nighttime mechanical ventilation |
| Fish et al. [ | 1988 | 63 | Female | Ataxia, occipital pain and dyspnea 10 days before, asthenia, dysphagia | I | - | Decompressive suboccipital craniectomy and C1 laminectomy | Asymptomatic |
| Fish et al. [ | 1988 | 54 | Female | Ataxia, respiratory pauses, dysphagia, tetraparesis | I | - | Decompressive suboccipital craniectomy and C1 laminectomy | Ataxia and tetraparesis |
| Alvarez et al. [ | 1995 | 38 | Male | Nocturnal dyspnea | I | Yes | Decompressive suboccipital craniectomy and C1 and C2 laminectomy | Resolution of severe symptoms |
| Omer et al. [ | 1996 | 23 | Male | Paraparesis | I | Yes | Decompression of the foramen magnum | Asymptomatic |
| Omer et al. [ | 1996 | 26 | Female | Dyspnea, dysphagia, asthenia, paraparesis | I | No | Decompression of the foramen magnum | Sudden death 2 months after surgery |
| Gentry et al. [ | 2001 | 38 | Male | Dyspnea, dysphagia, ataxia, upper limb weakness, daytime hypersomnolence, snoring | I | Yes | Decompressive suboccipital craniectomy and C1, C2 and C3 laminectomy | Resolution of severe symptoms |
| Tsara et al. [ | 2005 | 32 | Male | Morning headache, fatigue | I | Yes | Decompression of the foramen magnum and duroplasty | Persistence of sleep-related respiratory changes, daytime hypercapnia |
| Gladding et al. [ | 2005 | 22 | Male | Difficulty breathing at night | I | Yes | Decompression of the foramen magnum and C1 and C2 laminectomy | Asymptomatic |
| Vasani et al. [ | 2017 | 35 | Male | Dyspnea | 1.5 | Yes | Decompressive suboccipital craniectomy and C1 and C2 laminectomy | Asymptomatic |
| Ribeiro et al. | 2024 | 51 | Female | Mild tetraparesis | 1.5 | Yes | Decompressive suboccipital craniectomy and C1 laminectomy | Mild tetraparesis; nighttime mechanical ventilation |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpinal Dysraphism and Malformations · Cerebrospinal fluid and hydrocephalus · Family and Disability Support Research
Introduction
Chiari type I malformation (CM) is a relatively common condition identified in approximately 1% of patients undergoing magnetic resonance imaging (MRI) [1,2]. Despite its prevalence, the underlying pathophysiological mechanisms remain poorly understood [3]. While CM is often asymptomatic, symptomatic cases typically present with gradually progressive symptoms [1,4]. The most frequent clinical manifestation is effort-induced headache [1]. Acute respiratory insufficiency as an initial presentation of CM is exceedingly rare, with only a few cases documented in the literature [5-12]. This case report aims to present a rare clinical case of an adult patient with abrupt-onset respiratory insufficiency due to CM, necessitating emergent surgical intervention, and to provide a literature review of similar cases involving acute respiratory insufficiency as the presenting symptom requiring urgent surgical treatment.
Case presentation
A 51-year-old female presented to the emergency department following an acute loss of consciousness. Prior to this event, the patient reported a progressive global decrease in limb strength, without any specific neurological deficits, and exhibited hyperreflexia in her osteotendinous reflexes. Her overall functional status was assessed using the Modified Rankin Scale (mRS), where she scored 2. Due to these findings, she was referred for further neurological evaluation and was awaiting cervical magnetic resonance imaging (MRI).
The patient was found comatose by her family and was immediately transported to the emergency department of her reference hospital. Upon arrival, she scored 6 on the Glasgow Coma Scale and demonstrated severe respiratory acidosis with acidemia, confirmed by arterial blood gas analysis (fraction of inspired oxygen (FiO2) 80%: pH 6.9; partial pressure of carbon dioxide (pCO2) 127 mmHg; partial pressure of oxygen (pO2) 220 mmHg). A computed tomography (CT) scan of the brain revealed a cerebellar tonsillar herniation with syringomyelia. Subsequently, a cervical and dorsal MRI (Figure 1) showed a tonsillar herniation at the foramen magnum, significantly compressing the bulbo-medullary junction, with an extensive syringomyelic cavity extending through the cervical and dorsal spine.
Magnetic resonance imaging, T2-weighted (A) and T1-weighted (B), performed at diagnosis before surgery.Cerebellar tonsillar herniation at the foramen magnum, significantly compressing the bulbo-medullary junction (white asterisk), with an extensive syringomyelic cavity extending through the cervical and dorsal spine (white arrow).
The most common causes, such as stroke, metabolic disturbances, and seizures, were excluded. Given the severity of her condition, the patient was transferred to a hospital with a neurosurgery unit. An emergency decompressive suboccipital median craniectomy and C1 laminectomy with dural opening and duroplasty were performed.
Post-surgery, the patient was admitted to an intensive care unit (ICU), where she required invasive mechanical ventilation and orotracheal intubation for two weeks. Following tracheostomy and ventilatory weaning, she recovered to a state of normal consciousness and was cooperative and oriented, and she remained in the ICU due to persistent hypercapnia, particularly at night, necessitating continuous nocturnal bilevel positive airway pressure (BIPAP). She remained in this unit for approximately two additional months before being transferred to a rehabilitation unit.
The patient underwent an intensive rehabilitation program for three months, gradually regaining functional capacity. At her one-year follow-up, she continued to experience mild tetraparesis and required nocturnal mechanical ventilation with BIPAP. Her overall functional status was assessed using the mRS, where she scored 3, indicating she was unable to perform all previous activities but was able to carry out daily activities with some limitations. The MRI scans of the brain and cervical spine, taken approximately one year after the event, are presented in Figure 2 and show that the volume of the extensive syringohydromyelic cavity is reduced in the current examination, with a consequent reduction in the volume occupied by the observable portions of the spinal cord.
Magnetic resonance imaging, T2-weighted (A) and T1-weighted (B), performed 1 year after surgeryPostoperative changes following foramen magnum decompression (white asterisk) and reduction of the syringomyelic cavity previously observed in the preoperative scan (white arrow)
Discussion
Eight articles from the literature search were included, covering the period from 1988 to 2017. In total, 10 adult patients with CM-1 presented with an abrupt onset of acute respiratory insufficiency, requiring emergent surgical treatment. The main characteristics of the 11 reported patients (including our clinical case) are summarized in Table 1.
The average age was 37.1 years (range 22-63 years), with a slight male predominance (n=6, 54.5%). All patients presented with acute respiratory insufficiency. Among the 11 included patients, 8 had prior complaints of dyspnea. Regarding the presence of syringomyelia/syringobulbia, this was documented in 8 out of the 11 patients. Decompressive surgery was performed on all patients. One case of mortality was reported among the 11 included patients, which occurred 2 months after surgery. The outcomes of the included patients are provided in Table 1.
CM-1 is often a chronic and asymptomatic condition. Many cases of CM-1 are found incidentally on MRI or CT scans [13]. Presentation as a life-threatening acute condition requiring emergent treatment is very rare. Only 4.6% of patients with CM-1 require urgent decompression surgery (within 24 hours of symptom deterioration) [4]. In the limited literature available on acute presentation in patients with CM-1, there is a significant association with preceding traumatic events, approximately 41.5% [14]. In patients with acute presentation, sudden death is estimated to occur in 12% of cases [14]. In this study, we focused on patients with CM-1 who presented acutely, without associated trauma, and with spontaneous symptoms in the absence of an apparent causal factor.
From an anatomical and imaging standpoint upon admission, we observed that in the vast majority of published clinical cases, as in our own, patients who presented more acutely had associated syringomyelic cavities. This finding aligns with the literature, which shows that patients with acute presentations tend to have larger and more extensive syrinx cavities compared to those with non-acute cases [4]. Massimi et al., in their review of patients with Chiari type I malformation and acute presentation, found syringomyelia in approximately 51% of cases [14]. Despite these findings, it is important to note that the prevalence of syringomyelia in the general population is relatively high, and in the vast majority of cases, surgery is not required [15]. Despite the association of CM-1 with syringomyelia, the natural history of this association appears to be benign, and most conservatively treated patients will not require surgery [16].
Clinically, previously published cases of acute CM-1 presentations most often involved spinal cord signs and symptoms, vocal cord paralysis, acute respiratory distress, cranial nerve dysfunction, or syncope [17]. Our clinical case aligns with this evidence. Follow-up of the patients selected for this study indicates that, in general, they had an excellent outcome, with symptom resolution before the event in almost all cases.
The type of surgery used in the collected cases was primarily decompressive surgery with or without cervical laminectomy, following standard surgical procedures. Despite the various surgical techniques available for the treatment of this condition [18,19], there is insufficient evidence to suggest that one specific type of surgical intervention is superior to another in the case of an acute symptomatic presentation.
Patients with CM-1 who have mild symptoms and a long follow-up period and are undergoing conservative treatment generally improve or do not worsen, with acute adverse events being infrequent [20]. Identifying risk factors for the acute deterioration of patients with Chiari type I malformation would facilitate the decision to proceed with early surgery. However, based on the available evidence, it remains very challenging to determine risk factors for the sudden deterioration of these patients [20].
Conclusions
In conclusion, our case contributes to the growing, although still limited, body of literature on acute presentations of CM-1 requiring emergent surgical intervention. While CM-1 is generally a chronic and asymptomatic condition, our findings highlight that a subset of patients may experience life-threatening acute respiratory insufficiency, necessitating urgent decompressive surgery. The presence of syringomyelia appears to be a common feature in these cases, suggesting its potential role in the pathophysiology of acute deterioration. Our literature review further supports the idea that emergent surgical decompression remains the standard approach for managing acute CM-1 presentations, often leading to favorable outcomes, although long-term neurological impairments, such as persistent tetraparesis and ventilatory dependence, may persist in some patients. The identification of predictive risk factors for acute decompensation remains uncertain, emphasizing the need for further research to refine patient selection for early surgical intervention and optimize clinical management strategies. Given the rarity of acute CM presentations, continued case reporting and larger-scale studies are essential to improve our understanding of the condition's natural history and refine management approaches. Better recognition of high-risk patients could enable earlier interventions, potentially preventing catastrophic neurological and respiratory complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chiari malformation (update on diagnosis and treatment)Neurol Clin Rosenblum JS Pomeraniec IJ Heiss JD 2973074020223546587610.1016/j.ncl.2021.11.007PMC 9043468 · doi ↗ · pubmed ↗
- 2Asymptomatic Chiari type I malformations identified on magnetic resonance imaging J Neurosurg Meadows J Kraut M Guarnieri M Haroun RI Carson BS 9209269220001083925010.3171/jns.2000.92.6.0920 · doi ↗ · pubmed ↗
- 3Chiari type 1-a malformation or a syndrome? A critical review Acta Neurochir (Wien) FričR Eide PK 1513152516220203165698210.1007/s 00701-019-04100-2 · doi ↗ · pubmed ↗
- 4Acute deterioration of adults with Chiari I malformation associated with extensive syrinx Br J Neurosurg Almotairi FS Tisell M 13173420203166808510.1080/02688697.2019.1684438 · doi ↗ · pubmed ↗
- 5Isolated central respiratory failure due to syringomyelia and Arnold-Chiari malformation BMJ Bullock R Todd NV Easton J Hadley D 144814492971988314701110.1136/bmj.297.6661.1448 PMC 1835174 · doi ↗ · pubmed ↗
- 6Respiratory arrest: a complication of cerebellar ectopia in adults J Neurol Neurosurg Psychiatry Fish DR Howard RS Wiles CM Simon L 714716511988340416910.1136/jnnp.51.5.714PMC 1033083 · doi ↗ · pubmed ↗
- 7Acute respiratory failure as the first sign of Arnold-Chiari malformation associated with syringomyelia Eur Respir J Alvarez D Requena I Arias M Valdés L Pereiro I De la Torre R 661663819957664871 · pubmed ↗
- 8Respiratory arrest: a complication of Arnold-Chiari malformation in adults Eur Neurol Omer S al-Kawi MZ Bohlega S Bouchama A Mclean D 3638361996871964810.1159/000117197 · doi ↗ · pubmed ↗