Impact of Education and Gender on Knowledge, Attitudes, and Practices Toward Vitamin D Among the Lebanese Population With Emphasis on Young Adults
Suzana Salhab, Ibrahim A Srour, Imtithal Sheet, Lamis Karaki, Hadi Haddad, Mohamad Nour Zeineddine, Samer Sakr

TL;DR
This study examines how education and gender influence knowledge, attitudes, and practices about vitamin D among young Lebanese adults.
Contribution
The study provides new insights into vitamin D-related knowledge and behaviors in a sun-rich but understudied population.
Findings
Most participants had sufficient knowledge about vitamin D sources, with sunlight seen as most crucial.
Over 90% were willing to take supplements or undergo testing for vitamin D deficiency.
Despite good knowledge, over half expressed concerns about their vitamin D levels.
Abstract
Background Vitamin D deficiency is a growing global health concern that affects populations, even in sun-rich regions such as Lebanon. Despite abundant sunlight, limited research has explored the knowledge, attitudes, and practices (KAP) related to vitamin D among young Lebanese adults. Study design This study employed an online quantitative cross-sectional design. Methods A self-administered online questionnaire distributed over six months (from August 2023 to January 2024) collected data on the participants' demographic characteristics, as well as their knowledge, attitudes, and practices related to vitamin D. Results Most participants (75.7%) had sufficient knowledge about vitamin D sources. The internet and physicians emerged as the dominant sources, cited by 175 participants, which represented 17.6% of the total responses related to vitamin D knowledge sources. Sunlight was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
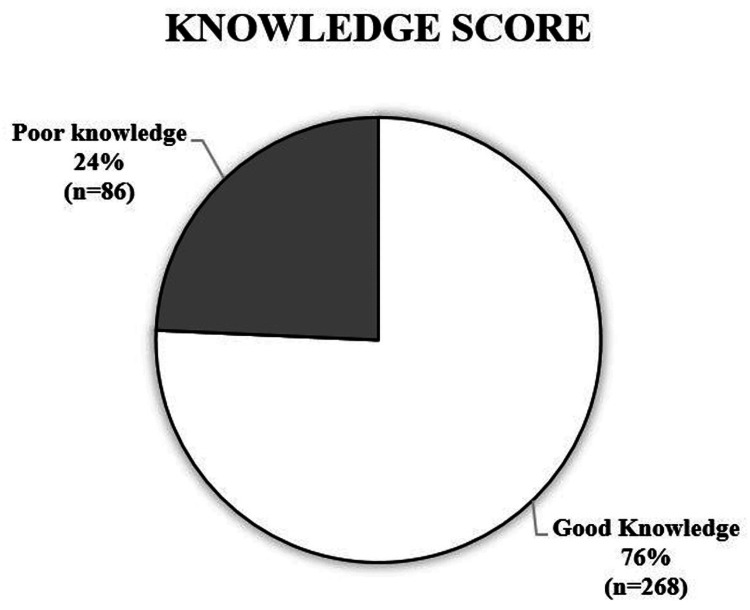 Figure 1
Figure 1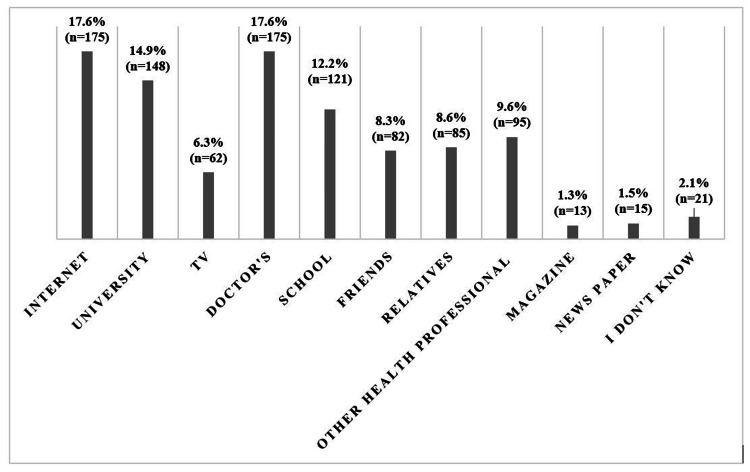 Figure 2
Figure 2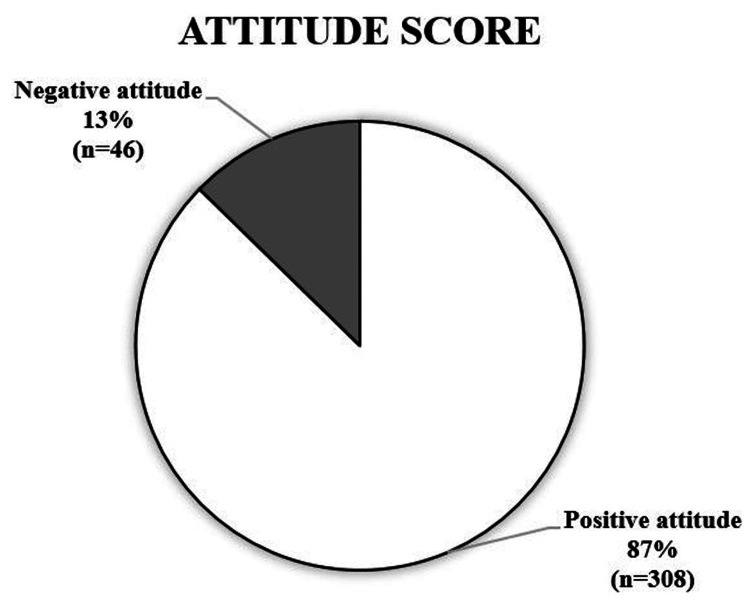 Figure 3
Figure 3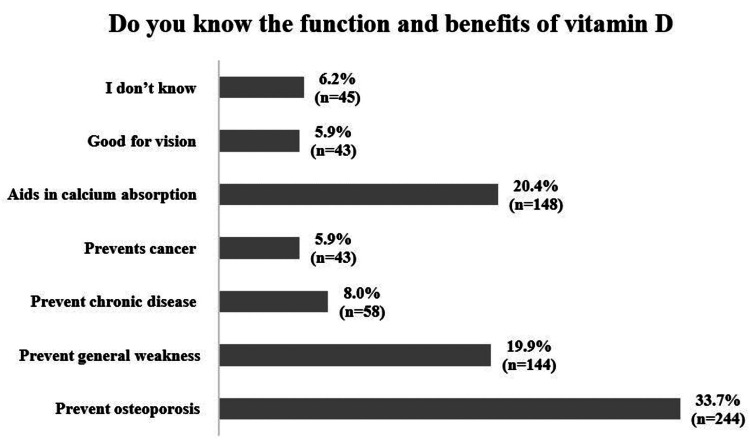 Figure 4
Figure 4| Description | N (%) | Knowledge Score | Attitude Score |
| Age (years) | P=0.239 | P=0.583 | |
| 18-23 | 228 (64.4%) | ||
| 24-29 | 75 (21.2%) | ||
| 30-35 | 30 (8.5%) | ||
| 36-41 | 12 (3.4%) | ||
| 42-47 | 7 (2.7%) | ||
| 48-53 | 2(0.6%) | ||
| Gender | P=0.002 | P=0.001 | |
| Male | 113 (31.9%) | ||
| Female | 241 (68.1%) | ||
| If you are a woman, do you wear a scarf? | |||
| Yes | 148 (41.8%) | ||
| No | 116 (32.8%) | ||
| Marital status | P=0.118 | P=0.173 | |
| Unmarried | 298 (84.2%) | ||
| Married | 56 (15.8%) | ||
| Education level | P=0.001 | P=0.776 | |
| High school | 55 (15.5%) | ||
| Bachelor's degree | 187 (58.8%) | ||
| Diploma | 36 (10.2%) | ||
| Master's degree | 31 (8.8%) | ||
| PhD | 5 (1.45%) | ||
| Others | 40 (11.3%) | ||
| Occupation (multiple responses) | P=0.192 | P=0.745 | |
| Indoor employed | 124 (29.5%) | ||
| Outdoor employed | 39 (9.3%) | ||
| Student | 204 (48.5%) | ||
| Retired | 0 (0%) | ||
| Unemployed | 54 (12.8%) | ||
| Skin color | |||
| Fair or pale | 51 (14.4%) | ||
| Fair/light to beige | 213 (60.2%) | ||
| Light brown/olive | 88 (23.2%) | ||
| Dark brown | 8 (2.3%) |
| Description | N (%) | |
| Knowledge questions regarding vitamin D | Have you ever heard or learned about vitamin D? | |
| Yes | 328 (92.7%) | |
| No | 26 (7.3%) | |
| Where did you hear or learn about vitamin D? (multiple responses) | ||
| Newspaper | 15 (1.5%) | |
| Magazine | 13 (1.3%) | |
| TV | 62 (6.3%) | |
| Doctors | 175 (17.6%) | |
| Friends | 82 (8.3%) | |
| Relatives | 85 (8.6%) | |
| School | 121 (12.2%) | |
| University | 148 (14.9%) | |
| Internet | 175 (17.6%) | |
| Other health professionals | 95 (9.6%) | |
| I do not know | 21 (2.1%) | |
| Is vitamin D present in the body? | ||
| Yes | 285 (80.5%) | |
| No | 33 (9.3%) | |
| I do not know | 36 (10.2%) | |
| Do you know the function and benefits of vitamin D? (multiple responses) | ||
| Prevents osteoporosis | 244 (33.7%) | |
| Prevents general weakness | 144 (19.9%) | |
| Prevents chronic disease | 58 (8%) | |
| Prevents cancer | 43 (5.9%) | |
| Aids in calcium absorption | 148 (20.4%) | |
| Good for vision | 43 (5.9%) | |
| I do not know | 45 (6.2%) | |
| Where do you think the body gets vitamin D? (multiple responses) | ||
| Diet | 61 (11%) | |
| Exposure to the sun | 176 (31.6%) | |
| Food supplement | 109 (19.6%) | |
| All the above | 198 (35.5%) | |
| I do not know | 13 (2.3%) | |
| How much time do you need to spend in the sun to get enough vitamin D? | ||
| <10 minutes | 48 (13.6%) | |
| 10-20 minutes | 174 (49.2%) | |
| 30-60 minutes | 88 (24.9%) | |
| >1 hour | 38 (10.7%) | |
| Missing | 6 (1.7%) | |
| Meals alone can provide sufficient levels of vitamin D | ||
| Yes | 45 (12.7%) | |
| No | 252 (71.2%) | |
| I do not know | 57 (16.1%) | |
| What type of food is a good source of vitamin D? (multiple responses) | ||
| Vegetables and fruits | 95 (15.5%) | |
| Milk | 121 (19.8%) | |
| Fatty fish: salmon | 181 (29.6%) | |
| Olive oil | 43 (7.1%) | |
| Eggs | 99 (16.2%) | |
| I do not know | 72 (11.8%) | |
| Aware of normal serum vitamin D levels | ||
| Yes | 166 (46.9%) | |
| No | 188 (53.1%) | |
| What is the normal level of vitamin D (ng mL-1)? | ||
| <12 | 13 (3.7%) | |
| <20 | 32 (9%) | |
| 20-50 | 142 (40.1%) | |
| I do not know | 167 (47.2%) | |
| What are the daily needs for vitamin D (IU)? | ||
| 200 IU | 39 (11%) | |
| 600 IU | 88 (24.9%) | |
| 800 IU | 16 (4.5%) | |
| I do not know | 211 (59.6%) | |
| What are the causes of vitamin D deficiency? (multiple responses) | ||
| Hereditary | 90 (12.3%) | |
| Less exposure to the sun | 283 (38.6%) | |
| Lack of eating vitamin D-rich food | 260 (35.4%) | |
| Kidney disease | 49 (6.7%) | |
| Respiratory disease | 8 (1.1%) | |
| I do not know | 43 (5.9%) | |
| Complications for vitamin D deficiency (multiple responses) | ||
| Osteoporosis | 281 (32.4%) | |
| Hair loss | 212 (24.4%) | |
| Depression | 162 (18.7%) | |
| Acne | 66 (7.6%) | |
| Obesity | 50 (5.8%) | |
| Cancer | 31 (3.6%) | |
| Eczema | 22 (2.5%) | |
| Blindness | 20 (2.3%) | |
| Peptic ulcer | 24 (2.7%) | |
| Attitude questions regarding vitamin D | Vitamin D is vital for overall health | |
| Yes | 352 (99.4%) | |
| No | 2 (0.6%) | |
| I like to expose myself to sunlight | ||
| Yes | 292 (82.5%) | |
| No | 62 (17.5%) | |
| The exposure to sunlight is harmful to the skin | ||
| Yes | 207 (58.5%) | |
| No | 147 (41.5%) | |
| I am concerned that my current vitamin D levels might be too low | ||
| Yes | 201 (56.8%) | |
| No | 153 (43.2%) | |
| Interested to know about vitamin D deficiency-associated symptoms | ||
| Yes | 31.7 (89.5%) | |
| No | 37 (10.5%) | |
| I am willing to undergo a test for vitamin D if a medical condition demands it | ||
| Yes | 326 (92.1%) | |
| No | 28 (7.9%) | |
| Vitamin D-related practices | Have you ever examined your vitamin D level? | |
| Yes | 207 (58.5%) | |
| No | 147 (41.5%) | |
| Do you take food supplements or a multivitamin containing vitamin D? | ||
| Yes | 193 (54.5%) | |
| No | 161 (45.5%) | |
| If no, what is the primary reason for not taking vitamin D? | ||
| Never thought about it | 116 (32.8%) | |
| Feels getting enough vitamin D from diet | 32 (9%) | |
| Feels getting enough vitamin D from the sun | 23 (6.5%) | |
| I prefer not to take any supplements/vitamins | 30 (8.5%) | |
| Missing | 153 (43.2%) | |
| If yes, what is the vitamin D dose of the supplement? | ||
| <1000 IU | 62 (17.5%) | |
| 1000 IU and over | 81 (22.9%) | |
| I do not know | 144 (40.7%) | |
| Missing | 67 (18.9%) | |
| Motivation for starting to take vitamin D | ||
| A doctor or health professional recommended | 209 (59%) | |
| A friend or family member recommended | 30 (8.5%) | |
| Read about vitamin D on the internet or in a book/magazine | 42 (11.9%) | |
| Someone else in the family is taking it | 32 (9%) | |
| Missing | 41 (11.6%) | |
| Previously investigated vitamin D serum levels among family members | ||
| Yes | 147 (41.5%) | |
| No | 207 (58.5%) | |
| If yes, what was the result? | ||
| Normal vitamin D levels | 27 (7.6%) | |
| Vitamin D deficiency | 122 (34.5%) | |
| Excess vitamin D level | 1 (0.3%) | |
| I do not know | 91 (25.7%) | |
| Missing | 113 (31.9%) | |
| How do you feel about sun exposure? | ||
| I like getting exposed to the sun all the time | 56 (15.8%) | |
| I like getting exposed to the sun sometimes | 220 (62.1%) | |
| I rarely get exposed to the sun | 40 (11.3%) | |
| I avoid getting exposed to the sun | 28 (7.9%) | |
| I do not know | 10 (2.9%) | |
| What time do you prefer to be exposed to the sun? | ||
| Early morning | 170 (47.8%) | |
| Afternoon | 70 (19.7%) | |
| At noon | 63 (17.7%) | |
| I avoid sunlight | 24 (6.7%) | |
| I usually go out at night but not during the day | 11 (3.1%) | |
| I do not know | 16 (4.4%) | |
| Missing | 2 (0.6%) | |
| Which season do you like to be exposed to the sun? | ||
| Summer | 92 (25.8%) | |
| Autumn | 20 (5.6%) | |
| Spring | 93 (26.1%) | |
| Winter | 70 (19.7%) | |
| All year | 79 (22.2%) | |
| Missing | 2 (0.6%) | |
| How frequently are you exposed to the sun? (times per week) | ||
| 0-1 | 53 (14.6%) | |
| 2-3 | 116 (32.6%) | |
| >3 | 138 (38.7%) | |
| I do not know | 48 (13.5%) | |
| Missing | 2 (0.6%) | |
| Duration of sun exposure | ||
| 15 minutes or less | 147 (41.3%) | |
| 15-29 minutes | 72 (20.2%) | |
| 30-60 minutes | 50 (14%) | |
| More than an hour | 42 (11.8%) | |
| I do not know | 45 (12.7%) | |
| What do you use most often as protection from the sun? | ||
| Umbrella | 7 (2%) | |
| Sunscreen | 205 (57.6%) | |
| Hat | 35 (9.8%) | |
| Do not use any protection | 101 (28.4%) | |
| I wear a scarf, and that is enough for me | 6 (1.7%) | |
| Missing | 2 (0.6%) | |
| Do you use sunscreen products that contain SPF>15? | ||
| Yes | 195 (54.8%) | |
| No | 115 (32.3%) | |
| I do not know | 44 (12.3%) | |
| Missing | 2 (0.6%) | |
| At what season do you prefer to use sunscreen? | ||
| Summer | 173 (48.6%) | |
| Winter | 5 (1.4%) | |
| Both | 128 (36%) | |
| I do not know | 48 (13.5%) | |
| Missing | 2 (0.6%) | |
| How often do you use sunscreen? | ||
| Always | 118 (33.1%) | |
| Sometimes | 109 (30.6%) | |
| Rarely | 74 (20.8%) | |
| Never used sunscreen | 53 (14.9%) | |
| Missing | 2 (0.6%) | |
| What practices do you apply to prevent vitamin D deficiency? (multiple responses) | ||
| Exposure to sunlight | 213 (35.1%) | |
| Take a vitamin D supplement | 188 (31%) | |
| Drink two cups of milk | 52 (8.6%) | |
| Not using SPF-containing creams | 18 (3%) | |
| Increase seafood in the diet | 73 (12%) | |
| None | 62 (10.2%) | |
| Willing to take vitamin D regularly if prescribed by physicians | ||
| Yes | 330 (92.7%) | |
| No | 24 (6.7%) | |
| Missing | 2 (0.6%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVitamin D Research Studies · Menstrual Health and Disorders · Climate Change and Health Impacts
Introduction
Vitamin D, popularly known as the sunshine vitamin, is an essential fat-soluble nutrient that plays a crucial role in overall good health. It is most well-known for assisting in promoting bone health by facilitating the absorption of phosphorus and calcium [1]. Vitamin D also contributes to immune system support, cell development regulation, and inflammation reduction [2]. An increased risk of many different ailments, including osteoporosis, diabetes, cardiovascular diseases, cancer, musculoskeletal disorders, and hypertension, has been associated with an insufficient amount of vitamin D [3].
Vitamin D is derived mostly from sun exposure, which is predominantly synthesized in the skin by activating 7-dehydrocholesterol with ultraviolet B (UVB) radiation and, to a lesser extent, through dairy products such as milk, codfish, mushrooms, eggs, and fortified food, as well as vitamin D supplementation [3]. Serum 25-hydroxyvitamin D (25(OH)D) is a valid biomarker of vitamin D status. The vitamin D range is based on numerous factors and differs across populations. Despite the constant controversy surrounding vitamin D deficiency, the most widely agreed upon definition for adults is a serum 25(OH)D level of less than 20 ng/mL, insufficiency between 20 and 30 ng/mL, and sufficiency above 30 ng/mL [4].
Recent studies suggest that there is growing concern about the worldwide prevalence of vitamin D insufficiency and deficiency [5]. It is estimated that nearly one billion people around the globe are affected by inadequate levels of this vital vitamin. In particular, populations in Europe, the Middle East, China, and Japan are at increased risk [6]. Vitamin D insufficiency is a concern for women in the Middle East [7,8]. Vitamin D insufficiency in women in the Middle East is primarily attributed to cultural practices, such as clothing habits that cover most of the body, which limit sun exposure necessary for vitamin D synthesis. Despite the region's abundant sunshine, many women spend considerable time indoors due to social and cultural factors, reducing their exposure to sunlight. Additionally, seasonal variation and air pollution can also contribute to lower vitamin D levels.
The prevalence of vitamin D deficiency ranges widely, ranging from 18% to 84%, and is influenced by factors such as the country of residence and local cultural practices [9]. Additional contributors to vitamin D deficiency include insufficient sun exposure, lifestyle choices, darker skin tones, warm climates, and prolonged breastfeeding without the supplementation of calcium and vitamin D [10]. Deficiencies in vitamin D are also prevalent in Lebanon, although the country has a Mediterranean climate, with ample sunlight throughout the year [11]. Thus, it is important to study the level of knowledge, attitudes, and practices (KAP) regarding vitamin D among populations. Given these concerns, it is essential to assess how well young Lebanese adults understand vitamin D's role, sources, and health implications. Investigating their knowledge, attitudes, and practices will provide valuable insights into potential gaps and inform strategies for improving awareness and prevention efforts. The primary aim of this study is to assess the knowledge, attitudes, and practices (KAP) regarding vitamin D among the Lebanese population with emphasis on young adults.
Materials and methods
Study design, sample size, and data collection
We used a quantitative cross-sectional design to investigate knowledge regarding vitamin D, along with attitudes and practices among the young adult population in Lebanon. The study was conducted between August 2023 and January 2024. Research data were collected through a self-administered online survey via Google Forms (Google, Inc., Mountain View, CA). The online questionnaire included an introduction that described the aim of the research and stated that participation was voluntary and anonymous and that the information collected via the survey would be used only for research purposes. Among the 370 responses, 16 were incomplete or invalid and were excluded, and 354 responses met the inclusion criteria.
Eligibility criteria included adult men or women aged 18-65 years residing in Lebanon. The data collection content was chosen and refined through a comprehensive analysis of previously published studies [12-14]. The questionnaire included four sections. The first part described the respondents' sociodemographic characteristics. The second section consisted of 12 queries related to vitamin D knowledge and an additional question about the source of that knowledge. The third part contained six questions exploring attitudes toward vitamin D, while the final part involved 18 practice-related questions concerning vitamin D. The questionnaire was provided in two languages, Arabic and English, to ensure accessibility.
Pilot study
We carried out a pilot study involving 16 participants to evaluate the survey before its full implementation. On the basis of these findings, adjustments were made to enhance clarity and comprehension. Data from the pilot study were excluded from the analysis presented hereafter. The survey's reliability was evaluated via a test-retest method, confirming its internal consistency. A value of 0.752 from Cronbach's alpha coefficient test demonstrated acceptable internal consistency.
Methodology for assessing knowledge and attitudes
For the knowledge assessment, scores were assigned on a scale of 0-40, with a mean cutoff of 21. The knowledge levels were categorized as poor for values below 20 and good for values equal to or exceeding 21. For the attitude evaluation, the participants who correctly answered four or more out of six questions were deemed to possess a positive attitude. Conversely, those with a score of 3 or less points were categorized as exhibiting a negative attitude.
Ethical approval
The Lebanese International University (LIU) Institutional Review Board approved the study under ethical authorization (approval number: LIUIRB-240208-SS-324). The participants in the research project were informed and provided agreement, with the understanding that their information would remain confidential.
Statistical analysis
The statistical analysis was conducted via the Statistical Package for Social Sciences (SPSS) version 26 (IBM SPSS Statistics, Armonk, NY) and Microsoft Office Excel 2016 (Microsoft Corp., Redmond, WA). The descriptive statistics present frequencies and percentages to show sociodemographic characteristics and responses regarding knowledge and attitudes toward vitamin D. The chi-square test was applied along with cross-tabulation analysis to assess correlations between sociodemographic characteristics and knowledge and attitudes toward vitamin D. A P value of ≤0.05 was used to indicate statistical significance.
Results
The survey included 354 participants; 241 (68.1%) were women, and 113 (31.9%) were men. Among the total female percentage, 41.8% (148) are veiled. The majority of the participants (64.4%, 228) were between the ages of 18 and 23, whereas 75 (21.2%) were between the ages of 24 and 29. In terms of educational status, a significant proportion of respondents, specifically 58.8% (187), were pursuing bachelor's degrees. In terms of marital status, the majority of the participants (298, 84.2%) were unmarried, 204 (48.5%) were students, and 124 (29.5%) and 39 (9.3%) were employed indoors and outdoors, respectively. The majority of the participants (60.2%, 213) stated that their skin tones varied from fair/light to beige. A total of 88 (23.2%) individuals reported having a light-brown/olive skin tone, whereas eight (2.3%) reported having dark-brown skin. Table 1 presents a detailed description of the participants' demographic characteristics.
Most participants had sufficient knowledge about sources of vitamin D, primarily from the internet and physicians (17.6%, 175). Sunlight was recognized as the most crucial source. Additionally, 244 (33.7%) of the participants acknowledged the role of vitamin D in preventing osteoporosis, whereas 148 (20.4%) believed that it was aiding in calcium absorption. Significant levels of knowledge and positive attitudes were evident among more than 266 (75%) of the participants. However, over half expressed concerns about their vitamin D levels. Most were willing to take supplements (92.7%, 330) and undergo testing (92.1%, 326).
A significant percentage of individuals (75.7%, 268) had adequate knowledge about vitamin D, while 86 (24.3%) had below-average levels (Figure 1).
Participants' overall knowledge scores
Our findings showed that education (chi-square=22.28; P value=0.001) and sex (chi-square=9.425; P value=0.002) had significant effects on vitamin D knowledge. Our results indicated that the internet and physicians accounted for 17.6% (175) of the primary knowledge sources, followed by colleges (14.9%, 148) and schools (12.2%, 121) (Figure 2).
Knowledge sources of vitamin D
Nearly all of those involved in the study knew that vitamin D is present in our body, and 198 (35.5%) of the participants were aware of its source. While 252 (71.2%) believed that meals alone could not provide sufficient vitamin D, the correct identification of dietary sources varied, with fatty fish being recognized by 181 (29.6%) and olive oil being recognized by only 43 (7.1%). Benefits, such as preventing osteoporosis (33.7%, 244) and assisting in calcium absorption (20.4%, 148) were reported. However, 142 (40.1%) of the respondents were aware of the correct range of vitamin D (20-50 ng/mL), whereas 167 (47.2%) were uncertain. With respect to the duration required for sun exposure to attain adequate vitamin D levels, 174 (49.2%) of the participants accurately reported the recommended duration of 10-20 minutes per day. Additionally, 211 (59.6%) were unaware of the recommended daily dosage of 600 IU. The causes of insufficiency were identified as inadequate meals (35.4%, 260) and insufficient sun exposure (38.6%, 283), with limited knowledge of additional factors. The awareness of the association of vitamin D with osteoporosis (32.4%, 281) and depression (18.7%, 162) varied, with only 31 (3.6%) of the respondents identifying cancer as a possible consequence of vitamin D deficiency. Table 2 shows the participants' knowledge of vitamin D.
Our study revealed that the majority of the participants (87.3%, 309) had a positive attitude toward vitamin D, whereas 12.7% (45) had a negative attitude (Figure 3). Statistics revealed a significant association between attitudes and gender (chi-square=10.877; P value=0.001).
Participants' overall attitude scores
In addition, 352 (99.4%) of the participants acknowledged the vital role of vitamin D in health. Although 292 (82.5%) expressed a preference for sun exposure, more than half (58.5%, 207) believed that it could harm the skin. There was clear concern about vitamin D levels, with 201 (56.8%) of the respondents expressing concern and 153 (43.2%) being unconcerned. Furthermore, a significant majority (89.5% and 92.1%, respectively) expressed interest in learning about symptoms associated with vitamin D deficiency and were willing to undergo testing if it was recommended by a medical professional. Details regarding the attitudes toward vitamin D are provided in Table 2.
Among the study participants, 207 (58.5%) reported having vitamin D serum levels tested, whereas 193 (54.5%) indicated that they were taking food supplements or multivitamins containing vitamin D. Of those individuals, 81 (22.9%) consumed 1000 IU or more of vitamin D, while 62 (17.5%) consumed less than 1000 IU. The majority (92.7%, 330) were willing to take vitamin D if recommended by physicians. When questioned about their preferences regarding sun exposure, 220 (62.1%) preferred exposure to the sun sometimes, whereas 28 (7.9%) avoided it altogether. Among those who indicated that they tended to spend time in the sun, 170 (47.8%) preferred morning hour exposure, followed by 70 (19.7%) in the afternoon. In terms of direct sun exposure frequency, 138 (38.7%) stated that they spent more than three times per week in direct sunlight. Moreover, 205 (57.6%) used sunscreen, primarily with an sun protection factor (SPF)>15, and the frequency of its application varied. The frequency of sunscreen application was reported to be 33.1% (118). With respect to practices to prevent vitamin D deficiency, sunlight exposure (35.1%, 213) and the use of vitamin D supplements (31%, 188) were included. Table 2 describes vitamin D-related practices.
In response to the question on the functions and benefits of vitamin D, the most recognized benefit among the participants was its role in preventing osteoporosis (33.7%, 244), followed by aiding in calcium absorption (20.4%, 148) and preventing general weakness (19.9%, 144). Fewer participants associated vitamin D with preventing chronic diseases (8%, 58) and cancer (5.9%, 43), while an equal number (5.9%, 43) linked it to vision health. Notably, 6.2% (45) of the respondents indicated that they were unaware of vitamin D's functions and benefits. These findings, summarized in Figure 4, highlight varying levels of awareness, with a stronger association between vitamin D and bone health compared to its broader physiological roles.
Functions and benefits of vitamin D
Discussion
Our cross-sectional study, which aimed to evaluate the levels of knowledge, attitudes, and practices regarding vitamin D deficiency among the young population in Lebanon, is one of the very few studies in a country marked with significant deficiency in vitamin D [11]. The study of the participants' vitamin D knowledge, attitudes, and practices provides information about essential variables affecting public health. Understanding these characteristics provides useful insights into alternative interventions aimed at addressing deficiencies and promoting optimal vitamin D status. The findings revealed a good level of knowledge about vitamin D among the public, which aligns with similar results reported in other studies [13,15,16] and contradicts those of other studies [17,18]. Variations in vitamin D knowledge can be associated with various factors, including public health education, healthcare infrastructure, culture, dietary practices, and access to information. Moreover, economic differences, literacy levels, and healthcare accessibility play major roles in shaping knowledge about vitamin D. Countries with well-established healthcare systems and comprehensive health promotion efforts tend to exhibit greater awareness of vitamin D than countries with less developed healthcare systems and limited health education initiatives. The internet emerged as the primary source of information, similar to the findings of a previous study [12,13]; additionally, physicians played a significant role in increasing health awareness among the Lebanese, which contrasts with findings from Kuwait [19]. In accordance with findings from other studies, the participants presented satisfactory knowledge regarding the three primary sources of vitamin D: sunlight, food, and supplements [20-22].
Even though the participants demonstrated good knowledge regarding the role of the sun in providing vitamin D, almost half of the respondents were able to specify the required duration of sun exposure accurately to acquire enough vitamin D (10-20 minutes) [16]. This differs from a study conducted in Oman [23]. Most respondents correctly identified fatty fish (salmon) as the main dietary source of vitamin D, in line with previous research [24]. However, similar to our results, 95 (15.5%) individuals incorrectly stated that vegetables and fruits are sources of vitamin D [24]. According to Matsui (2020), a daily vitamin D dosage of 600 IU is recommended [16]. Our analysis demonstrated that only 22.9% of the participants were aware of this recommended dose, which aligns with the results reported in another study in Jordan [13]. Furthermore, approximately half of the participants indicated awareness of normal serum vitamin D levels, with two-fifths providing the correct answer. This contrasts with findings from other research conducted in Saudi Arabia [25]. Research carried out by Uzrail et al. (2021) revealed that the respondents knew that insufficient sunlight and a lack of vitamin D-rich foods cause vitamin D deficiency [13]. Only a few thought it could be hereditary [13]. Our investigation provides comparable findings. In addition, most participants were familiar with the benefits of vitamin D (Figure 4) in maintaining bone health by preventing osteoporosis and assisting in calcium absorption. However, our results revealed a low level of awareness regarding other benefits of vitamin D, such as its role in preventing cancer. Matching results were observed in other studies carried out in Jordan and Oman [13,23].
This research investigated attitudes and practices of young Lebanese adults toward vitamin D. The results revealed that nearly all the participants presented positive attitudes toward vitamin D. These findings contrast with those of Al Bathi et al. (2012) [19] in Kuwait but align with those of Alkalash et al. (2023) [12], where all the participants agreed on the importance of vitamin D for health. Additionally, more than half of the participants were concerned about sunlight exposure, and most were interested in learning about vitamin D deficiency symptoms and being tested if needed [12]. In terms of practices, our results diverge from those reported in a study in Kuwait, indicating a different pattern of behaviors [19]. The majority of the participants reported spending only 15 minutes or between 15 and 29 minutes per day in the sun, particularly during the early morning, which is in accordance with the findings of research conducted in Jordan [13]. Most of the respondents in our study expressed a preference for sun exposure during the spring and summer seasons, suggesting that they obtain adequate vitamin D from sunlight. This aligns with the idea that exposure during these seasons promotes the synthesis of vitamin D through the skin, as suggested by Hoge et al. (2015) [26]. Furthermore, our findings show that practices such as sun exposure and the use of vitamin D supplements to prevent vitamin D deficiency are similar to those reported in other studies [13].
Two-fifths of the family respondents examined their vitamin D levels; however, one-third of them were vitamin D deficient [11,27]. In addition, 34.8% of the 148 female participants who wore scarves consumed food supplements or multivitamins containing vitamin D. This behavior may be due to cultural and religious practices, where women are expected to cover their hair and bodies, which might lead to vitamin D deficiency. In addition, over half of the participants utilized sunscreen as a protective measure against the sun. Limited exposure to sunlight and increased sunscreen usage, particularly among women, have been identified as key factors contributing to vitamin D deficiency, especially in women [28]. A considerable number of participants who use vitamin D supplements do so on the basis of recommendations from healthcare professionals or physicians; this demonstrates the importance of professional healthcare guidance in maintaining their health and overall well-being. In addition, 34.7% of the individuals who consumed food supplements or multivitamins containing vitamin D had fair-to-light beige skin tones. Importantly, individuals with darker skin tones are more prone to vitamin D deficiency. This is due to the presence of melanin, the pigment responsible for skin color, which limits the production of vitamin D3 in the skin. Therefore, individuals with darker skin need more sunlight exposure to generate sufficient vitamin D [29]. However, individuals with fair-to-light beige or pale skin tones may use more vitamin D tablets or multivitamins containing vitamin D since individuals with fair skin tones are more prone to sunburn and should therefore avoid prolonged sun exposure [30].
Limitations
The study of vitamin D knowledge, attitudes, and practices has limitations, including a sample that may not fully represent the population's diversity of knowledge and practices. Moreover, the predominance of female respondents in our study poses a potential limitation. Additionally, the use of an online survey introduces the possibility of self-selection bias, where health-conscious individuals may be overrepresented.
Conclusions
The study examines the knowledge, attitudes, and practices of the young Lebanese population regarding vitamin D. This study reveals that people are generally well-informed about its sources and benefits, despite some misconceptions. Most people are interested in learning about vitamin D deficiency symptoms and testing if necessary. However, there is potential for improvement in sun exposure practices and vitamin D supplementation adherence among specific demographic groups. The findings can be used to improve targeted interventions and public health campaigns in Lebanon.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Calcium and vitamin D: skeletal and extraskeletal health Curr Rheumatol Rep Khazai N Judd SE Tangpricha V 1101171020081846026510.1007/s 11926-008-0020-y PMC 2669834 · doi ↗ · pubmed ↗
- 2The sunlight-vitamin D connection: implications for patient outcomes in the surgical intensive care unit Cureus Nagaria TD Shinde RK Shukla S Acharya S Acharya N Jogdand SD 015202310.7759/cureus.46819 PMC 1063629037954702 · doi ↗ · pubmed ↗
- 3High prevalence of vitamin D deficiency among Iranian population: a systematic review and meta-analysis Iran J Med Sci Tabrizi R Moosazadeh M Akbari M 125139432018 https://pubmed.ncbi.nlm.nih.gov/29749981/29749981 PMC 5936844 · pubmed ↗
- 4Vitamin D deficiency N Engl J Med Holick MF 26628135720071763446210.1056/NEJ Mra 070553 · doi ↗ · pubmed ↗
- 5Global vitamin D status and determinants of hypovitaminosis D Osteoporos Int Mithal A Wahl DA Bonjour JP 180718202020091954376510.1007/s 00198-009-0954-6 · doi ↗ · pubmed ↗
- 6The urgent need to recommend an intake of vitamin D that is effective Am J Clin Nutr Vieth R Bischoff-Ferrari H Boucher BJ 6496508520071734448410.1093/ajcn/85.3.649 · doi ↗ · pubmed ↗
- 7Is vitamin D deficiency a major global public health problem?J Steroid Biochem Mol Biol Palacios C Gonzalez L 13814514420142423950510.1016/j.jsbmb.2013.11.003PMC 4018438 · doi ↗ · pubmed ↗
- 8Increasing trends and significance of hypovitaminosis D: a population-based study in the Kingdom of Saudi Arabia Arch Osteoporos Hussain AN Alkhenizan AH El Shaker M Raef H Gabr A 190920142521379810.1007/s 11657-014-0190-3 · doi ↗ · pubmed ↗