A Prospective Cross‐Sectional Cohort Study on Factors Associations With Right Heart Thrombi and Pulmonary Embolism
Wendlassida Martin Nacanabo, Taryètba André Arthur Seghda, Djième Claudine Dah, Mureille Loya, Lamoudi Prisca Thiombiano, Wendlassida Léa Françoise Sawadogo, Ella Hatoula Lengani, Anna Tall/Thiam, Nobila Valentin Yameogo, André Koudnoaga Samadoulougou, Partice Zabsonre

TL;DR
This study examines the management and outcomes of right heart thrombi in patients with pulmonary embolism over a 76-month period.
Contribution
The study provides new insights into the association between right heart thrombi and adverse outcomes in pulmonary embolism patients.
Findings
Right heart thrombi were associated with higher mortality and more frequent thrombolysis use.
Arterial hypotension and right ventricular dilatation were significantly linked to right heart thrombi.
The prevalence of right heart thrombi in pulmonary embolism was 2.98%.
Abstract
Floating thrombus of the right heart chambers is an uncommon diagnosis and is systematically associated with pulmonary embolism. The aim of this study is to describe the management and evolution of right intracavitary thrombi (TIC) in pulmonary embolism. This was a prospective cohort that ran for 76 months from March 5, 2017 to July 31, 2023. Patients diagnosed with pulmonary embolism were included. Two population groups were established according to the presence or absence of right intracavitary thrombus on Doppler echocardiography (intracavitary thrombi+ vs. intracavitary thrombi−) permitted to compare the risks factors. Thromboembolic risk factors, including the patient's background and clinical, paraclinical, therapeutic and evolutionary aspects, were reported. A significance level of p < 0.05 was used for data analysis. The prevalence of emboli associated with intracavitary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
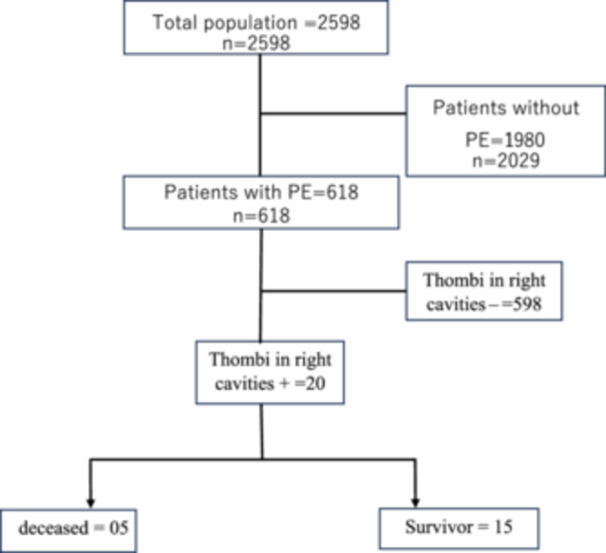 Figure 1
Figure 1| Variables | Total effectif ( | Thrombus+ ( | Thrombus− ( |
|---|---|---|---|
| Sociodemographic parameters | |||
| Average age | 54.46 | 53.11 | 54.56 |
| Men | 283 | 11 | 271 |
| Women | 335 | 09 | 326 |
| Thromboembolic risk factors | |||
| Obesity | 171 | 04 | 167 |
| Sedentary lifestyle | 422 | 14 | 408 |
| History of thromboembolic disease | 64 | 01 | 63 |
| Comorbidities | |||
| Diabetes | 45 | 00 | 45 |
| Hypertension | 161 | 05 | 156 |
| Cancer | 32 | 01 | 31 |
| Chronic respiratory disease | 38 | 03 | 35 |
| Clinical signs | |||
| Shortness of breath | 515 | 16 | 499 |
| Chest pain | 491 | 16 | 475 |
| Syncope/lipothymia | 80 | 05 | 75 |
| Haemoptysis | 65 | 04 | 61 |
| Arterial hypotension | 62 | 06 | 56 |
| Evolution | |||
| Hospital death | 62 | 05 | 57 |
| Paraclinical characteristics | Total number ( | TIC+ ( | TIC− ( |
|---|---|---|---|
| Electrocardiographic aspects | |||
| Aspect S1Q3T3 | 140 | 07 | 133 |
| Negative T waves from V1 to V3 | 102 | 02 | 100 |
| Right bundle branch block | 62 | 03 | 59 |
| Right atrial hypertrophy | 27 | 00 | 27 |
| Echocardiographic findings | |||
| Dilation of the right cavities | 164 | 12 | 152 |
| Right ventricular systolic dysfunction | 202 | 10 | 192 |
| TAPSE < 17 mmHg | 109 | 09 | 100 |
| CT scan | |||
| Proximal pulmonary embolism | 335 | 11 | 324 |
| Bilatérale pulmonary embolism | 346 | 08 | 338 |
| Pulmonary artery dilatation | 36 | 01 | 35 |
| Variables | TIC+ ( | TIC− ( | Odds ratio |
|
|---|---|---|---|---|
| Thromboembolic factors | ||||
| Sedentary lifestyle | 14 (3.32%) | 408 (96.68%) | 1.0866 | 0.5416 |
| Obesity | 04 (2.34%) | 167 (97.66%) | 0.6452 | 0.3097 |
| VTE history | 1 (1.56%) | 63 (98.44%) | 0.4470 | 0.3674 |
| Comorbidities | ||||
| Hypertension | 05 (3.11%) | 156 (96.89%) | 0.9444 | 0.5745 |
| Cancer | 02 (6.25%) | 30 (95.75%) | 2.1037 | 0.2774 |
| Respiratory disease | 03 (7.89%) | 35 (92.11%) | 2.8387 | 0.1183 |
| Clinical signs | ||||
| Shortness of breath | 16 (3.11%) | 499 (96.89%) | 0.7936 | 0.4341 |
| Chest pain | 16 (3.26%) | 475 (96.74%) | 1.0358 | 0.6059 |
| Syncope | 05 (6.25%) | 75 (93.757%) | 2.3244 | 0.0685 |
| Haemoptysis | 4 (6.15%) | 61 (93.85%) | 2.2008 | 0.1489 |
| Hypotension | 06 (9.68%) | 56 (90.32%) | 4.1482 | 0.0100 |
| Paraclinical signs | ||||
| S1Q3T3 Aspect | 7 (5.00%) | 133 (95.00%) | 1.8826 | 0.1442 |
| T wave V1 to V3 | 7 (07.44%) | 87 (92.55%) | 0.0358 | 0.4034 |
| CR dilatation | 12 (7.32%) | 152 (92.68%) | 4.4013 | 0.0013 |
| RV dysfunction | 10 (4.98%) | 191 (95.02%) | 2.1309 | 0.0759 |
| Proximal PE | 11 (3.18%) | 335 (96.82%) | 0.9595 | 0.5514 |
| Treatment | ||||
| Thrombolysis | 11 (13.58%) | 70 (86.42%) | 9.2190 | 0.0000 |
| Heparin | 20 (3.24%) | 598 (96.76) | 0.0000 | 0.0000 |
| Evolution | ||||
| Deceased | 05 (8.06%) | 57 (91.94%) | 3.1637 | 0.0409 |
| Variable | Univariate analysis | Multivariate analysis | |||
|---|---|---|---|---|---|
| OR |
| OR | [IC 95%] |
| |
| Hemoptysis | 2.2008 | 0.1489 | 2.2015 | [0.71; 6.69] | 0.1700 |
| Chronic respiratory disease | 2.8387 | 0.1183 | 0.0000 | [0.00; 1.00] | 0.9759 |
| Arterial hypotension | 4.1482 | 0.0100 | 4.1485 | [1.53; 11.2] | 0.0051 |
| Aspect S1Q3T3 | 1.8826 | 0.1442 | 1.8826 | [0.73; 4.81] | 0.1866 |
| Syncope | 2.3244 | 0.0685 | 2.3253 | [0.82; 6.58] | 0.1119 |
| Dilation of the right ventricle | 4.4013 | 0.0013 | 4.4013 | [1.76; 10.9] | 0.0015 |
| Thrombolysis | 9.2190 | 0.0000 | 9.2191 | [3.69; 23.3] | 0.0000 |
| Deaths | 3.1637 | 0.0000 | 3.1638 | [1.10; 9.02] | 0.0313 |
- —The authors received no specific funding for this work.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVenous Thromboembolism Diagnosis and Management · Cardiac tumors and thrombi · Atrial Fibrillation Management and Outcomes
Introduction
1
Floating thrombus of the right heart chambers is an uncommon diagnosis and is systematically associated with pulmonary embolism in 99% of cases [1]. It is a very poorly described entity with a prevalence of 4% in the literature [2, 3]. Several parameters have been identified as predictors of this pathology. The factors generally associated with its occurrence are congestive heart failure, right bundle branch block, and right ventricular systolic dysfunction [4]. It is a serious disease with a mortality rate of between 28% and 44% [4]. Despite this high mortality rate, its management remains less well codified, as there are no recommendations to date [4]. Emergency thrombolysis seems to be the most recommended treatment, but the route of administration is not unanimously accepted by authors, although there are regional consensuses [5]. We conducted a prospective cross‐sectional cohort study to investigate the factors associated with right intracavitary thrombi in pulmonary embolism at the Bogodogo University Hospital.
Patients and Methods
2
Study Population
2.1
This was a descriptive and analytical cross‐sectional study in the Cardiology Department of the Bogodogo University Hospital during the period from March 05, 2017 to July 31, 2023. Patients admitted to the cardiology department with pulmonary embolism confirmed by CT scan of the pulmonary arteries were included in our study. In cases of hemodynamic instability requiring emergency thrombolysis, the diagnosis of PE was re‐established by thoracic CT scan after the emergency had been resolved.
Study Variables
2.2
The presence of right intracavitary thrombus was the study variable of interest. Independent variables included:
- ▪Sociodemographic and clinical data including risk of hospital death.
- ▪Electrocardiographic parameters including the presence of S1Q3T3, negative T waves from V1 to V3, right bundle branch block, right atrial hypertrophy.
- ▪The Doppler echocardiographic parameters were: dilatation of the right cavities, presence of thrombus, and systolic function of the right ventricle assessed by Tricuspid Annular Plane Systolic Excursion (TAPSE).
- ▪The CT scan parameters were: location of thrombus, uni‐ or bilateral character, and dilatation of the pulmonary artery.
- ▪Evolutionary variables included mode of exit.
Ethical Considerations
2.3
Our study does not involve any risk for the participants. Participation in the study offers no financial remuneration and does not expose the patient to any additional risk other than that associated with his or her pathology. The study does not require the doctor to perform any additional act other than that which he or she undertakes for the patient concerned. The confidentiality of patients' personal information was respected during data processing. We have obtained the consent of the subjects concerned.
Statistical Analysis
2.4
All the data were entered on a microcomputer and analyzed using Epi‐Info software in its French version 7.2.5.0. The patients were subdivided into two groups according to whether echocardiography revealed a right intracavitary thrombus (Thrombus IC+) or not (Thrombus IC−). χ ^2^ and Fisher's exact tests were used in univariate analysis to determine the categorical variables associated with the occurrence of intracavitary thrombi. For quantitative variables, a Student's mean comparison test was used after verification of normality. In the absence of variable normality, the Kruskal–Wallis test was used to compare medians. The normality of the distribution of continuous variables was tested using graphical methods. A value of p < 0.05 defined the significance threshold for the association between the independent variables and the occurrence of pulmonary embolism. All variables with a univariate p < 0.2 were included in a multivariate logistic regression model to identify independent predictors of intracavitary thrombi.
Results
3
Clinical Characteristics of Patients
3.1
Among the 618 patients hospitalized for pulmonary embolism, 20 cases of right intracavitary thrombi were recorded, representing a prevalence of 3.22%. Figure 1 shows the flow of our patients. The mean age of our series was 54 ± 16.74 years, with a sex ratio of 0.86 for women. A sedentary lifestyle and obesity were the predominant thromboembolic risk factors. Table 1 shows the general characteristics of the patients according to the presence or absence of thrombus in the right cavities.
Patient flowchart.
Paraclinical Characteristics of Patients
3.2
The electrocardiogram showed an S1Q3T3 appearance in 05% (n = 07) of right intracavitary thrombi. The McGinn and White sign and the presence of a negative T wave from V1 to V3 were the most frequent electrical characteristics in our series. Transthoracic Doppler echocardiography revealed dilatation of the right cavities and right ventricular systolic dysfunction in 07.31% (n = 12) and 04.95% (n = 10) of these patients, respectively. Of the 20 cases of thrombi identified, 14 were in the right atrium, 5 in the right ventricle, and 1 in the pulmonary artery. PE was proximal in 11 patients and bilateral in 8 patients. Table 2 summarizes the paraclinical characteristics of patients.
Therapeutic and Evolutionary Characteristics of Patients
3.3
Heparin was used in all patients with right intracavitary thrombi. The presence of right intracavitary thrombi was statistically associated with thrombolysis. In total, 25% of patients with right intracavitary thrombi died. Table 3 gives the characteristics of the patients in univariate analysis. After multivariate logistic regression, arterial hypotension (OR = 4.14; IC = 1.53–11.2; p = 0.0051), right ventricular dilatation (OR = 4.40; IC = 1.76–10.9; p = 0.0051), thrombolysis (OR = 9.21; IC = 3.69–23.3; p = 0.00), and death (OR = 3.16; IC = 1.10–9.02; p = 0.03) were associated with the presence of intracavitary thrombi with a p < 0.05 (Table 4).
Discussion
4
Thrombi of the right heart can be classified into two main groups: the first group represents thombi of venous origin in transit from the right atrium or right ventricle. These are generally mobile, serpiginous thrombi [6]. Thrombi developed in situ or mural are small and immobile and make up the second group [4]. In the first group, thrombi most often originate in the veins of the lower limbs, inferior vena cava, renal veins, etc. The frequency of right heart thrombi in our series was 3.22%. Higher frequencies have been reported in the literature. The International Cooperative Pulmonary Embolism Registry (ICOPER) study found 4% [2]. Like other series, our results show a frequent association between hemodynamic instability and the presence of right heart thrombi in PE. The association of right ventricular dysfunction and arterial hypotension with right heart thrombi has been described in many series. It was 20% in the series by Koć et al. and that of Kurnicka et al. [7, 8].
The thromboembolic risk factors reported in our series were similar to those found in other scientific reviews. In agreement with previous studies, a sedentary lifestyle, obesity, and cancer were the most important thromboembolic risk factors associated with right heart thrombi [9]. Hypertension was the most frequent comorbidity in our series, but was not significantly associated with right heart thrombi. The difference between the physical characteristics of left and right heart thrombi is that right intracavity thrombi most often do not originate from the right atrium but rather from emboli of venous origin [10]. However, although exceptional, heart failure or atrial fibrillation may be responsible for right heart thrombi [10].
In our series, no thrombus attached to the heart wall was observed. That could be due to the size, location of thrombi in the heart chambers or the experience of the sonographer. Some authors also believe that the biological characteristics of thrombi may limit their detection by transthoracic echocardiography [11].
Emergency fibrinolysis was carried out in 13.58% of patients in our series, or 55% in the case of right intracavity thrombi, with a statistically significant difference. Failure to treat leads to mortality in 100% of cases [12]. However, there is still no consensus on the management of these thrombi, as there is as yet no consensus among practitioners. As a result, it is not clearly defined in the European recommendations on the management of pulmonary embolism [13]. Elsewhere, embolectomy has given satisfactory results [4, 14]. Some authors believe that thrombolytic agents cause thrombi to migrate into the pulmonary system, with dreadful consequences [15]. For this reason, surgical embolectomy is sometimes preferred to thrombolysis. In the case of early discovery of deep vein thrombosis in the lower limbs, the installation of a vena cava filter can prevent these thrombi from passing through the right cavities to cause PE [16].
The mortality rate was 25% among patients with right intracavitary thrombi in our series. This result is lower than that of Seghda and colleagues who found 45% mortality in 2015 [3]. Lower values have been reported in the literature. Indeed, Islam and colleagues, Ibrahim and colleagues, and Athappan and colleagues reported, respectively, 18.7%, 20.4%, and 23.2% mortality of right heart thrombi [16, 17, 18, 19]. The absence of emergency treatment other than fibrinolysis could explain this high mortality in our context.
Limitations of the Study
5
The limitations of this study are its single‐center design, the no 30‐day follow‐up, and the absence of investigations with an etiological aim. These limitations make it impossible to generalize these results, hence, the need for further multicenter studies.
Conclusion
6
The presence of a floating thrombus in the right chambers is an uncommon entity but is associated with a high mortality rate. Arterial hypotension, right ventricular dilatation, thrombolysis, and death were the factors associated with right heart thrombi in this study. Although their mortality is high, there is no consensus or recommendation on their management. Surgical embolectomy or emergency fibrinolysis appear to be the best way of improving their prognosis. An evaluation of the impact of thrombolysis on right intracavitary thrombi is crucial in our context where other means are unavailable.
Author Contributions
Wendlassida Martin Nacanabo: writing – original draft, writing – review and editing, investigation, methodology. Taryètba André Arthur Seghda: conceptualization, methodology, data curation, writing – original draft, writing – review and editing, investigation, project administration. Djième Claudine Dah: methodology, data curation. Mureille Loya: data curation. Lamoudi Prisca Thiombiano: data curation. Wendlassida Léa Françoise Sawadogo: data curation. Ella Hatoula Lengani: data curation. Anna Tall/Thiam: supervision. Nobila Valentin Yameogo: supervision. André Koudnoaga Samadoulougou: supervision. Partice Zabsonre: supervision.
Ethics Statement
Approval was obtained from the Ethics Committee of Bogodogo University Hospital (N2024‐03‐038). The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Conflicts of Interest
The authors declare no conflicts of interest.
Transparency Statement
The lead author Wendlassida Martin Nacanabo affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1O. Brault‐Meslin , S. Mazouz , O. Nallet , S. Cattan , and W. Amara , “Floating Thrombus in Right Cavities,” Annales de Cardiologie et d'Angéiologie 64, no. 5 (2015): 410–413.10.1016/j.ancard.2015.09.04326482630 · doi ↗ · pubmed ↗
- 2S. Z. Goldhaber , L. Visani , and M. De Rosa , “Acute Pulmonary Embolism: Clinical Outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER),” Lancet 353, no. 9162 (1999): 1386–1389.10227218 10.1016/s 0140-6736(98)07534-5 · doi ↗ · pubmed ↗
- 3T. A. Seghda , N. V. Yaméogo , G. R. C. Millogo , et al., “Prise en charge et pronostic des embolies pulmonaires associées à des thrombi intracavitaires droits: à propos d'une série prospective au centre Hospitalier Universitaire Yalgado Ouédraogo,” Annales de Cardiologie et d'Angéiologie 68, no. 2 (2019): 65–70.10.1016/j.ancard.2018.09.00430292445 · doi ↗ · pubmed ↗
- 4A. Torbicki , N. Galié , A. Covezzoli , E. Rossi , M. De Rosa , and S. Z. Goldhaber , “Right Heart Thrombi in Pulmonary Embolism,” Journal of the American College of Cardiology 41, no. 12 (2003): 2245–2251.12821255 10.1016/s 0735-1097(03)00479-0 · doi ↗ · pubmed ↗
- 5Z. Sammuel , M. D. Goldhaber , et al., “Optimal Strategy for Diagnosis and Treatment of Pulmonary Embolism Due to Right Atrial Thrombus,” Science Direct 63, no. 12 (1988): 1261–1264.10.1016/s 0025-6196(12)65416-03199890 · doi ↗ · pubmed ↗
- 6B. Mohan , S. T. Chhabra , A. Gulati , et al., “Clinical and Echocardiographic Diagnosis, Follow Up and Management of Right‐Sided Cardiac Thrombi,” Indian Heart Journal 65, no. 5 (2013): 529–535.24206876 10.1016/j.ihj.2013.08.015PMC 3860838 · doi ↗ · pubmed ↗
- 7M. Koć , M. Kostrubiec , W. Elikowski , et al., “Outcome of Patients With Right Heart Thrombi: The Right Heart Thrombi European Registry,” European Respiratory Journal 47, no. 3 (2016): 869–875.26797032 10.1183/13993003.00819-2015 · doi ↗ · pubmed ↗
- 8K. Kurnicka , B. Lichodziejewska , S. Goliszek , et al., “Echocardiographic Pattern of Acute Pulmonary Embolism: Analysis of 511 Consecutive Patients,” Journal of the American Society of Echocardiography 29, no. 9 (2016): 907–913.27427291 10.1016/j.echo.2016.05.016 · doi ↗ · pubmed ↗