Clear cell adenocarcinoma of the cervix, a rare entity of young females: A case report
Paramita Paul, Paramita Rudra Pal, Sadaf Hayat

TL;DR
A rare case of clear cell adenocarcinoma in an 18-year-old woman without DES exposure is reported, showing metastasis but no recurrence after treatment.
Contribution
This case report adds to the understanding of clear cell adenocarcinoma in young women not exposed to DES.
Findings
Clear cell adenocarcinoma was diagnosed in an 18-year-old woman without DES exposure.
Metastasis was found in lymph nodes, and the patient was staged as FIGO stage I.
No recurrence was observed after six months of follow-up.
Abstract
Clear cell adenocarcinoma of the cervix is a rare neoplasm that accounts for about 4-9% of all uterine cervical adenocarcinoma. It was first reported in young women with in-utero exposure of diethylstilbesterol (DES). However, many cases have been reported post-ban of DES that are not associated with diethylstilbesterol (DES). Here, we are reporting a case of clear cell adenocarcinoma in an 18-year-old woman without any exposure history of DES. An exophytic mass arising from the anterior lip was found in MRI. Biopsy from the mass was diagnosed as Clear cell adenocarcinoma of the cervix based on histopathological and immunohistochemical findings. The patient then underwent a total hysterectomy and bilateral salpingo-oophorectomy. One each of the right pelvic lymph nodes and external iliac lymph nodes showed metastatic deposits. The patient was staged as FIGO stage I [AJCC TNM staging…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
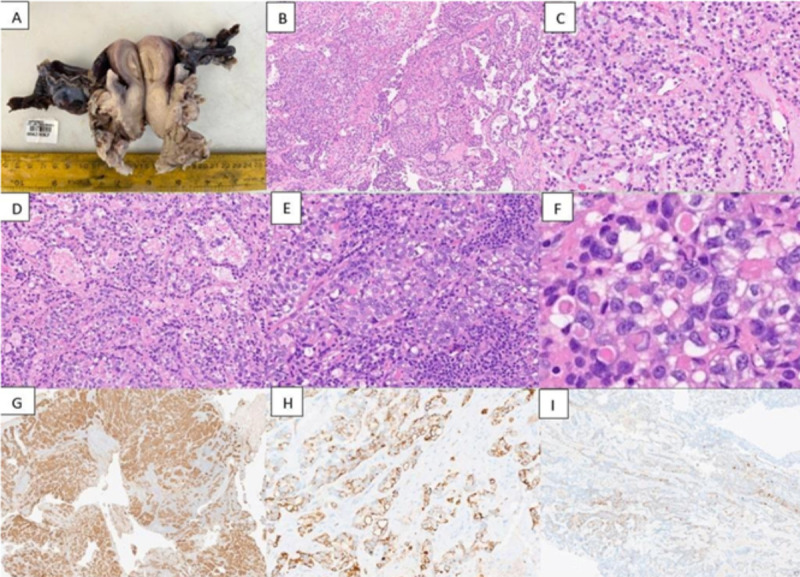 Figure 1
Figure 1| Tumor types | Immunohistochemistry | Molecular findings | ||||||||||
| Napsi n | HNF 1β | Vimentin | ER | PR | p53 | SA LL4 | Glypican 3 | AFP | WT 1 | PAX8 | ||
| Clear cell adeno-carcinoma | + | + | Wild type, usually | _/+ | +/_ | PI3K, ARID1 A, MMR genes | ||||||
| Yolk sac tumor | + | + | Wild type, usually | + | + | + | Usually isochromosome 12p | |||||
| High-grade Serous carcinoma with clear cell changes | _ | _ | _ | + (patchy to diffuse) | + (patchy to diffuse) | Mutant type | _ | _ | _ | + | + | p53, BRCA 1, BRCA 2, HRD with genomic instability |
| Endometrioid carcinoma with clear cell changes | _ | _ | + | + | + | Wild type, usually | _ | _ | _ | _ | _ | PTEN, β- catenin, ARID1 A, MMR genes |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndometrial and Cervical Cancer Treatments · Ovarian cancer diagnosis and treatment · Sarcoma Diagnosis and Treatment
Introduction
Clear cell adenocarcinoma of cervix is a rare neoplasm, especially in younger patients. It accounts for 4-9% of all uterine cervical adenocarcinoma^1,2^.A high significant association between diethylstilbesterol (DES) in utero exposure and subsequent clear cell adenocarcinoma of cervix in young women in later life was published in 1971^3^. But cases have been reported without exposure of DES in both young and older women likewise. It is important to note that pediatric patients tend to have a higher incidence of late-stage (stage III and IV) disease compared to adult patients diagnosed with this condition^4^. Typically, patients present with symptoms such as abnormal vaginal bleeding (including premenarchal, intermenstrual, postcoital, or postmenopausal), abnormal vaginal discharge, abdominal pain, or swelling in the lower extremities^5^. We report a case of clear cell adenocarcinoma in a young woman without any history of in -utero exposure of DES with the possible morphological mimics.
Case presentation
An 18-year-old girl presented with complaints of irregular on and off per vaginum (PV) bleeding and watery cervical discharge for a year. The patient had no relevant personal or family history. The patient was treated with progesterone 5 mg in a different hospital for same complaints but was not relieved of her symptoms. Pelvic MRI revealed a heterogeneously enhancing exophytic mass arising from the anterior cervical lip, measuring 4.2 x 7.3 x 4.5 cm. The uterus and ovaries were normal, and an enlarged indeterminate left external iliac node was seen measuring 2 x 1.3 cm. A cervical biopsy was performed which showed a tumor disposed of in tubule-cystic, solid nested and focal papillary pattern separated by fibrovascular septa (Figure 1A). The tumor cells show mild to moderate anisonucelosis, hyperchromatic to vesicular chromatin, occasional prominent nucleoli, and a moderate amount of eosinophilic to clear cytoplasm. The tubulo-cystic areas show nuclear hob nailing. Intervening stroma was hyalinized and showed myxoid change at places. (Figure 1B-E) Areas of necrosis were noted.
Intracytoplasmic hyaline globules were evident. (Figure 1F) Dense lymphoplasmacytic inflammatory infiltrates are seen within fibrous septa (Figure 1E) Foam cells aggregates were noted. Scattered mitoses were noted. Based on morphology a differential diagnosis of clear cell adenocarcinoma, germ cell tumor (GCT) (yolk sac tumor), and adenocarcinoma with clear cell change was considered and the tissue was subjected to immunohistochemistry (Table 1). On immuno-histochemistry, tumor cells were diffusely positive for AE1/AE3(pan-cytokeratin), CK7, and Napsin A (focal strong) while were negative for ER (ruling out endometrioid adenocarcinoma), SALL4 (ruling out GCTs), CEA, and p53 (wild type). p16 showed mosaic type of staining ruling out HPV association. Diagnosis of clear cell adenocarcinoma of the cervix (CCAC) was rendered based on histopathological and immunohistochemical findings.
Gross image shows a grey-white solid tumor involving cervix(A). Microscopic images of clear cell carcinoma (B-F) show an infiltrating tumor disposed in tubulo-cystic pattern and papillary pattern (B, H&E, ×40), tubulocystic areas, tumor cells exhibiting clear to eosinophilic cytoplasm with nuclear hobnailing. (C,D H&E,×200), a dense lymphocytic infiltrate seen focally (E, H&E, ×200), hyaline globules (F, H&E, ×400). Microscopic images of immunohistochemical results (G-I) .Tumor cells are diffusely positive for pancytokeratin (G, immuoperoxidase,×40), CK7 (H, immuoperoxidase,x200), and Napsin A (I, immuoperoxidase,x40).
Subsequently, a thoracoabdominal CT scan was performed for metastatic workup. No hepatic, pulmonary or skeletal metastasis was not found. The patient underwent total abdominal hysterectomy with bilateral salpingo-oophorectomy (TAH-BSO) and bilateral pelvic lymph node dissection. Bilateral ovaries, uterus, parametrium, and bilateral fallopian tubes were uninvolved. One each of the right pelvic lymph nodes and external iliac lymph nodes showed metastatic deposits. The patient was staged FIGO stage I [AJCC TNM staging (8th Edition): pT2b pN1].
Adjuvant radiotherapy was planned for this patient. Patient had received adjuvant chemoradiation (6cycles of Cisplatin and External beam radiotherapy 50Gy/25#) followed by vaginal cuff brachytherapy (6Gy/2#). At last follow up, after 1 year and 2 months of completing treatment patient is doing well without any complaints.
Discussion
In-utero DES exposure was a major risk factor associated with the development of clear cell adenocarcinoma of the cervix as described by Herbst AL et al in their study in 1971.
Subsequently, after the ban of DES, Herbst reviewed 705 cases of cervical and vaginal clear cell adenocarcinoma, of which 30% cases had no exposure history of DES^6^. The pathogenesis of non-DES exposure associated with clear cell adenocarcinoma of the cervix is unclear till now and the causal factors are postulated to be similar to the conventional carcinomas.
Clear cell adenocarcinoma of cervix cases shows two peaks of incidences according to multiple studies^7^. The first peak is found between 17 to 37 years of age (mean age, 26 years), while the second peak is between 44 to 88 years of age (mean age, 71 years).
Clear cell adenocarcinoma of the cervix may present as an exophytic lesion, an endophytic lesion (with a grossly normal-appearing cervix), or a barrel-shaped cervix. During physical examination, the lesions can vary in appearance, sometimes presenting as raised nodular red lesions or small punctate ulcers. On average, the size of the lesion at diagnosis is 3.3 cm^8^.
The microscopic patterns of CCAC include solid, tubule-cystic and papillary patterns, papillary pattern is the least common. The tubule-cystic pattern is associated with most favourable outcome, followed by papillary and solid patterns, respectively. The patient in this study has complaint of irregular vaginal bleeding, which is the most common initial symptom. Because of this non-specific clinical finding, diagnosis is often delayed. Moreover, the age and microscopic images can be a confounding factor. The presence of cystic spaces with hyaline globules may suggest a diagnosis of yolk sac tumor in young patients. In elderly population the differential diagnosis can include serous/ endometrioid carcinoma with clear cell change or even a squamous cell/ adenocarcinoma of cervix with clear cell change. Table 1 shows the possible differential diagnosis with immunohistochemical markers to differentiate the entities.
Treatment in young patient with this condition usually includes hysterectomy with fertility preservation. However, this case had already presented with lymph node metastasis which was confirmed on frozen and hence was subjected to TAH-BSO with lymph node dissection. Treatment strategy is not well described in CCAC because of relative paucity of literature and rarity of cases. For early-stage disease, surgery is the definitive treatment^9^. Most studies agree that clear cell carcinoma is a tumor linked to lymphovascular space invasion and lymph node metastases, with pelvic lymph node involvement observed in up to 25% of cases. Similarly, Stolnicu et al. reported lymphovascular invasion in 31% of cases and lymph node metastases in 24.1%. Additionally, 10.3% of cases were associated with abdomino-pelvic metastases, 32.8% experienced recurrences, and 19% succumbed to the disease^10^. Important negative prognostic factors are; a tumor more than 4 cm in size, positive lymph node metastasis, and advanced stages along with few histopathological findings like nuclear atypia, high mitotic count and solid growth pattern^1,9^. The FIGO stage and pelvic node status are the most important prognostic factors for progression-free survival and overall survival in these patients^11^. Key risk factors for recurrence include positive parametrial extension, positive pelvic lymph nodes, and positive vaginal margins. For patients with these high-risk factors, chemoradiation is the preferred postoperative adjuvant treatment^11^.
Conclusion
Etiopathogenesis of non-HPV-related cervical cancer is still unknown and it has mainly nonspecific clinical features that cause misdiagnosis of this entity in many times. As it can affect the pediatric population and adolescents, fertilizing preservation becomes an important consideration in the management of these patients, So, early diagnosis by clinicopathological correlation is needed for better management and disease-free survival for the patients with CCAC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clear Cell Carcinoma of the Uterine Cervix: Pathology and Prognosis in Surgically Treated Stage IB–IIB Disease in Women Not Exposed in Utero to Diethylstilbestrol 3331-335 Reich Olaf Tamussino Karl Lahousen Manfred Pickel Hellmuth Haas Josef Winter Raimund Gynecologic Oncology 7620001068470610.1006/gyno.1999.5700 · doi ↗ · pubmed ↗
- 2Primary Clear Cell Adenocarcinoma of the Uterine Cervix in a 14-Year-Old Virgin Girl: Case Report 2416652 Bujor Iuliana Elena Lozneanu Ludmila Ursache Alexandra Cristofor Alexandra Scurtu Ana-Maria Plamadeala Petru Gireada Roxana Mandici Cristina Elena GăinăMarcel Alexandru Matasariu Daniela Roxana International Journal of Environmental Research and Public Health 1920223655453310.3390/ijerph 192416652 PMC 9779421 · doi ↗ · pubmed ↗
- 3Adenocarcinoma of the vagina. Association of maternal stilbestrol therapy with tumor appearance in young women.1587881 Herbst A L Ulfelder H Poskanzer D C The New England journal of medicine 2841971554983010.1056/NEJM 197104222841604 · doi ↗ · pubmed ↗
- 4Cervical cancer in women under 25 years of age and outside the screening age: Diagnosis profile and long-term outcomes.1150156 Teixeira Julio Cesar Santos Daniel Zaidan Campos Cirbia Silva Vale Diama Bhadra Bragança Joana Froes Zeferino Luiz Carlos International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics 15420213334196210.1002/ijgo.13553 · doi ↗ · pubmed ↗
- 5Clinical Features and Prognostic Factors of Cervical Clear Cell Adenocarcinoma: A Retrospective Analysis of 74 Cases from a Tertiary Hospital.15330338221149297 Liu Yue Shi Xiaohua Yang Jiaxin Zhou Huimei Peng Peng Cao Dongyan Technology in cancer research & treatment 2220233671853110.1177/15330338221149297 PMC 9896093 · doi ↗ · pubmed ↗
- 6Clear cell adenocarcinoma of the vagina and cervix. An update of the central Netherlands registry showing twin age incidence peaks.11222936 Hanselaar A van Loosbroek M Schuurbiers O Helmerhorst T Bulten J Bernhelm J Cancer 791997917907110.1002/(sici)1097-0142(19970601)79:11<2229::aid-cncr 22>3.0.co;2-x · doi ↗ · pubmed ↗
- 7Clear cell carcinoma of the uterine cervix: clinical characteristics and feasibility of fertility-preserving treatment.1116 Jiang Xiang Jin Ying Li Yan Huang Hui-Fang Wu Ming Shen Keng Pan Ling-Ya Onco Targets and therapy 720142447076210.2147/OTT.S 53204 PMC 3891640 · doi ↗ · pubmed ↗
- 8Clear Cell Carcinoma of the Uterine Cervix: A Clinical and Pathological Analysis of 47 Patients Without Intrauterine Diethylstilbestrol Exposure.510091014 Yang Li Zheng Aiwen Zhang Xiang Fang Xianhua Sun Wenyong Chen Yaqing International journal of gynecological cancer : official journal of the International Gynecological Cancer Society 2720172849826110.1097/IGC.0000000000000992 · doi ↗ · pubmed ↗