Fidaxomicin for Clostridioides difficile infection in patients with inflammatory bowel disease: a multicenter retrospective cohort study
Daniele Noviello, María Chaparro, Chiara Viganò, Andreas Blesl, Brigida Barberio, Henit Yanai, Ambrogio Orlando, Rocío Ferreiro-Iglesias, Cristina Bezzio, Alessandra Zilli, Tamás Molnár, Cristian Gheorghe, Francesco Conforti, Tommaso Innocenti, Simone Saibeni, Peter Bossuyt

TL;DR
This study shows that fidaxomicin is effective and safe for treating Clostridioides difficile infection in patients with inflammatory bowel disease, especially those who have not had the infection before.
Contribution
The study provides new evidence on the effectiveness and safety of fidaxomicin for CDI in IBD patients, highlighting better outcomes in CDI-naïve individuals.
Findings
CDI recurrence rate was 10% at week 8, with a sustained response rate of 82% at week 12.
CDI-naïve patients had lower recurrence and higher sustained response rates compared to those with previous CDI episodes.
Fidaxomicin was associated with a low colectomy rate and minimal adverse events in IBD patients.
Abstract
Inflammatory bowel disease (IBD) patients with Clostridioides difficile infection (CDI) are at increased risk of adverse outcomes. Data on fidaxomicin use in IBD remain scarce. We assessed the effectiveness and safety of fidaxomicin for CDI and its impact on IBD outcomes in a large international cohort. Adult patients with ulcerative colitis (UC) or Crohn’s disease (CD) treated with fidaxomicin for documented CDI were retrospectively included. The primary outcome was CDI recurrence rate within 8 weeks (C. difficile toxin detection and CDI-targeted therapy). Secondary outcomes included sustained response (no CDI-targeted therapy within 12 weeks), IBD therapy escalation, colectomy rate, and all-cause mortality within 30, 90, and 180 days. Ninety-six patients (57 UC and 39 CD) from 20 IBD centers were included. Most were on advanced IBD therapy. Half had a previous CDI episode, 15% a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
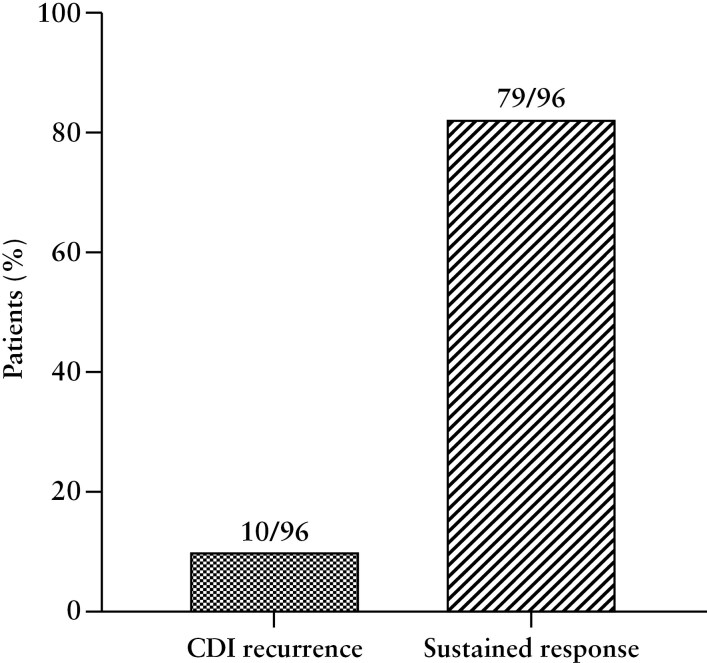 Figure 1
Figure 1| All patients | Ulcerative colitis | Crohn’s disease |
| |
|---|---|---|---|---|
| Age at onset, | .09 | |||
| - < 16 years | 14 (14.6%) | 12 (21.1%) | 2 (5.1%) | |
| -17 40 years | 56 (58.3%) | 30 (52.6%) | 26 (66.7%) | |
| - > 40 years | 26 (27.1%) | 15 (26.3%) | 11 (28.2%) | |
| Disease extension, | - | |||
| -Proctitis | - | 6 (10.6%) | - | |
| -Left-side | - | 11 (19.3%) | - | |
| -Extensive | - | 40 (70.2%) | - | |
| Disease location, | - | |||
| -Ileal | - | - | 3 (7.7%) | |
| -Colonic | - | - | 11 (28.2%) | |
| -Ileocolonic | - | - | 25 (64.1%) | |
| Disease behavior, | - | |||
| -Inflammatory | - | - | 26(66.7%) | |
| -Stricturing | - | - | 8(20.5%) | |
| -Penetrating | - | - | 3(7.7%) | |
| Disease duration, m | 45.1 (11.3 | 33.8 (17.5 | 55.6 (5.1 | 1 |
| Prior Crohn’s disease-related surgery, | - | - | 11 | - |
| Body mass index | 21.7 (19.7 | 21.7 (19.7 | 21.6 (19.7 | .91 |
| Family history of IBD, | 9 (9.2%) | 5 (8.6%) | 4 (10.0%) | .91 |
| Appendectomy, | 11 (12.2%) | 3 (5.2%) | 8 (20.5%) | .07 |
| Smoking, | <.01 | |||
| -never | 56 (58.3%) | 41 (71.9%) | 15 (38.5%) | |
| -former | 18 (18.8%) | 5 (8.7%) | 13 (33.3%) | |
| -active | 17 (17.7%) | 7 (12.3%) | 10 (27.6%) | |
| Prior systemic steroids cycles | 2.2 ± 2.3 | 2.2 ± 1.9 | 2.2 ± 2.9 | .82 |
| Failed azathioprine, | 39 (40.2%) | 27 (47.4%) | 12 (30.0%) | .10 |
| Failed methotrexate, | 4 (4.1%) | 2 (3.5%) | 2 (5%) | .48 |
| Naïve to advanced therapies, | 26 (27.1%) | 16 (28.1%) | 10 (25.6%) | .79 |
| Previous advanced therapy use, | ||||
| -Infliximab | 46 (65.7%) | 28 (68.3%) | 18 (62.1%) | |
| -Adalimumab | 26 (37.1%) | 9 (21.9%) | 18 (62.1%) | |
| -Golimumab | 2 (2.9%) | 2 (4.9%) | - | |
| -Vedolizumab | 35 (50.0%) | 24 (58.5%) | 11 (37.9%) | |
| -Ustekinumab | 22 (31.4%) | 12 (29.2%) | 10 (34.5%) | |
| -Risankizumab | 4 (%) | - | 5 (17.2%) | |
| -Tofacitinib | 5 (%) | 4 (9.8%) | - | |
| -Filgotinib | 1 (%) | 1 (2.4%) | - | |
| -Upadacitinib | 3 (%) | 3 (7.3%) | 1 (3.4%) | |
| -Etrasimod | 2 (%) | 1 (2.4%) | - | |
| Number of exposure to advanced therapy lines | .12 | |||
| -First | 25 (35.7%) | 15 (36.6%) | 10 (33.3%) | |
| -Second | 25 (35.7%) | 15 (36.6%) | 11 (36.7%) | |
| -Third | 9 (12.9%) | 5 (12.2%) | 4 (13.3%) | |
| -Fourth | 11 (15.7%) | 6 (14.6%) | 5 (16.7%) | |
| C-reactive protein*, mg/dL | 2.3 (0.5 | 2.1 (0.5 | 2.7 (0.6 | .74 |
| Calprotectin*, μg/g | 660 (262 | 732 (490 | 624 (123 | .58 |
| Mayo Endoscopic Subscore | - | |||
| -1 | - | 4 (20.0%) | - | |
| -2 | - | 8 (40.0%) | - | |
| -3 | - | 8 (40.0%) | - | |
| Simple Endoscopic Score for Crohn’s Disease | - | |||
| -mild | - | - | 3 (37.5%) | |
| -moderate | - | - | 2 (25.0%) | |
| -severe | - | - | 3 (37.5%) | |
| Concomitant** steroids, | .24 | |||
| -Methylprednisolone | 11 (33.3%) | 9 (40.9%) | 2 (18.2%) | |
| -Prednisone | 17 (51-5%) | 10 (45.5%) | 7 (63.6%) | |
| -Budesonide | 3 (9.1%) | 1 (4.5%) | 2(18.2%) | |
| -Beclomethasone dipropionate | 2 (6.1%) | 2 (9.1%) | - | |
| Concomitant** immunomodulator, | 5 (5.2%) | 4 (7.0%) | 1 (2.5%) | .64 |
| Concomitant** advanced therapy, | .11 | |||
| -Infliximab | 13 (23.2%) | 8 (22.2%) | 5 (25.0%) | |
| -Adalimumab | 6 (10.7%) | 2 (5.6%) | 4 (20.0%) | |
| -Golimumab | 1 (1.8%) | 1 (2.8%) | - | |
| -Vedolizumab | 17 (30.4%) | 12 (33.3%) | 5 (25.0%) | |
| -Ustekinumab | 9 (16.1%) | 6 (16.7%) | 3 (15.0%) | |
| -Risankizumab | 2 (3.6%) | - | 2 | |
| -Tofacitinib | 3(5.4%) | 3 (8.3%) | - | |
| -Filgotinib | 1 (1.8%) | 1 (2.8%) | - | |
| -Upadacitinib | 3 (5.4%) | 2(5.6%) | 1 (5.0%) | |
| -Investigational drug | 1 (1.8%) | 1 (2.8%) | - |
| All patients | Ulcerative colitis | Crohn’s disease |
| |
|---|---|---|---|---|
| Age at CDI diagnosis, years | 37 (25 | 35 (24 | 40 (26 | .45 |
| Female, | 47 (48.0%) | 27 (46.6%) | 20 (50.0%) | .74 |
| Number of previous CDI episodes, | .80 | |||
| -None | 46 (48.4%) | 25 (44.6%) | 21 (53.9%) | |
| -One | 29 (30.5%) | 18 (32.1%) | 11 (28.2%) | |
| -Two | 14 (14.7%) | 9 (16.1%) | 5 (12.8%) | |
| -Three or more | 6 (6.3%) | 4 (7.1%) | 2 (5.1%) | |
| Timeframe between last and current CDI episode, m | 2.7 (1.6 | 2.5 (1.6 | 3.3 (1.6 | .76 |
| Therapy for previous CDI episodes, | ||||
| -Metronidazole | 12 (16%) | 6 (12.2%) | 6 (23.1%) | |
| -Vancomycin standard dose | 44 (58.7%) | 29 (59.2%) | 15 (57.7%) | |
| -Vancomycin extended-pulsed | 15 (20%) | 13 (26.5%) | 2 (7.7%) | |
| -Fidaxomicin | 3 (4%) | 0 | 3 (11.5%) | |
| -Fecal microbial transplantation | 1 (1.3%) | 1 (2%) | 0 | |
| Hospitalization up to 8 weeks prior to current CDI episode, | 37 (38.5%) | 17 (30.4%) | 20 (51.3%) | .04 |
| -IBD-related | 25 (67.6%) | 13 (76.5%) | 12 (60%) | |
| -CDI-related | 8 (21.6%) | 3 (17.7%) | 5 (25%) | |
| -Infectious disease-related | 1 (2.7%) | 0 | 1 (5%) | |
| Proton pump inhibitors, | 26 (27.4%) | 13 (23.6%) | 12 (30.8%) | .34 |
| Antibiotics use in the 3 months prior to current CDI episode, | 33 (35.9%) | 15 (28.3%) | 18 (47.4%) | .16 |
| -Clindamycin | 2 | 1 | 1 | |
| -Cephalosporins | 9 | 4 | 5 | |
| -Penicillin | 9 | 2 | 7 | |
| -Fluoroquinolones | 9 | 4 | 5 | |
| -Tetracycline | 1 | 1 | 0 | |
| Current severe CDI episode, | 15 (15.5%) | 8 (14.0%) | 7 (17.9%) | .60 |
| Care intensity at diagnosis, | .84 | |||
| -outpatients | 53 (55.2%) | 31 (54.4%) | 22 (56.4%) | |
| -inpatients for IBD-related condition | 37 (38.6%) | 23 (40.4%) | 14 (35.9%) | |
| -inpatients for non IBD-related condition | 6 (6.2%) | 3 (5.2%) | 3 (7.7%) | |
| Care intensity during management, | .68 | |||
| -outpatients | 48 (49.5%) | 27 (47.4%) | 21 (52.5%) | |
| -inpatients | 48 (49.5%) | 29 (50.9%) | 19 (47.5%) | |
| Leukocytes, WBC/mm3 | 9050 (6375 | 9050 (6430 | 9100 (6030 | |
| Albumin, | 3.8 (3.1 | 3.8 (3.24 | 3.9 (3.1 | |
| Creatinine | 0.8 (0.68 | 0.88 (0.7 | 0.74 (0.66 | |
| Abdominal computed tomography within 1 week of CDI diagnosis, | 20 | 10 | 10 | |
| -Increased bowel wall thickness | 14 (70.0%) | 8 (80.0%) | 6 (60.0%) | .33 |
| -Bowel wall enhancement | 8 (40.0%) | 6 (60.0%) | 2 (20.0%) | .07 |
| -Bowel ditation | 3 (15.0%) | 1 (10.0%) | 2 (20.0%) | .53 |
| Endoscopic findings within 1 week of CDI diagnosis, | 15 | 8 | 7 | |
| -Pseudomembranes | 2 (13.3%) | 1 (12.5%) | 1 (14.3%) | .92 |
| -Ulcers | 13 (86.7%) | 7 (87.5%) | 6 (87.7%) | .92 |
| -Spontaneous bleeding | 6 (40.0%) | 4 (50.0%) | 2 (28.6%) | .40 |
| CDI recurrence | CDI recurrence- free |
| |
|---|---|---|---|
| Age at CDI diagnosis, years | 43 (23 | 35 (25 | .57 |
| Female | 3 (17.7%) | 43 (54.4%) | .006 |
| BMI | 20.9 (20.4 | 21.7 (19.6 | .53 |
| IBD disease duration, m | 28 (10.8 | 46.7 (11.3 | .38 |
| Age at IBD onset | .02 | ||
| - < 16 years | 6 (35.3%) | 8 (10.1%) | |
| -17 | 6 (35.3%) | 50 (63.3%) | |
| - > 40 years | 5 (29.4%) | 21 (26.6%) | |
| UC disease extension | .17 | ||
| -Proctitis | 0 | 6 (13.3%) | |
| - Left-side | 1 (8.3%) | 10 (22.2%) | |
| -Extensive | 11 (91.7%) | 29 (64.4%) | |
| CD disease location | .79 | ||
| -Ileal | 0 | 3 (3.8%) | |
| -Colonic | 2 (11.7%) | 9 (11.4%) | |
| -Ileocolonic | 3 (17.7%) | 22 (27.9%) | |
| -Isolated upper disease | 0 | 1 (1.3%) | |
| CD disease behavior | .99 | ||
| -Inflammatory | 4 (23.5%) | 22 (27.9%) | |
| -Stricturing | 1 (5.9%) | 7 (8.9%) | |
| -Penetrating | 0 | 3 (3.8%) | |
| Crohn’s disease-related surgery | 1 | 9 | |
| Family history of IBD | 1 (5.9%) | 8 (10.1%) | .57 |
| Appendectomy | 1 (5.9%) | 10 (12.7%) | .65 |
| Smoking | .54 | ||
| -Never | 12 (70.6%) | 44 (55.7%) | |
| -Former | 2 (11.8%) | 16 (20.3%) | |
| -Active | 3 (17.7%) | 14 (17.7%) | |
| Concomitant steroid use | 12 (70.6%) | 51 (64.6%) | .64 |
| Systemic steroids cycles | 32.5 (25 | 25 (15 | |
| Failed azathioprine | 4 (23.5%) | 35 (44.3%) | .11 |
| Failed methotrexate | 0 | 4 (5.1%) | .34 |
| Naïve to advanced therapies | 3 (17.6%) | 23 (29.1%) | .55 |
| Concomitant advanced therapy | .88 | ||
| -Infliximab | 4 (30.8%) | 9 (20.9%) | |
| -Adalimumab | 1 (7.7%) | 5 (11.6%) | |
| -Golimumab | 0 | 1 (2.3%) | |
| -Vedolizumab | 2 (15.4%) | 15 (34.9%) | |
| -Ustekinumab | 3 (23.1%) | 6 (13.9%) | |
| -Risankizumab | 1 (7.7%) | 1 (2.3%) | |
| -Tofacitinib | 1 (7.7%) | 2 4.6 (%) | |
| -Filgotinib | 0 | 1 (2.3%) | |
| -Upadacitinib | 1 (7.7%) | 2 (4.6%) | |
| -Investigational drug | 0 | 1 (2.3%) | |
| Mayo endoscopic score | .24 | ||
| -Mild | 1 (14.3%) | 3 (17.7%) | |
| -Moderate | 1 (14.3%) | 8 (47.1%) | |
| -Severe | 5 (71.4%) | 6 (35.3%) | |
| Hospitalization up to 8 weeks prior to CDI diagnosis | 6 (35.3%) | 31 (39.7%) | .7 |
| Timeframe between last and current CDI episode, m | 5.8 (1.7 | 2.2 (1.5 | .19 |
| Therapy for previous CDI episodes, | .69 | ||
| -Metronidazole | 0 | 1 (2.8%) | |
| -Vancomycin standard dose | 7 (58.3%) | 23 (63.9%) | |
| -Vancomycin extended-pulsed | 5 (41.7%) | 9 (25.0%) | |
| - Fidaxomicin | 0 | 2 (5.6%) | |
| -Fecal microbial transplantation | 0 | 1 (2.8%) | |
| Care intensity | .29 | ||
| -Outpatients | 6 (37.5%) | 42 (53.2%) | |
| -Inpatients | 10 (62.5%) | 37 (46.8%) | |
| Current severe CDI episode | 2 (11.8%) | 13 (16.5%) | .63 |
| Increased bowel wall thickness | 5 (25%) | 9 (45%) | .26 |
| Ulcers at endoscopy | 4 (26.7%) | 9 (60.0%) | .99 |
| Fidaxomicin-treated | |
|---|---|
| Dizziness | 0 |
| Cutaneous rash | 1 |
| Chills | 0 |
| Headache | 0 |
| Nausea | 1 (mild), 1 (moderate) |
| Vomiting | |
| Conjunctivitis | 1 |
| Asthenia | 1 |
| Laboratory abnormalities | |
| -Hyperuricemia | 0 |
| -Increased AST and/or ALT | 0 |
| -Leukopenia | 0 |
| -Azotemia | 0 |
| -Hypercalcemia | 0 |
| -Hypocalcemia | 1 |
| -Hyperglycemia | 0 |
| -Hyponatremia | 0 |
| -Hypophosphatemia | 0 |
| -Hypokalemia | 1 |
| -Neutropenia | 0 |
| -Lymphopenia | 0 |
| -Thrombocytopenia | 0 |
| -Increased International Normalized Ration | 0 |
- —Italy’s Ministry of Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClostridium difficile and Clostridium perfringens research · Gastrointestinal motility and disorders · Microscopic Colitis
1. Background
Patients with inflammatory bowel disease (IBD) have a nearly 5-fold increase in the risk of Clostridioides difficile infection (CDI) compared with the general population, harboring an estimated prevalence of 37.3 per 1000 and 10.9 per 1000 among patients with ulcerative colitis (UC) and Crohn’s disease (CD), respectively.^1,2^ Patients with IBD who develop CDI may exhibit atypical clinical features with respect to the general population, including younger age at onset, lack of recent antibiotic use, and community acquisition. Colonic involvement in IBD, biological therapy, and antibiotic use are independent risk factors for CDI among patients with IBD.^3^ In addition, IBD patients are more likely to experience IBD exacerbations requiring therapy escalation, emergency department visits, prolonged hospital stays, and an increased risk of colectomy and mortality.^4–7^ All symptomatic patients with IBD and confirmed CDI by stool testing should receive appropriate antimicrobial therapy. The American College of Gastroenterology suggests vancomycin for a minimum of 14 days in patients with IBD and CDI.^8^ The European Crohn’s and Colitis Organization (ECCO) Guidelines on the Prevention, Diagnosis, and Management of Infections in IBD state that oral vancomycin and fidaxomicin for 10 days are equally effective in treating non-severe CDI.^9^ However, these guidelines are guided by data from the general population and it has not been determined if this also applies to patients with IBD. Some studies specifically investigated the effectiveness of vancomycin in patients with IBD.^10,11^ However, data on fidaxomicin in IBD are very limited, mostly from small, single-center, non-IBD-focused studies.^12–15^ In addition, it remains unexplored whether the resolution of CDI may affect IBD outcomes. We aimed to assess the effectiveness of fidaxomicin for CDI in IBD patients in relation to CDI recurrence rate, the safety profile, and its impact on IBD outcomes in a large retrospective multicenter international cohort study.
2. Methods
2.1. Study design and patients
This is a retrospective multicenter cohort study involving 20 IBD referral centers across Europe and Israel. We performed a cross-referenced search of fidaxomicin prescriptions with a manual chart review of IBD patients seen at each participating center. Adult patients with an established diagnosis of UC or CD according to the current ECCO guidelines^16^ and a CDI episode, defined as a positive glutamate dehydrogenase antigen test or nucleic acid amplification test for toxigenic C. difficile or a toxin enzyme immunoassay, treated with fidaxomicin for at least 7 consecutive days were included (Supplementary Table S1). Patients with unclassified colitis, acute severe UC as per Truelove and Witts criteria,^17^ fidaxomicin therapy for less than 7 consecutive days, toxic megacolon, total abdominal colectomy, and ileal pouch anal anastomosis were excluded.
The date of CDI diagnosis was considered as the baseline. Demographic data, such as gender, age, smoking status, history of malignancy, and comorbidities; and IBD-related characteristics, including phenotype by Montreal Classification, age at diagnosis, disease duration, previous and current IBD treatments, C-reactive protein (CRP), faecal calprotectin, colonoscopy, or sigmoidoscopy up to 8 weeks prior to CDI were collected. Furthermore, CDI-related characteristics, such as recent hospitalization, systemic antibiotic use up to 8 weeks prior to CDI, proton pump inhibitors intake, number of CDI episodes, disease severity according to Zar criteria,^18^ colonoscopy or sigmoidoscopy findings or computed tomography features of the colon within one week of CDI diagnosis, complete blood count, serum creatinine, and albumin at baseline; intensity of care at the time of CDI diagnosis and during clinical management, such as outpatient, inpatient, or intensive care unit admission were extracted from patients’ clinical records. Study data were pseudo-anonymized and managed using an electronic data capture tool hosted at Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico (REDCap, Research Electronic Data Capture).^19^
2.2. Outcomes
The primary outcome was CDI recurrence rate, defined as C. difficile toxin detection and treatment with any antimicrobial directed at CDI or faecal microbial transplant within 8 weeks. Secondary outcomes included sustained response rate defined as no CDI treatment for 12 weeks, IBD therapy escalation rate defined as induction with an IBD advanced therapy, colectomy rate, and all-cause mortality within 30, 90, and 180 days. IBD- and CDI-related characteristics were analyzed through univariate analysis to investigate potential associations with CDI recurrence. The safety profile of fidaxomicin in IBD patients was assessed through a prespecified list of adverse events including dizziness, rash, chills, headache, nausea, vomiting, increased alanine aminotransferase, increased aspartate aminotransferase, hyperuricemia, leukopenia, hypercalcemia, hypocalcaemia, hyperglycaemia, hyponatremia, hypophosphatemia, neutropenia, lymphopenia, thrombocytopenia, and increased International Normalized Ration (INR), and any other adverse events were collected. The severity of adverse events (mild, moderate, or severe) was assigned according to the evaluation of the local investigator.
2.3. Statistics
Standard descriptive statistics were used to analyze patients’ characteristics. Continuous variables were described as median and interquartile range (IQR). Categorical variables were described as the number of cases and proportions. Comparisons between variables were performed by Chi-squared, Fisher exact test, and Mann–Whitney U tests. All statistical analysis was performed by Stata software (Stata Statistical Software: Release 18, StataCorp LLC).
2.4. Ethical considerations
The study was performed in accordance with the Declaration of Helsinki, Good Clinical Practice, and applicable regulatory requirements. The study was approved by the Ethics Committee of the coordinating center (Comitato Etico Milano Area 2: 3565) and, thereafter, by all the participating centers.
3. Results
3.1. Baseline characteristics of the patients
All clinical records of IBD patients in a regular follow-up at each participating IBD center up to September 2024 were retrospectively reviewed. Overall, 99 IBD patients with CDI treated with fidaxomicin were identified between 2013 and 2024 (90 cases from 2019 onward). Three patients were excluded due to incomplete data. Ninety-six patients, 57 with UC and 39 with CD, met the inclusion criteria and were included. IBD characteristics are summarized in Table 1. Most patients had UC (n = 57, 59%), median disease duration was 4 (IQR: 1*-10) years, and 70 (73%) were receiving an advanced therapy. Among patients with an objective IBD disease activity up to 8 weeks prior to CDI diagnosis, 46/70 (66%) had CRP ≥ 1 mg/dL, 37/48 (77%) had a faecal calprotectin ≥ 250 μg/g, 16/20 (80%) a Mayo endoscopic subscore ≥ 2, and 5/8 (63%) a Simple endoscopic score for CD ≥ 7. Table 2 summarizes baseline and CDI characteristics. The median age was 37 (IQR: 25-59), and 47 (48%) patients were female. The analyzed episode was the first episode of CDI in 46 (48%) patients, the first recurrence in 29 (31%) patients, and a second and more recurrences in 20 (21%) patients. The timeframe between the previous and the current CDI episode was 2.7 (IQR: 1.6-*10.3) months. Specifically, 17 (18%) patients had the previous CDI in the previous 2 months. Regarding prior treatments for CDI, most patients had received vancomycin 44 (59%) at standard—125 mg 4 times daily for 10-14 days—or 15 (20%) at extended-pulsed—if treatment lasted over 14 days—dose regimen (Supplementary Figure S1). About a third of patients had at least one additional CDI risk factor, such as recent hospitalization, proton pump inhibitors, and antibiotics use. Most patients (55%) were diagnosed in an outpatient setting, while the remaining were diagnosed during hospitalization, either due to IBD-related issues (38%) or unrelated conditions (6%). Half of the patients were hospitalized, and 16% fulfilled the definition of a severe CDI episode. In the 20 patients with an abdominal computed tomography within 1 week of CDI diagnosis, increased bowel wall thickness and bowel wall enhancement were predominantly reported. Ulcers and spontaneous bleeding were the most common endoscopic findings within 1 week of CDI diagnosis, while pseudomembranous were observed in only 2 patients (13%).
3.2. Effectiveness of fidaxomicin for CDI in relation to CDI recurrence rates
Most patients 83/96 (86%) received a fidaxomicin standard dose regimen (200 mg twice daily for 10 days), 9 received extended-pulsed dosing (200 mg twice daily for days 1-5, then 200 mg on alternate days for days 7-25), 2 received fidaxomicin 200 mg twice daily for 7 days, 2 for 14 days, and 1 for 15 days. CDI recurrence occurred in 10 (10%) patients at week 8, while 79 (82%) patients achieved a sustained response until week 12 (Figure 1). Female sex, but no other demographic characteristic, was associated with a reduced risk for CDI recurrence (Table 3). No IBD-related characteristic, including IBD type and phenotype, exposure to and type of IBD advanced therapy, steroid use at CDI diagnosis, was associated with CDI recurrence (Table 3). Patients at first CDI episode tended to have a lower recurrence rate (4% vs 16%; P = .06) and had a significantly higher sustained response (91% vs 75%; P = .04) rate compared with patients with previous CDI episode. No difference was found between patients with mild-moderate and severe CDI episodes in terms of CDI recurrence (10% vs 13%; P = .85) and sustained response (83% vs 87%; P = .87). The timeframe between the previous and current CDI episode, the type of previous therapy for CDI, care intensity, the severity of the current episode, increased bowel wall thickness, and ulcers at endoscopy were not associated with CDI recurrence (Table 3).
CDI recurrence rate at week 8 and sustained response rate at week 12.
3.3. CDI resolution through fidaxomicin influences IBD outcomes
Induction treatment with an IBD advanced therapy was required in almost half of the patients: 18 (19%), 18 (19%), and 10 (10%) patients within 30, 90, and 180 days, respectively. Of note, 10 patients were naïve to any IBD advanced therapy. These patients started predominantly anti-TNF, while anti-TNF- and vedolizumab-experienced patients initiated anti-IL12/IL23 or -IL23p19 antibody therapy (Supplementary Figure S2). Patients achieving, compared with not achieving, CDI sustained response showed a numerically lower need for IBD therapy escalation within 30 days, with 2 (12%) vs 16 (20%) (P = .42). No difference was found between patients with mild-moderate and severe CDI episodes (48% vs 47%; P = .92). Overall, 5 (5%) UC patients underwent colectomy for IBD-refractory disease activity within 96 (30*-*117) days after CDI diagnosis, despite advanced IBD therapy induction in 2 patients and without any recurrence of CDI. A 79-year-old UC patient with congestive heart failure, peripheral vascular disease, and atopic dermatitis died of urosepsis 107 days after CDI diagnosis, unrelated to the CDI episode or UC disease control.
3.4. Safety profile of fidaxomicin in IBD patients
Adverse events related to the treatment with fidaxomicin were documented in 5 patients (Table 4). Mild episodes of cutaneous rash (1), nausea (1), conjunctivitis (1), asthenia (1), hypokalaemia (1), and hypocalcaemia (1) were reported. One episode of moderate nausea was reported. No adverse events led to treatment discontinuation. No previously unreported adverse events were identified.
4. Discussion
This international multicenter cohort study provided the largest dataset so far collected on the real-life effectiveness and safety of fidaxomicin treatment in IBD patients with CDI. Our results showed that fidaxomicin was effective and safe for CDI resolution, with greater effectiveness for first episodes than recurrent ones which is comparable with non-IBD cohorts.^20^ Furthermore, CDI resolution might influence short-term IBD outcomes. The safety profile was consistent with that of fidaxomicin application in the general population.^21,22^
In the absence of randomized control trials (RCTs) specifically designed to investigate the effectiveness and safety of CDI-targeted therapies in IBD patients with CDI, reliance on real-world evidence from observational studies is extremely valuable in filling knowledge gaps. In this specific scenario, 2 case series investigated the effectiveness of fidaxomicin in subjects at-risk of CDI, including IBD patients, or 2 in IBD patients alone. However, no definitive conclusions can be drawn due to several limitations. A small sample size (up to 29 IBD patients), heterogeneous definitions of recurrence (diarrhoea, diarrhoea requiring hospital admission, diarrhoea and C. difficile toxin, diarrhoea, and any antibiotic treatment targeting CDI), and a heterogeneous follow-up timeframe (30 days, 8-12 weeks, 180 days).^12–15^ Our multicenter cohort study was designed to overcome these limitations with a large sample size, a stringent recurrence definition, and a follow-up timeframe consistent with RCTs.
The observed recurrence rate of 10% aligns with the lower end of the 7%*-*30% range reported in previous studies.^12–15^ This relatively low rate could be partly attributable to the strict recurrence definition, including the need for a CDI-targeted therapy, and the proportion of patients at first CDI episode. Notably, this rate is consistent with fidaxomicin data from the general population, predominantly first CDI episode, where recurrence required likewise a CDI-targeted treatment. No demographic characteristic, except for sex, was associated with a CDI recurrence risk. Specifically, female sex was associated with a reduced risk for CDI recurrence. Although epidemiological studies identified the inverse association between female sex and multiply recurrent CDI (defined as at least 3 courses of CDI antibiotics),^23^ no sex-related effect was reported in fidaxomicin RCTs among the general population.^21,22^ Notably, patients who received fidaxomicin for the first CDI episode experienced fewer recurrences than those with prior CDI episodes. This observation is consistent with data from the general population.^21,22^ However, applying fidaxomicin at the initial CDI occurrence may be particularly beneficial to IBD patients.
In fact, most studies associate the occurrence of CDI in IBD patients with an increased need for treatment optimization, colectomy, and mortality.^4–7^ In our cohort, a significant proportion (48%) of patients required IBD therapy escalation within 180 days after CDI diagnosis compared with a literature rate ranging between 21% and 47%.^4,11,24,25^ The high rate in our cohort could be partly attributable to the baseline IBD characteristics as most patients were already on advanced therapy, and some were on a second or subsequent line of therapy, compared with previous studies. Interestingly, patients achieving CDI resolution showed a numerically lower need for a novel advanced therapy within 30 days. Our results suggest that achieving sustained CDI resolution may potentially influence short-term IBD outcomes. This finding underscores the potential indirect benefit of CDI resolution on IBD disease control. Employing fidaxomicin at the initial occurrence of CDI may offer particular benefit to IBD patients, as it could reduce the vicious cycle of repeated CDI relapses and preempt the need for escalating both CDI- and IBD-related therapies. In fact, the management of steroids and advanced therapies for IBD disease control during a CDI episode can be challenging. According to the ECCO Guidelines on the Prevention, Diagnosis, and Management of Infections in IBD, the use of immunosuppressants can be maintained after careful risk-benefit evaluation and clinical judgment.^9^ The American Gastroenterological Association clinical practice guidelines recommend initiation of corticosteroids or immunosuppressive therapy 3*-*4 days after persistent symptoms of colitis despite appropriate antimicrobial therapy for CDI.^26^ Notably, corticosteroid use has been linked to a higher risk of colectomy in some cohorts, while biologic therapy may have a protective effect.^27,28^ However, patients receiving 2 or more immunosuppressive medications may face a higher risk of severe complications such as megacolon, bowel perforation, and mortality.^29^ A personalized approach, with vigilant monitoring and prompt therapy modifications, is essential for optimal care.
The observed colectomy rate (5%) aligns with the lower end of the 2%*-*48% range reported in IBD patients with CDI during hospitalization or up to 1-year follow-up.^4,10,11,15,24,30–32^ In our cohort, no colectomy was directly attributed to CDI, with the earliest surgery occurring 1 month after CDI diagnosis.
Fidaxomicin was well tolerated in our cohort. No AE led to treatment discontinuation, and no previously unrecognized safety signals emerged. This aligns with the established safety profile of fidaxomicin reported in general population studies and small IBD-focused case series.
Logistical and economic challenges regarding fidaxomicin use emerge in our cohort, as a substantial proportion of patients were hospitalized and repeatedly treated with metronidazole or vancomycin even for CDI recurrences. In certain countries, reimbursement for fidaxomicin requires hospital admission, limiting its use primarily to severe cases managed in inpatient settings. These inconsistencies across countries highlight the need for standardized reimbursement policies to ensure equitable access to any effective treatment.
Preventive strategies also play a crucial role in managing patients with multiple CDI relapses. Current guidelines recommend that patients in the general population who experience a second or subsequent recurrence of CDI, or those with a history of CDI and a high risk of recurrence, be treated with FMT or suppressive oral vancomycin therapy.^8^ Additionally, recent subgroup analyses suggest that a microbiota-based live biotherapeutic product is both safe and effective in preventing CDI recurrence following standard-of-care antimicrobials in patients with IBD—though it is not yet approved in Europe.^33^
This study comes with limitations of retrospective observational studies and some that should be acknowledged. The administration of varying fidaxomicin regimens may have influenced treatment outcomes, although almost all regimes adhered to the fidaxomicin data sheet. Notably, recent evidence suggests that also a shorter duration of treatment may still be effective.^34^ A few patients were tested exclusively through antigen or amplification test, potentially including colonization only. However, this is consistent with real-world studies on CDI.^14,15^ The absence of a comparator group restricts effectiveness comparison to other treatments, such as vancomycin. Heterogeneity regarding recurrence definition and follow-up timeframe also concerns vancomycin studies in IBD and limits indirect comparison.^10,11^ In addition, even a direct comparison through propensity score between fidaxomicin and vancomycin effectiveness in retrospective observational studies would be almost unfeasible due to the considerable challenges in accounting for the numerous variables associated with CDI and IBD. Thus, this large multicenter cohort provides a representative glimpse into clinical practice across Europe and Israel with a comprehensive assessment of both CDI and IBD disease characteristics, treatment patterns, and outcomes. Prospective controlled studies should confirm our findings and investigate optimal treatment positioning.
In conclusion, fidaxomicin is effective and safe for the resolution of CDI in IBD patients, with greater effectiveness for first episodes. The CDI resolution might reduce the short-term need for a novel advanced IBD therapy.
Supplementary Material
jjaf056_suppl_Supplementary_Figure_S1
jjaf056_suppl_Supplementary_Figure_S2
jjaf056_suppl_Supplementary_Table_S1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Singh H, Nugent Z, Yu BN, Lix LM, Targownik LE, Bernstein CN. Higher incidence of clostridium difficile infection among individuals with inflammatory bowel disease. Gastroenterology. 2017;153:430-438.e 2.28479377 10.1053/j.gastro.2017.04.044 · doi ↗ · pubmed ↗
- 2Nguyen GC, Kaplan GG, Harris ML, Brant SR. A national survey of the prevalence and impact of Clostridium difficile infection among hospitalized inflammatory bowel disease patients. Am J Gastroenterol. 2008;103:1443-1450.18513271 10.1111/j.1572-0241.2007.01780.x · doi ↗ · pubmed ↗
- 3Balram B, Battat R, Al-Khoury A, et al Risk factors associated with clostridium difficile infection in inflammatory bowel disease: a systematic review and meta-analysis. J Crohns Colitis. 2019;13:27-38.30247650 10.1093/ecco-jcc/jjy 143 · doi ↗ · pubmed ↗
- 4Jodorkovsky D, Young Y, Abreu MT. Clinical outcomes of patients with ulcerative colitis and co-existing Clostridium difficile infection. Dig Dis Sci. 2010;55:415-420.19255850 10.1007/s 10620-009-0749-9 · doi ↗ · pubmed ↗
- 5Murthy SK, Steinhart AH, Tinmouth J, Austin PC, Daneman N, Nguyen GC. Impact of Clostridium difficile colitis on 5-year health outcomes in patients with ulcerative colitis. Aliment Pharmacol Ther. 2012;36:1032-1039.23061526 10.1111/apt.12073 · doi ↗ · pubmed ↗
- 6Jen MH, Saxena S, Bottle A, Aylin P, Pollok RCG. Increased health burden associated with Clostridium difficile diarrhoea in patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2011;33:1322-1331.21517920 10.1111/j.1365-2036.2011.04661.x · doi ↗ · pubmed ↗
- 7Tariq R, Law CCY, Khanna S, Murthy S, Mc Curdy JD. The impact of clostridium difficile infection on mortality in patients with inflammatory bowel disease: a systematic review and meta-analysis. J Clin Gastroenterol. 2019;53:127-133.29206751 10.1097/MCG.0000000000000968 · doi ↗ · pubmed ↗
- 8Kelly CR, Fischer M, Allegretti JR, et al ACG clinical guidelines: prevention, diagnosis, and treatment of Clostridioides difficile infections. Am J Gastroenterol. 2021;116:1124-1147.34003176 10.14309/ajg.0000000000001278 · doi ↗ · pubmed ↗