Spontaneous Forearm Hemorrhage in a Patient With Polycystic Kidney Disease: A Case Report
Tomohiro Nakajima, Akihiro Tabata

TL;DR
A 73-year-old woman with polycystic kidney disease experienced a rare forearm hemorrhage, requiring surgical intervention.
Contribution
This case report highlights a rare complication of spontaneous forearm hemorrhage in a patient with polycystic kidney disease.
Findings
The patient had a history of brain hemorrhage and progressive renal failure requiring hemodialysis.
She developed a rare forearm hemorrhage, which was managed with hemostatic surgery.
The case emphasizes the need for vigilance in managing comorbidities in polycystic kidney disease patients.
Abstract
The patient is a 73-year-old woman. She had a brain hemorrhage at 53 years of age and underwent craniotomy and hematoma removal. At 55 years of age, she was treated for multiple renal cysts. An infection has spread to the existing renal cyst. The patient’s renal function gradually deteriorated, and she underwent hemodialysis at 56 years of age. At 58 years of age, an internal shunt was created using an autologous blood vessel in the left elbow fossa. Thereafter, she was hospitalized six times because of a cyst infection and received antibiotic treatment. At 72 years of age, she experienced a brain hemorrhage and received conservative treatment at our hospital. Presently, she presented with swelling in the left forearm. Upon further examination, bleeding was found in the left forearm muscles. Hemostatic surgery was performed under general anesthesia. Here, we report a rare case of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
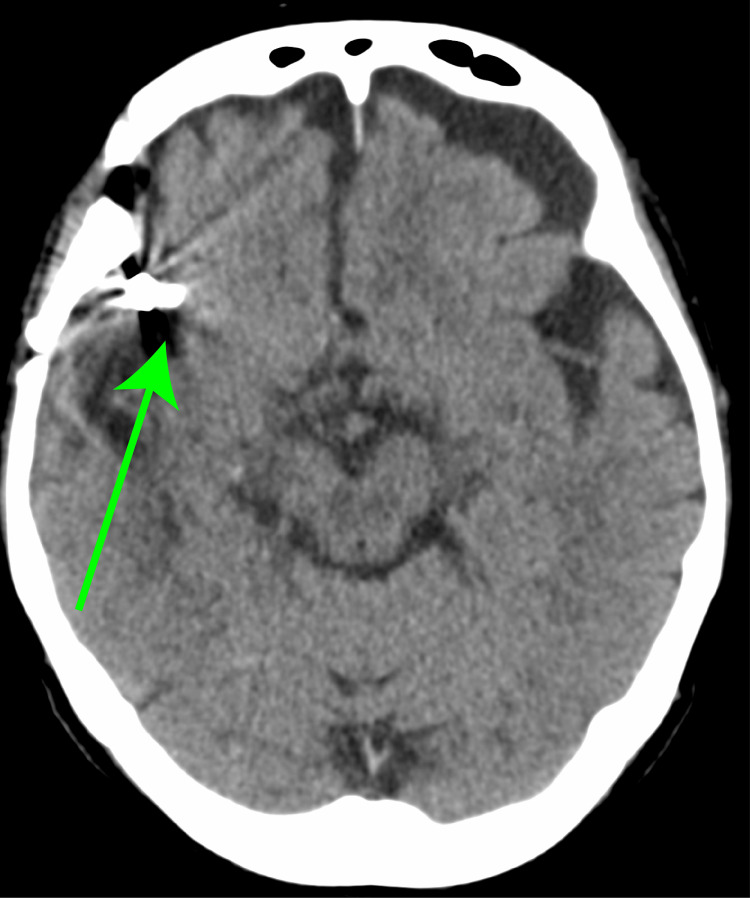 Figure 1
Figure 1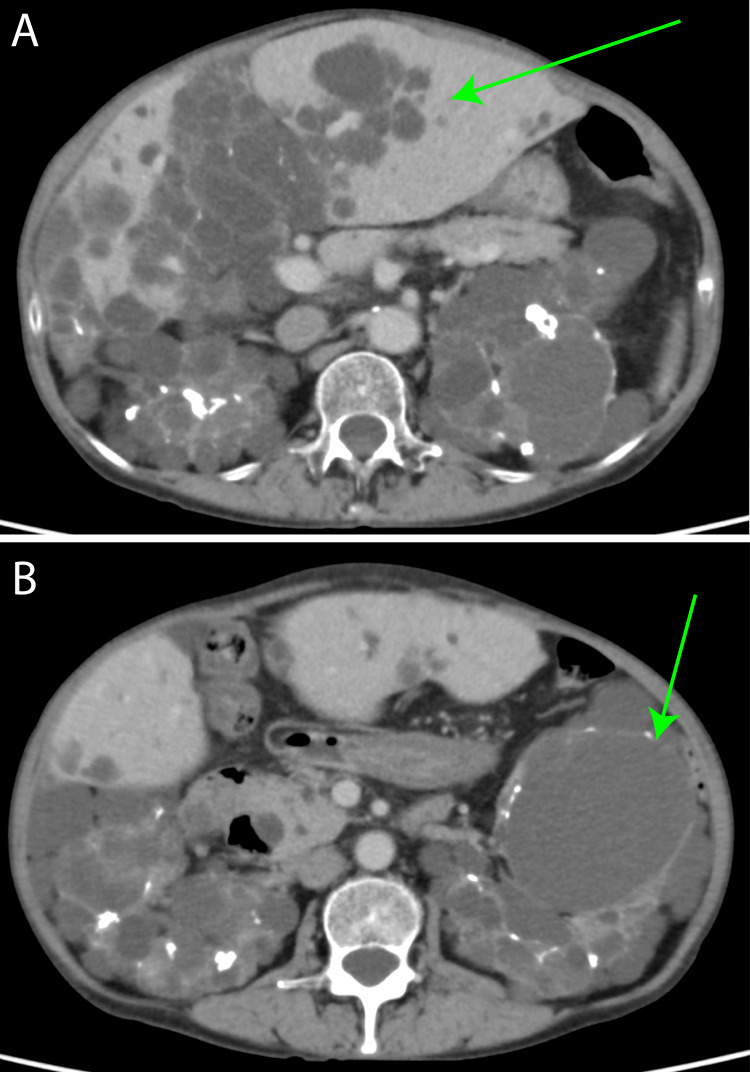 Figure 2
Figure 2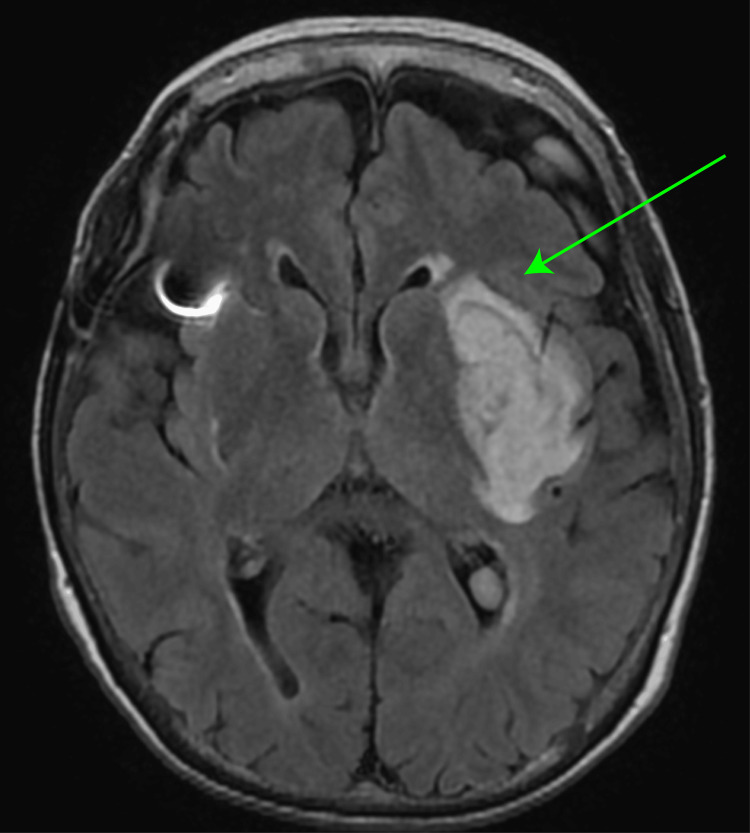 Figure 3
Figure 3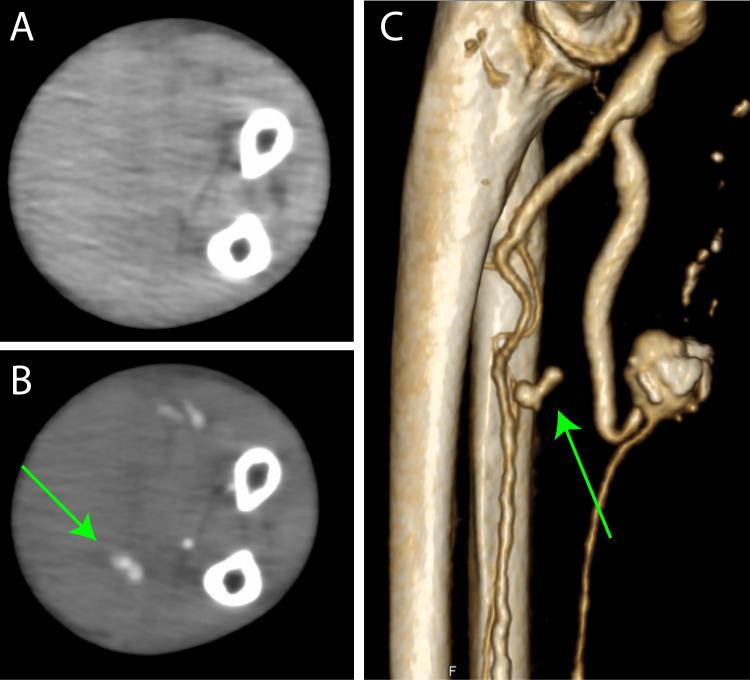 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenetic and Kidney Cyst Diseases · Fetal and Pediatric Neurological Disorders · Tuberous Sclerosis Complex Research
Introduction
Polycystic kidney disease (PKD) is among the most common inherited kidney disorders, with a reported prevalence of 1 in 400-1,000 individuals [1]. It is characterized by the progressive development of multiple renal cysts, leading to kidney enlargement and gradual loss of renal function. Its clinical manifestations include hypertension, hematuria, flank pain, and renal insufficiency. As the disease progresses, many patients eventually develop end-stage renal disease (ESRD) and require renal replacement therapy, such as hemodialysis or kidney transplantation; approximately 50% of patients with autosomal dominant PKD (ADPKD) develop ESRD by 60 years of age [2]. PKD is associated with an increased risk of bleeding due to vascular fragility and hypertension [3]. There are several reports of intracranial aneurysms, subarachnoid hemorrhage, and spontaneous bleeding events, such as intracystic hemorrhage and gross hematuria [4]. However, spontaneous bleeding from an arteriovenous (AV) fistula on the forearm is extremely rare in patients with PKD. Here, we report a rare case of active bleeding from an AV shunt arm that required surgical hemostasis in a patient with PKD.
Case presentation
The patient is a 73-year-old woman. She had a subarachnoid hemorrhage, at 53 years of age, and underwent craniotomy and hematoma removal surgery (Figure 1).
Brain computed tomography at the age of 53 years old.A clipping is observed in the right temporal lobe (green arrow).
At 55 years of age, she was treated for multiple renal cysts, which had been detected following an infection (Figure 2).
Contrast-enhanced computed tomography at the age of 55 years old.(A) Multiple cysts are observed in the liver and upper pole of the kidney (green arrow). (B) Numerous cysts are observed in the middle part of the kidney (green arrow).
The patient’s renal function gradually deteriorated, and she started undergoing hemodialysis at 56 years of age. An internal shunt was created using autologous blood vessels in the left forearm. At 58 years of age, an internal shunt was created using an autologous blood vessel in the left elbow fossa. Thereafter, she was hospitalized six times because of a cyst infection and received antibiotic treatment. At 72 years of age, she experienced a cerebral hemorrhage and received conservative treatment at our hospital (Figure 3).
Magnetic resonance image at the age of 72 years old.Magnetic resonance imaging reveals a high-intensity lesion in the left thalamus, indicating a brain hemorrhage (green arrow).
Recently, she presented with swelling in the left forearm. Upon further examination, bleeding into the left forearm muscle was found. Contrast-enhanced computed tomography (CT) revealed swelling in the left arm and rupture of the muscle branches (Figure 4). Because it was a difficult area to stop the bleeding, and the swelling of the left hand progressed, we had no choice but to consider surgery.
Preoperative images at the age of 72 years old.A computed tomography (CT) image of the left forearm.(A) Plain CT: Swelling of the left forearm is observed. (B) Venous phase: Venous bleeding is observed (green arrow). (C) Volume rendering image: Venous bleeding is observed (green arrow).
Under general anesthesia, a 10 cm skin incision was made on the left forearm, and hemostatic surgery was performed. The vein that flowed into the muscle was partially ruptured, and the site was clipped to stop the bleeding.
A drain was placed, the skin was closed, and surgery was completed. Thereafter, the bleeding subsided, and the swelling in the left forearm improved.
Discussion
Here, we report a rare case of unexpected venous bleeding from a left forearm hemodialysis shunt in a patient with PKD. Although access to hemodialysis is crucial for patients with PKD progressing to ESRD, reports of shunt-related complications, particularly venous bleeding, are scarce. In this instance, a patient with a prolonged history of PKD-induced renal failure underwent left forearm AV fistula creation and subsequently experienced spontaneous venous bleeding, without any evident trauma or infection.
PKD is a systemic disease that causes cyst formation in the kidneys and other organs [5]. Vascular wall fragility is a common characteristic of patients with PKD, increasing the risk of bleeding complications at various locations, including cerebral aneurysms, abdominal aortic aneurysms, and gastrointestinal cystic bleeding [6]. Therefore, venous bleeding from hemodialysis shunts may be attributable to PKD-related vascular wall fragility. Furthermore, renal dysfunction in PKD can lead to coagulopathy. Although the patient’s prothrombin time-international normalized ratio (PT-INR) is within normal limits, other coagulation abnormalities, such as platelet dysfunction, are included [7]. Additionally, PKD can be associated with vascular anatomical variations; although no gross abnormalities were observed, subtle variations may have played a role [8].
Provided the difficulty in achieving hemostasis, surgical intervention is necessary. Although the literature on managing such bleeding in patients with PKD is limited, surgical hemostasis appears to be a viable option. This case highlights the importance of considering the unique characteristics of patients with PKD in hemodialysis access management. Further research is necessary to identify the risk factors and establish optimal treatment strategies for this rare complication. Future studies are needed to further investigate the risk factors of hemodialysis shunt bleeding in patients with PKD, and clinical studies are needed to determine the best treatment plans for this complication.
Conclusions
Although access to hemodialysis is essential for patients with PKD and ESRD, bleeding from the shunt limb is uncommon. PKD is a systemic disease that predisposes patients to bleeding complications through various mechanisms, including vascular fragility and coagulopathy. Surgical hemostasis is a viable treatment option for intractable bleeding. This report emphasizes the importance of considering the unique characteristics of patients with PKD in hemodialysis access management and provides valuable insights for the clinical management of similar cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Autosomal dominant polycystic kidney disease Lancet Cornec-Le Gall E Alam A Perrone RD 91993539320193081951810.1016/S 0140-6736(18)32782-X · doi ↗ · pubmed ↗
- 2Determinants of disease progression in autosomal dominant polycystic kidney disease J Pers Med Kebede MA Mengistu YT Loge BY Eshetu MA Shash EP Wirtu AT Gemechu JM 9361420243933819010.3390/jpm 14090936 PMC 11433103 · doi ↗ · pubmed ↗
- 3Spontaneous coronary artery dissection in patients with autosomal dominant polycystic kidney disease: a systematic review of the literature J Pers Med Milutinovic S Bell A Jancic P 7021420243906395610.3390/jpm 14070702 PMC 11278354 · doi ↗ · pubmed ↗
- 4A spontaneous extracranial internal carotid artery dissection with autosomal dominant polycystic kidney disease: a case report and literature review Medicina (Kaunas) Izumo T Ogawa Y Matsuo A 5067958202210.3390/medicina 58050679 PMC 914391435630097 · doi ↗ · pubmed ↗
- 5Novel PKD 1 mutation (c.G 10086 T) drives high intracranial aneurysm risk in autosomal dominant polycystic kidney disease Eur J Neurol Gao L Lin M Wu C 032202510.1111/ene.70086 PMC 1184042539973757 · doi ↗ · pubmed ↗
- 6Vascular complications in autosomal dominant polycystic kidney disease Kidney Int Li J He H Li X Shu C 2409820203257148410.1016/j.kint.2020.01.013 · doi ↗ · pubmed ↗
- 7Compliance with a healthful plant-based diet is associated with kidney function in patients with autosomal dominant polycystic kidney disease Nutrients Heo S Han M Ryu H 27491620243920388510.3390/nu 16162749 PMC 11356780 · doi ↗ · pubmed ↗
- 8KDIGO 2025 clinical practice guideline for the evaluation, management, and treatment of autosomal dominant polycystic kidney disease (ADPKD): executive summary Kidney Int Torres VE Ahn C Barten TR 23425410720253984874610.1016/j.kint.2024.07.010 · doi ↗ · pubmed ↗