A ruptured ovarian ectopic pregnancy presenting as acute abdomen: A case report
Seblewengel Maru Wubalem, Birhanu Kassie Reta, Mihret Adane Woldemichael, Sara Alemnew Wedaj, Shemsu Abraham Hussien

TL;DR
This case report describes a rare ovarian ectopic pregnancy that presented as an acute abdomen and highlights the importance of prompt diagnosis and surgical management.
Contribution
The paper emphasizes the diagnostic challenges of ovarian ectopic pregnancy and the necessity of considering it in patients with relevant symptoms.
Findings
Ovarian ectopic pregnancy is rare and often misdiagnosed preoperatively.
Surgical intervention and histopathologic examination are essential for confirmation and management.
Use of IUDs and ART may be associated with the occurrence of ovarian ectopic pregnancy.
Abstract
Ovarian ectopic pregnancy (OEP) is a well-known but rare type of ectopic pregnancy, accounting for approximately 0.5 %–3 % of all ectopic pregnancies. It is a potentially fatal type of ectopic pregnancy. Preoperatively diagnosis is difficult, as it can mimic tubal pregnancy or complicated ovarian cysts. The aim of this paper is to highlight the possibility of OEP in females presenting with acute abdomen and the necessity of prompt diagnosis and management of patients. A 28-year-old multiparous mother who had been amenorrheic for 4 weeks presents with a complaint of abdominal pain lasting 4 days. She had diffuse abdominal and cervical motion tenderness. The investigations revealed moderate anemia and right complex adnexal mass with hemoperitoneum. Right salphingoophrectomy was done for an assessment of ruptured ectopic pregnancy. Histopathologic examination confirmed ovarian ectopic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1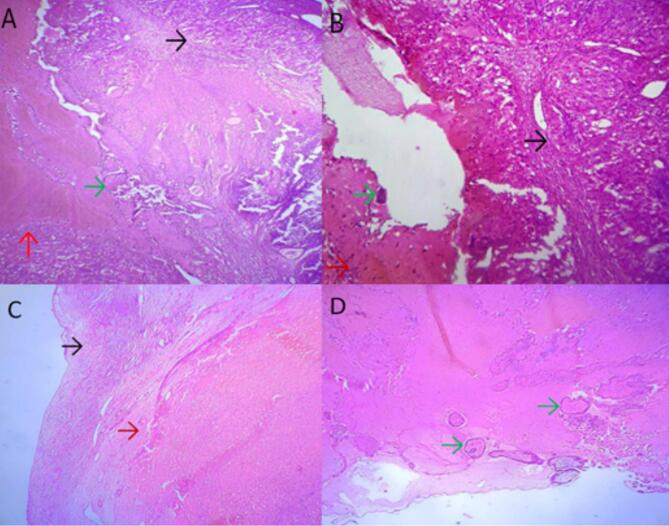 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEctopic Pregnancy Diagnosis and Management · Gestational Trophoblastic Disease Studies · Homicide, Infanticide, and Child Abuse
Introduction
1
Ovarian ectopic pregnancy (OEP) is a well-known but rare type of ectopic pregnancy, accounting for approximately 0.5 %–3 % of all ectopic pregnancies [1]. A systematic review of reports on OEP published on February 2023 found 667 articles of OEP since 1945 [2]. It is a potentially fatal type of ectopic pregnancy due to its occurrence in highly vascularized ovarian tissue and its association with a higher chance of rupture of the gestational sac, which leads to intraperitoneal bleeding and hemorrhagic shock [1,3]. It is difficult to diagnose OEP preoperatively, as it can mimic tubal pregnancy or complicated ovarian cysts, both clinically and in radiological studies [1,4,5]. Here, we present a rare case of ovarian ectopic pregnancy in a 28-year-old multiparous woman. This work has been reported in line with the SCARE guideline [6].
Case presentation
2
A 28-year-old gravida 5 para 4 (all alive and spontaneous vaginal deliveries) woman who had been amenorrheic for 4 weeks presented to the gynecologic emergency department with a complaint of abdominal pain lasting 4 days. The pain initially was on the right side and then progressively involved the whole abdomen. Otherwise, she had no history of vaginal bleeding, contraceptive use, or trauma to the abdomen.
On physical examination, she was tachycardic (pulse rate = 120, blood pressure = 120/68, and respiratory rate = 20). She exhibited conjunctival pallor. On abdominal examination, there was diffuse abdominal tenderness with no mass or organomegaly. There was cervical motion tenderness, and the cervix was closed on per vaginum examination. Her complete blood count profile showed moderate anemia (hemoglobin = 8.9 g/dl, hematocrit = 19.6 %). The urine β-HCG was positive. Abdominal-pelvic ultrasound revealed free fluid collection in the cul-de-sac, paracolic gutter, and Morrison's pouch. The uterus was empty, and there was a 2 × 3 cm complex right adnexal mass.
Given these finding; she was taken to the operating room for an emergency exploratory laparotomy. The abdomen was entered through a midline infraumbilical incision, revealing a ruptured right ovarian ectopic pregnancy and hemolyzed hemoperitoneum, with normal-appearing contralateral adnexa. Therefore, a right salpingo-oophorectomy was performed, and 500 ml of hemoperitoneum was aspirated.
The resected specimen was sent to the pathology department. Macroscopic examination demonstrated a 4.5 × 3 × 2 cm gray-white to gray-brown ovary, with a 2 × 2 cm hemorrhagic focus on cut sections (Fig. 1). Histopathologic sections revealed chorionic villi and trophoblastic cells along with hemorrhage and fibrin within the ovary, adjacent to a mature corpus luteum, confirming intraovarian pregnancy (Fig. 2).Fig. 1. Gross image of an ovary and a hemorrhagic focus (red arrow) of an OEP. (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)Fig. 1. Fig. 2Demonstrates histopathologic images of OEP. (A) Chronic villi (green arrow) embedded in hemorrhage (red arrow) and surrounded by corpus luteum (black arrow). (B) Corpus luteum (black arrow) with hemorrhagic area (red arrow) and syncytiotrophoblast (green arrow). (C) Ovarian stroma (black arrow) and hemorrhagic focus (red arrow). (D) Chorionic villi (green arrows). embedded in hemorrhage (4×, hematoxylin and eosin). (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)Fig. 2
The patient had a smooth postoperative period and was discharged on the fifth day with iron supplements and injectable contraceptives.
Discussion
3
The incidence of ovarian pregnancy is estimated to be 1 in 7000 to 40,000 live births [2]. Ectopic pregnancy is among the causes of first-trimester maternal death, accounting for around 10 % of pregnancy-related deaths [7].
The cause of ovarian ectopic pregnancy (OEP) is not clearly established, but several factors are associated with it. The proposed risk factors for OEP include the use of intrauterine devices (IUDs), assisted reproductive technologies (ART), endometriosis, pelvic inflammatory diseases, and previous pelvic or abdominal surgeries [2,3]. Previous pelvic or abdominal surgeries and IUDs are among the most frequently encountered risk factors, with around 81 % of OEP associated with IUDs [1,2,18]. IUDs can damage the fallopian tubal epithelium and interrupt the normal migration of the ovum [8,9]. Pelvic adhesions caused by pelvic inflammatory disease (PID), previous surgeries, or endometriosis can prevent the release of the ovum, which leads to fertilization in the ovary [3]. Various theories have been proposed regarding the mechanism of ovarian implantation in women undergoing ART, such as: uterine contractions resulting from difficult embryo transfer can lead to the retrograde movement of embryos through the fallopian tubes and into the ovary; ovarian trauma after oocyte retrieval can facilitate embryo implantation at the injured site; and a large number of spermatozoa that reach the ovary following intrauterine insemination can fertilize the ovum [3]. The patients can also present without any risk factors [10], like in this case.
Clinically, the patients presented with abdominal pain and amenorrhea, followed by vaginal bleedin [11]. When complicated by rupture, the main presentation will be hemorrhagic shock. Most of the cases are found in the first trimester [12]. However, there are reports of cases that lasted until full term [13].
The diagnosis of OEP is usually made postoperatively and confirmed by histopathological examination. Its similar clinical presentation and sonographic features to tubal pregnancy and complicated ovarian cysts make preoperative diagnosis difficult. The diagnosis remains challenging even during surgery [14,15]. Therefore; Spiegelberg's criteria are used for intraoperative diagnosis. The criteria include the presence of a normal ipsilateral tube that is separate from the ovary, the pregnancy occupying a normal position on the ovary, the ovary being attached to the uterus by the ovarian ligament, and pathologic confirmation of placental tissue attached to the ovarian stroma [9,15]. Ultrasound is the preferred imaging modality for the diagnosis of OEP. The classic sonographic features are a cyst with a wide echogenic outer ring and an empty uterus [8,15,18]. In this patient, the abdominopelvic ultrasound shows an empty uterus and a right adnexal complex mass, but it does not definitively indicate the exact location of the ectopic pregnancy. Therefore, the diagnosis of OEP was made intraoperatively and confirmed by histopathologic examination.
Surgery is the main modality of treatment for OEP, either laparotomy or laparoscopic surgery [1]. Laparoscopic surgery is becoming the preferred treatment over laparotomy since it has fewer complications and a shorter hospital stay [1,5,16]. Medical treatment with methotrexate (MTX) is controversial. There are reports of successful management of OEP with MTX [17]. However, Xin Zhou et al. report a trial of MTX treatment in three patients, which failed in all cases, and they were later managed surgically [1]. Our patient has been managed surgically by laparotomy since laparoscopic surgery is not available in our facility.
Conclusion
4
In conclusion, OEP is a rare potentially fatal condition. It is a diagnostic challenge since it is rare and mimics tubal ectopic pregnancy and complicated ovarian cysts. It should always be considered in patients presenting with amenorrhea, vaginal bleeding, and abdominal pain, particularly in those using an IUDs. Surgery is the mainstay of management, and histopathologic examination is crucial for confirming the diagnosis.
Abbreviations
ARTassisted reproductive technologiesIUDsintrauterine devicesOEPOvarian ectopic pregnancyPIDpelvic inflammatory diseaseMTXmethotrexateβ- HCGβ- human chorionic gonadotropin
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Ethical approval
The study was notified to the university ethics committee; but this is case report and it does not need a specific ethical approval.
Guarantor
Seblewengel Maru Wubalem
Shemsu Abraham Hussien
Funding
This work did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors*.*
Author contribution
- 1.Seblewengel Maru Wubalem: Conceptualization; Data curation; Resources; Visualization; riting – original draft; Writing – review and editing
- 2.Birhanu Kassie Reta: Data curation; Visualization; Writing – review and editing
- 3.Mihiret Adane Woldemichael: Data curation; Visualization; Writing – review and editing
- 4.Sara Alemnew Wedaj: Data curation; Visualization; Writing – review and editing
- 5.Shemsu Abraham Hussien: Data curation; Supervision; Visualization; Writing – original draft; Writing – review and editing
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shao M.Wang X.Zhou X.Case report: ovarian pregnancy, a rare but lethal condition: an analysis of 112 cases Front. Surg.102023106222810.3389/fsurg.2023.106222836874462 PMC 9982079 · doi ↗ · pubmed ↗
- 2Almahloul Z.Amro B.Nagshabandi Z.Alkiumi I.Hakim Z.Wattiez A.Tahlak M.Koninckx P.R.Ovarian pregnancy: 2 case reports and a systematic review J. Clin. Med.1232023113810.3390/jcm 1203113836769786 PMC 9917991 · doi ↗ · pubmed ↗
- 3Solangon S.A.Naftalin J.Jurkovic D.Ovarian ectopic pregnancy: clinical characteristics, ultrasound diagnosis and management Ultrasound Obstet. Gynecol.636202481582310.1002/uog.2754938031189 · doi ↗ · pubmed ↗
- 4Andrade A.G.Rocha S.Marques C.O.Ovarian ectopic pregnancy in adolescence Clin. Case Rep.311201591291510.1002/ccr 3.33626576271 PMC 4641473 · doi ↗ · pubmed ↗
- 5Hussain M.Rizzuto M.I.Macrae R.Laparoscopic management of ovarian ectopic pregnancy misdiagnosed at elective surgical termination of pregnancy: a report of two cases and review of the literature Gynecol. Surg.7201030330510.1007/s 10397-009-0470-x · doi ↗
- 6Sohrabi C.Mathew G.Maria N.Kerwan A.Franchi T.Agha R.A.The SCARE 2023 guideline: updating consensus Surgical C Ase R Eport (SCARE) guidelines Int. J. Surg. Lond. Engl.10952023113610.1097/JS 9.0000000000000373 PMC 1038940137013953 · doi ↗ · pubmed ↗
- 7Centers for Disease Control and Prevention (CDC)Ectopic pregnancy—United States, 1990–1992 MMWR Morb. Mortal. Wkly Rep.443199546487823895 · pubmed ↗
- 8Ghasemi Tehrani H.Hamoush Z.Ghasemi M.Hashemi L.Ovarian ectopic pregnancy: a rare case Iran. J. Reprod. Med.124201428128424976824 PMC 4071634 · pubmed ↗