A Schwannoma-Hemangioma Composite Tumor as a Very Uncommon Cause of a Chest Wall Tumor in a Teenage Patient: A Case Report
Ewa A Bieganska, Jakub Noskiewicz, Zaneta Slowik-Moczydlowska

TL;DR
A rare composite tumor involving a teenage patient's chest wall is reported, emphasizing the need for accurate diagnosis and further research.
Contribution
This case report presents a rare pediatric schwannoma-hemangioma composite tumor in the chest wall, expanding clinical awareness of this condition.
Findings
A 14-year-old male was diagnosed with a schwannoma-hemangioma composite tumor on the chest wall.
Surgical removal and histopathologic analysis confirmed the tumor's composite nature.
The patient had an uneventful recovery with no recurrence at three months.
Abstract
Schwannoma-hemangioma composite tumors are extremely rare, with most cases described in the head and neck of adult patients. Pediatric cases involving the chest wall have not been widely reported and, therefore, present diagnostic and therapeutic challenges. We describe the case of a 14-year-old male patient who presented with a painless nodular lesion on the chest wall. After imaging studies and laboratory analysis, the consulting oncologist recommended the surgical removal of the tumor due to the indeterminate nature of the lesion. Histopathologic analysis of the excised tissue confirmed a composite schwannoma-hemangioma tumor. The patient recovered uneventfully postoperatively with no recurrence or complications at the three-month follow-up. This case highlights the importance of considering rare composite tumors in the differential diagnosis of pediatric chest wall lesions. Accurate…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
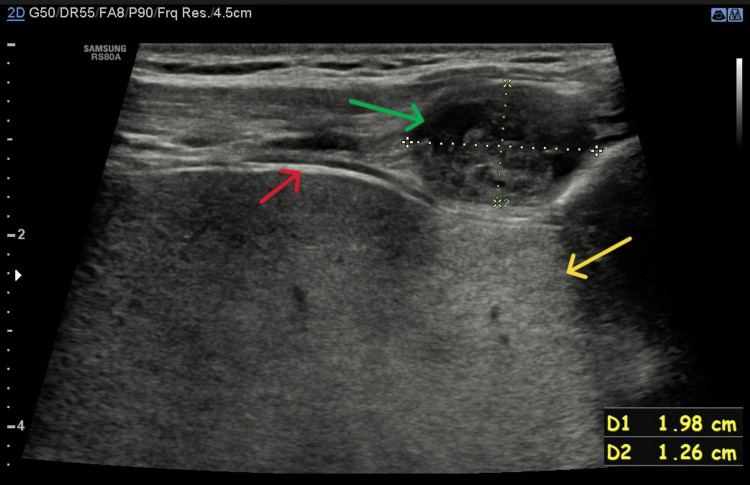 Figure 1
Figure 1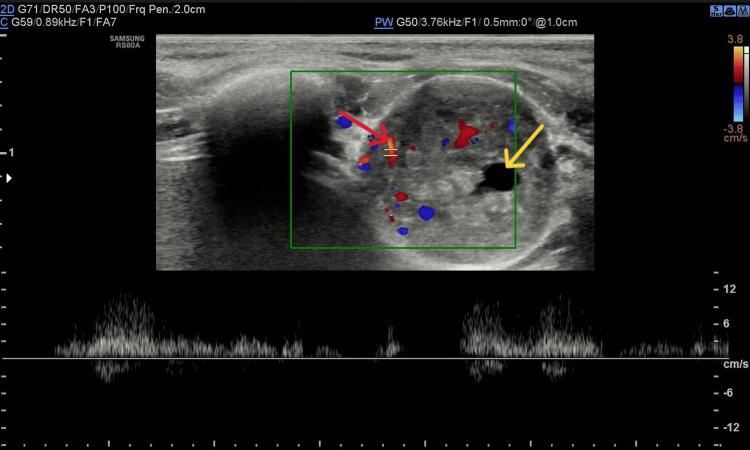 Figure 2
Figure 2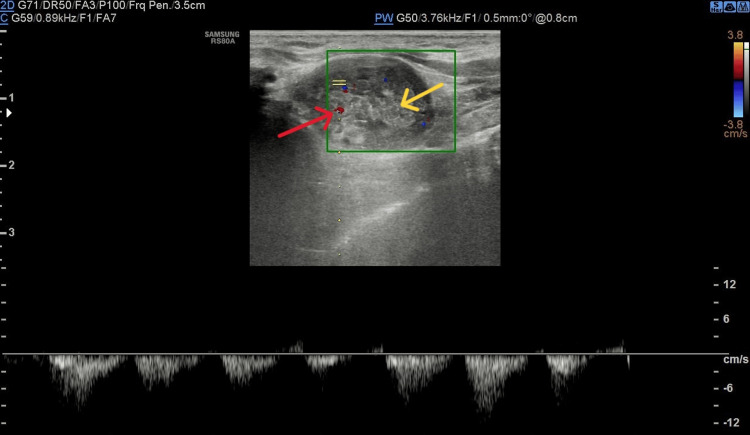 Figure 3
Figure 3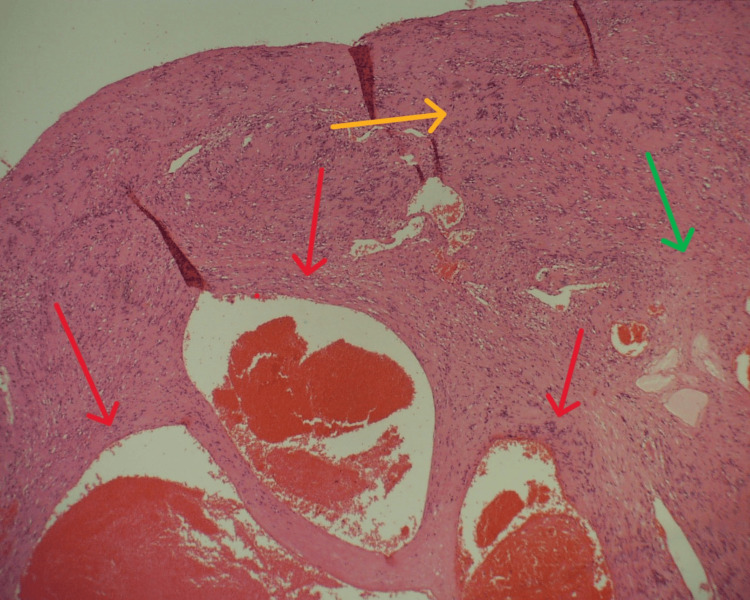 Figure 4
Figure 4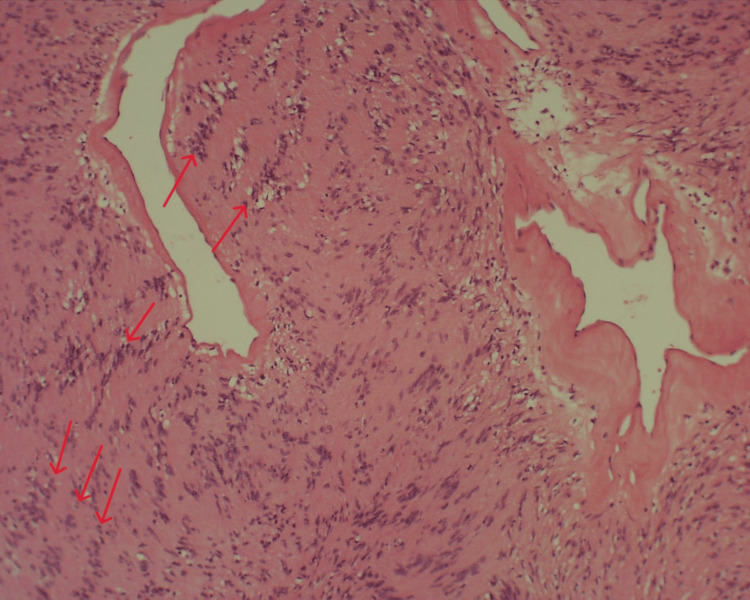 Figure 5
Figure 5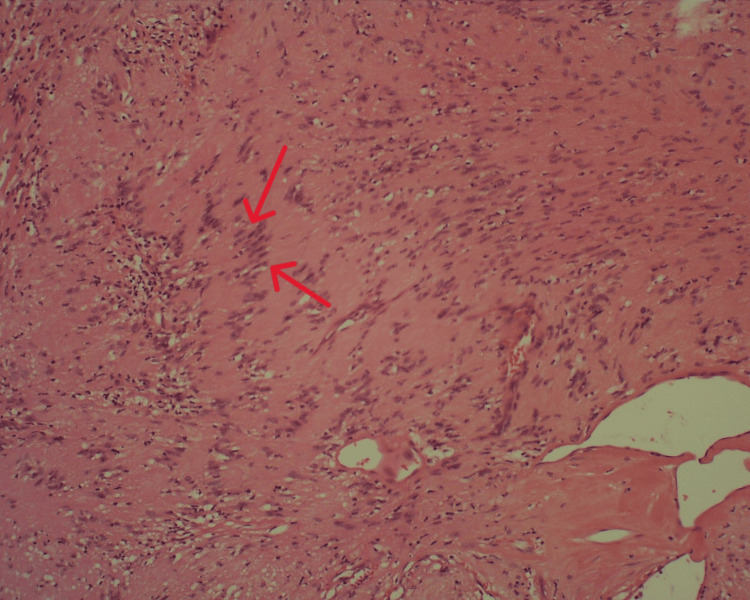 Figure 6
Figure 6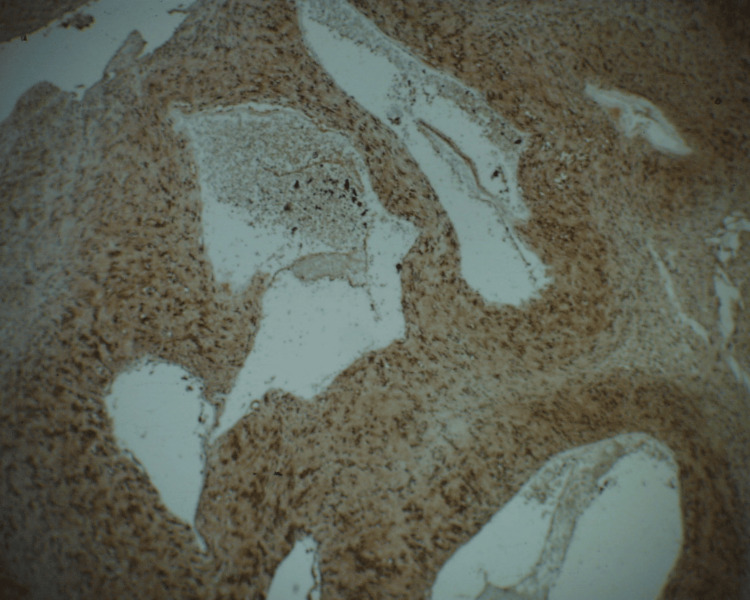 Figure 7
Figure 7| Marker | Results | Reference values | Units of measurement |
| AFP | 1.5 | <8 | ng/ml |
| β-hCG | <0.10 | <2.0 (for males) | mIU/ml |
| LDH | 177 | 120-300 | U/l |
| NSE | 11.9 | 9-12.4 | ng/ml |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEar and Head Tumors · Neurofibromatosis and Schwannoma Cases · Vascular Malformations and Hemangiomas
Introduction
Peripheral nerve sheath tumors and hemangiomas are common benign soft tissue tumors. Sporadic schwannomas account for approximately 89% of all peripheral nerve sheath tumors. They are most commonly found in the upper extremities, head and neck, trunk, and flexor surfaces of the lower extremities. These tumors are typically diagnosed in people between the ages of 20 and 50, with no gender or ethnic predilection [1,2].
Hemangiomas are the most commonly diagnosed benign soft tissue tumors in children. They occur predominantly in the head and neck region [3].
Despite the high prevalence of both tumor types, their simultaneous occurrence either as a composite tumor (known as conjoined association) or as separate tumors in close proximity but different locations (also known as discrete association) is extremely rare. According to the literature, only about 40 cases of such occurrences have been documented, mainly in the head and neck region [4-6]. Because of their rarity, the diagnosis and management of these tumors are clinical challenges.
Another critical clinical consideration is the occurrence of chest wall tumors in pediatric patients. They comprise a heterogeneous group of lesions, ranging from benign to malignant, and may arise from osseous, cartilaginous, or soft tissue structures. Common benign tumors include lipomas, fibromas, and chondromas, while malignant lesions may consist of peripheral primitive neuroectodermal tumors (PNETs), osteosarcomas, rhabdomyosarcomas, and metastases. Imaging plays a critical role in the initial assessment, with CT and MRI providing valuable information on lesion composition, extent, and potential invasiveness. Ultrasound is also a very useful diagnostic test, characterized by good resolution in pediatric patients and increased radiological safety, which is important for this group. Despite advances in imaging, definitive diagnosis often requires histopathological confirmation due to overlapping radiological features. Although chest wall tumors as a group are rare, a significant proportion are malignant and require increased oncological vigilance [7-9].
The purpose of this report is to present the case of a 14-year-old patient who was admitted to the hospital with a small nodular lesion in the chest wall region. Following surgical excision, histopathological analysis revealed features consistent with a schwannoma-hemangioma composite tumor. Given the rarity of this tumor type, particularly in the pediatric population, publishing this case aims to improve understanding of the diagnosis and management of such tumors. Such knowledge may be of benefit to pediatric surgeons and pathologists in their clinical practice.
Case presentation
A 14-year-old previously healthy, male patient presented to the pediatric surgery clinic with the chief complaint of painless swelling in the chest region. The patient had been initially evaluated during a diagnostic workup at the oncology clinic after a nodular lesion was noted between the 10th and 11th ribs on the left side. The lesion was asymptomatic and was discovered incidentally during an outpatient evaluation for a nodule in the breast region, where glandular tissue was identified.
Physical examination revealed a palpable, mobile nodule in the chest wall measuring approximately 2×3 cm, located along the left midaxillary line between the 10th and 11th intercostal spaces, and palpable axillary lymph nodes on the right side. No other abnormalities were noted.
During the first diagnostic stay in oncology, a differential diagnosis was made to determine whether the lesion was benign, such as a lipoma or hemangioma, or whether it could be a malignant tumor such as PNETs, sarcomas, or very rare but possible germ cell tumors. To this end, imaging studies were ordered, chest X-ray, abdominal ultrasound, chest wall ultrasound, and laboratory tests, including the available tumor markers that could indicate the aforementioned PNET or germ cell tumors. The results of the markers are shown in Table 1.
Chest X-ray and abdominal ultrasound were unremarkable. Ultrasound of the chest wall lesion showed a focal mass measuring 20×13 mm. The lesion was described as containing both solid and cystic elements, with heterogeneous echotexture, posterior acoustic enhancement, and visible arterial flow within the lesion (pictures from ultrasound examination: Figures 1-3). Previously palpated axillary lymph nodes were normal on ultrasound.
Image from ultrasound examination: lesion with cystic elements (green arrow), visceral pleura (red arrow), and posterior acoustic enhancement (yellow arrow) is presented
Image from Doppler ultrasonography: lesion with arterial flow (red arrow) and cystic elements (yellow arrow) is presented
Image from Doppler ultrasonography: apart from arterial flow (red arrow) in the lesion, solid elements with heterogeneous echostructure (yellow arrow) are presented
Since the ultrasound image did not allow a clear differentiation of the lesion, as it did not show features characteristic of benign tumors such as lipoma or hemangioma, and the nodule did not show radiological features of malignancy, and tumor markers were negative, it was decided to remove the lesion in its entirety for pathomorphological examination of the lesion.
The lesion was excised under general anesthesia. Intraoperatively, a well-demarcated, encapsulated mass was observed with no connection to adjacent bone, muscle, or pleura. The lesion, which was more cohesive than the surrounding tissues and cream in color, was completely excised together with its capsule. The procedure was uneventful, with typical closure of the surgical site. The postoperative course was uncomplicated, and the patient was discharged on the first postoperative day and referred to outpatient care.
Histopathological examination revealed features consistent with a schwannoma, characterized by the expression of S100 protein and CD56 antigen, together with dilated vascular spaces typical of a cavernous hemangioma (Figures 4-7). No other immunohistochemistry markers were performed. The tumor was removed in its entirety, and the surgical margins were negative. The overall findings support the diagnosis of a composite schwannoma-hemangioma tumor.
Histological preparation, HE staining, 40× magnification. Part of the lesion indicated by red arrows is comprised of dilated congested thin-walled vessels, characteristic for cavernous hemangioma. Also, the characteristic biphasic structure can be seen: Antoni A (hypercellular, yellow arrow) and Antoni B (hypocellular, green arrow) areas
Histological preparation, HE staining, 100× magnification. Characteristic areas of nuclear palisading around fibrillary process (Verocay bodies) are indicated with red arrows
Histological preparation, HE staining, 200× magnification. Verocay bodies are indicated with red arrows
Immunostain for S100 shows nuclear and cytoplasmic staining in the cells, 200× magnificationStrong and diffuse staining pattern is observed in the picture
Discussion
The case of a 14-year-old patient with a composite schwannoma-hemangioma tumor in the chest wall is noteworthy because of the rarity of such lesions and their atypical location. Previously reported cases of coexisting neural and vascular tumors have mainly involved adult patients, with lesions located in the head and neck region, affecting either the central nervous system or cranial nerves. In most cases, the neural tumors were schwannomas, with neurofibromas and gliomas being less commonly reported [5]. Although the coexistence of two different tumor types in a single location may be coincidental, the literature suggests that complex molecular mechanisms are more likely to underlie the simultaneous development of schwannomas and hemangiomas within a single tumor.
Proposed pathways of tumorigenesis include loss of Merlin-mediated inhibition of the MAP kinase MEK/ERK cascade, abnormalities in the PI3K/mTOR pathway, interactions between vascular endothelial growth factor (VEGF) secreted by schwannoma cells and endothelial cells, and KRIT1 gene mutations [5,6].
Identifying the molecular mechanisms responsible for the development of such tumors could be crucial in determining therapeutic strategies, particularly pharmacological approaches, in cases where complete surgical resection is not feasible due to the location of the tumor.
Another important consideration is the differential diagnosis of chest wall tumors in children, as a significant proportion of these lesions are malignant, such as Ewing's sarcoma, lymphoma, or metastatic tumors. According to review articles, benign tumors such as chondromas, hemangiomas, or the mixed tumor described in this report represent only a small percentage of all chest wall tumors in this age group [7-9].
Both van den Berg et al. [7] and La Quaglia [10] emphasized that although benign chest wall tumors are often incidental findings, typically identified by imaging studies, definitive diagnosis usually requires histopathological examination. Therefore, it is emphasized that in cases of pediatric chest wall tumors, biopsy or surgical resection should always be considered to establish the nature of the lesion and determine the optimal therapeutic approach.
Conclusions
This case highlights the importance of considering rare complex tumors in the differential diagnosis of subcutaneous and chest wall lesions, even in pediatric patients. Apart from diagnostic imaging like CT, MRI, and ultrasound, accurate histopathological and immunohistochemical evaluation is essential for correct diagnosis and, thus, therapeutic management. The publication of this case is a valuable addition to the literature on schwannoma-hemangioma tumors and may be helpful in the diagnosis and management of similar cases in the future.
Further studies and case reports are needed to gain a better understanding of the etiology, clinical course, and optimal management strategies for complex tumors of this type.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Peripheral nerve tumors: management strategies and molecular insights J Neurooncol Bhattacharyya AK Perrin R Guha A 3353496920041552709910.1023/b:neon.0000041891.39474.cb · doi ↗ · pubmed ↗
- 2Imaging of peripheral nerve sheath tumors with pathologic correlation: pictorial review Eur J Radiol Pilavaki M Chourmouzi D Kiziridou A Skordalaki A Zarampoukas T Drevelengas A 2292395220041554490010.1016/j.ejrad.2003.12.001 · doi ↗ · pubmed ↗
- 3Capillary infantile hemangiomas Stat Pearls [Internet] Koka K Zeppieri M Patel BC Treasure Island (FL)Stat Pearls Publishing 2024 https://pubmed.ncbi.nlm.nih.gov/30855837/
- 4Reappraising schwannoma-hemangioma composite tumors as synchronous tumorigenic entities with conjoined histomorphology: a case report Cureus Ramkumar S 013202110.7759/cureus.20724 PMC 871070434966629 · doi ↗ · pubmed ↗
- 5Reviewing schwannoma-hemangioma composite tumors with their tumorigenetic molecular pathways and associated syndromic manifestations Cureus Ramkumar S 013202110.7759/cureus.19839 PMC 861010334824953 · doi ↗ · pubmed ↗
- 6Cavernous malformation within a schwannoma: review of the literature and hypothesis of a common genetic etiology Acta Neurochir (Wien) Feiz-Erfan I Zabramski JM Herrmann LL Coons SW 64765214820061645004610.1007/s 00701-005-0716-y · doi ↗ · pubmed ↗
- 7Management of tumors of the chest wall in childhood: a review J Pediatr Hematol Oncol van den Berg H van Rijn RR Merks JH 2142213020081837628410.1097/MPH.0b 013e 318162 bd 54 · doi ↗ · pubmed ↗
- 8Chest wall tumors in infants and children Semin Pediatr Surg Shamberger RC Grier HE 26727631994 https://pubmed.ncbi.nlm.nih.gov/7850367/7850367 · pubmed ↗