Intrapleural administration with traditional Chinese medicine injections (Sophorae flavescentis preparations) in controlling malignant pleural effusion: a clustered systematic review and meta-analysis
Yan Zhang, Zheng Xiao, Hui Liu, Da-Chun Cai, Yao-Qin Luo, Jiao Xu, Feng Luo, Jun Huang, Yan-Yan Jin, Teng-Yang Fan, Jun Zhang, Xue Xiao, Ji-Hong Feng

TL;DR
This study reviews the effectiveness of traditional Chinese medicine injections in treating malignant pleural effusion, finding that some combinations may be as effective as standard treatments.
Contribution
The paper introduces a clustered systematic review and meta-analysis of Sophorae flavescentis injections for malignant pleural effusion.
Findings
Perfusion with CKI alone showed similar outcomes to cisplatin alone in treating MPE.
CKI combined with cisplatin significantly improved response rates and reduced side effects.
Kang’ai and matrine with cisplatin also improved response rates with moderate evidence.
Abstract
Sophorae flavescentis (kushen) preparations are widely used to control malignant pleural effusion (MPE) through intrapleural perfusion. This analysis aims to verify the therapeutic values of perfusion with kushen preparations for controlling MPE, reveal the optimal treatment plan, suitable population, and usage, and to demonstrate their clinical effectiveness and safety. We performed and reported this systematic review/meta-analysis (PROSPERO: CRD42023430139) following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. All randomized controlled trials (RCTs) concerning perfusion with kushen preparation for MPE were collected from Chinese and English databases. We clustered all eligible studies into multiple homogeneous treatment units, assessed their methodological quality using a RoB 2, pooled the data from each unit, and summarized the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
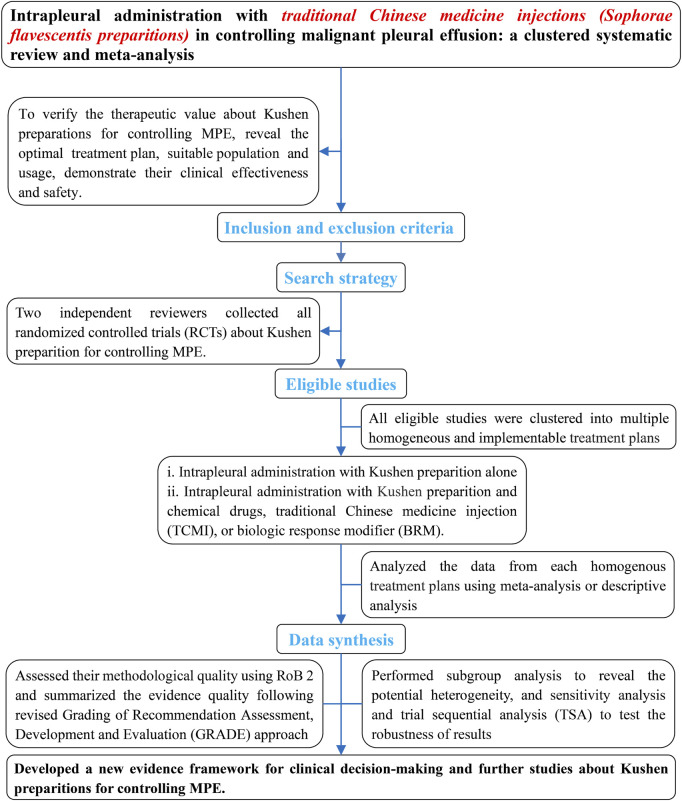 FIGURE 1
FIGURE 1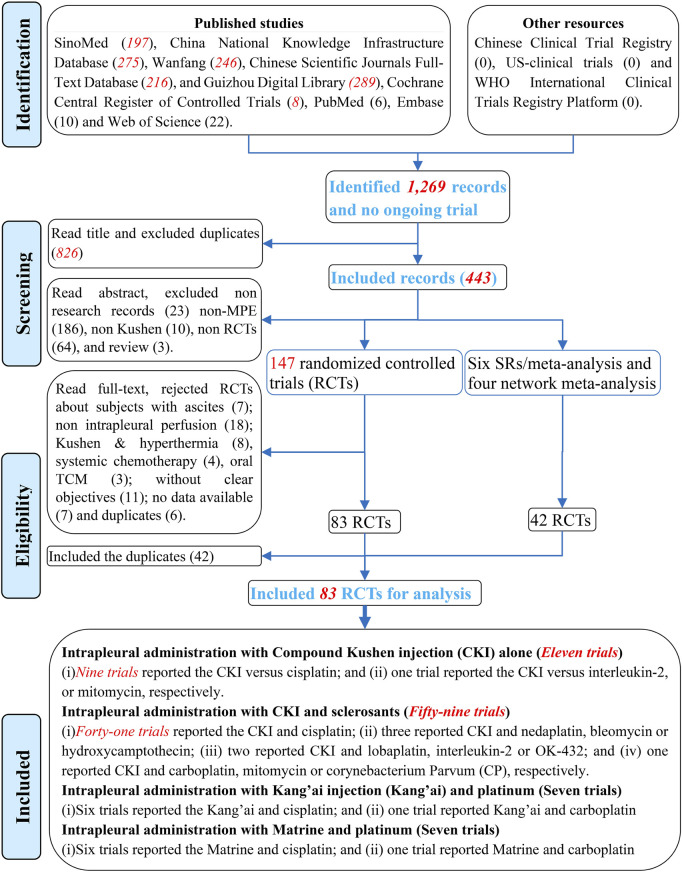 FIGURE 2
FIGURE 2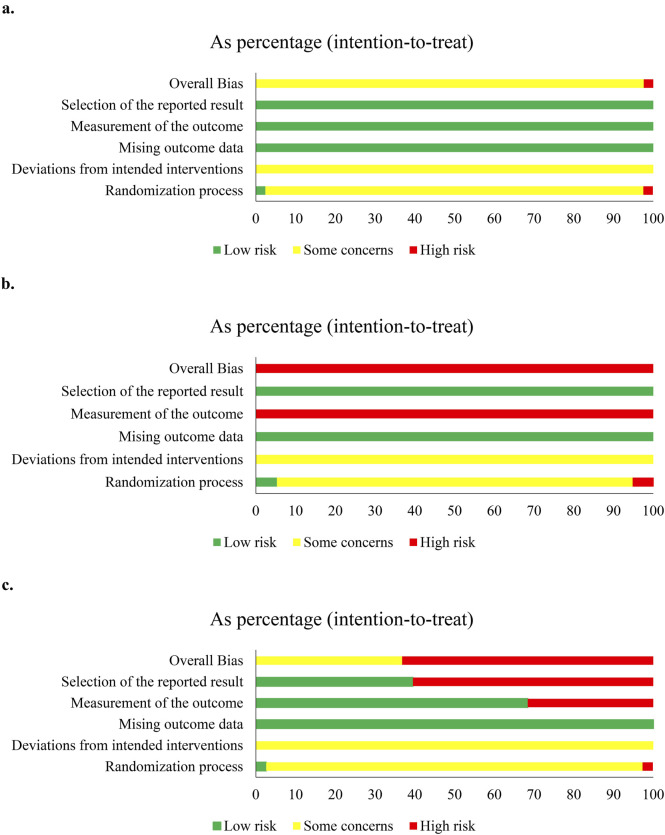 FIGURE 3
FIGURE 3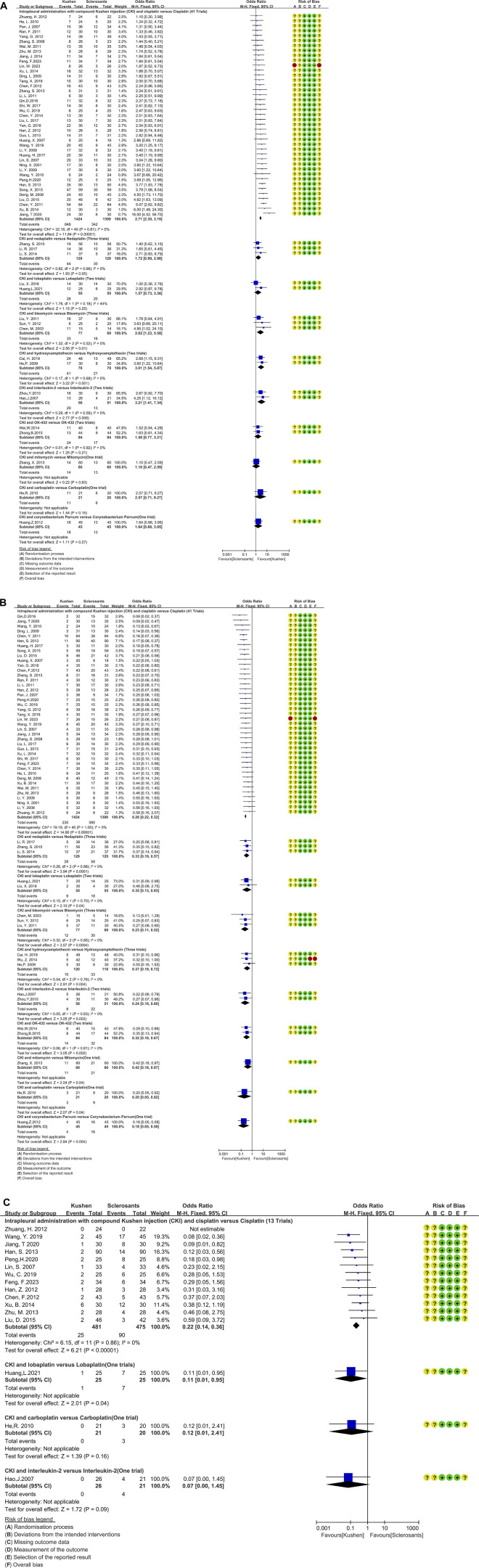 FIGURE 4
FIGURE 4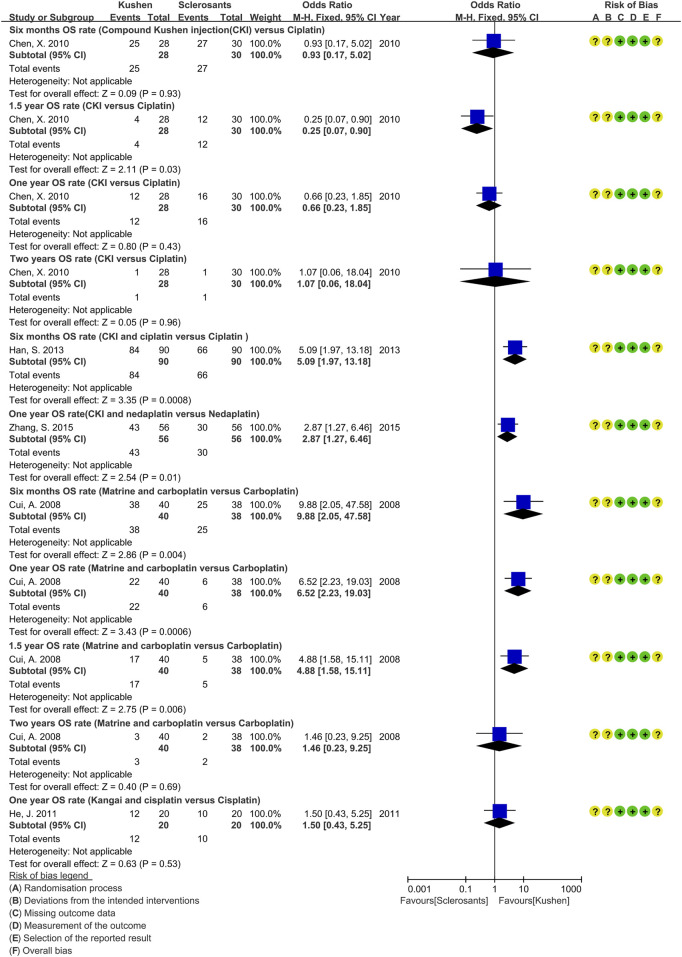 FIGURE 5
FIGURE 5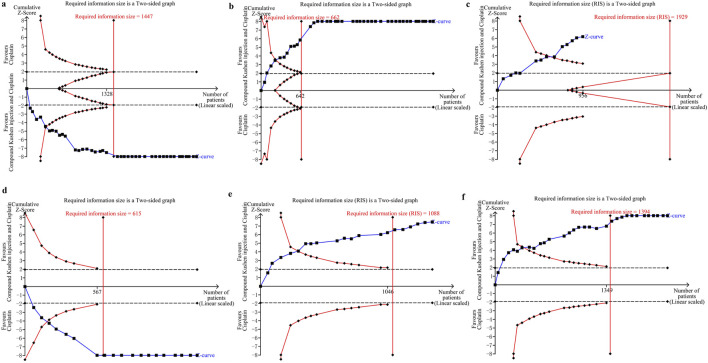 FIGURE 6
FIGURE 6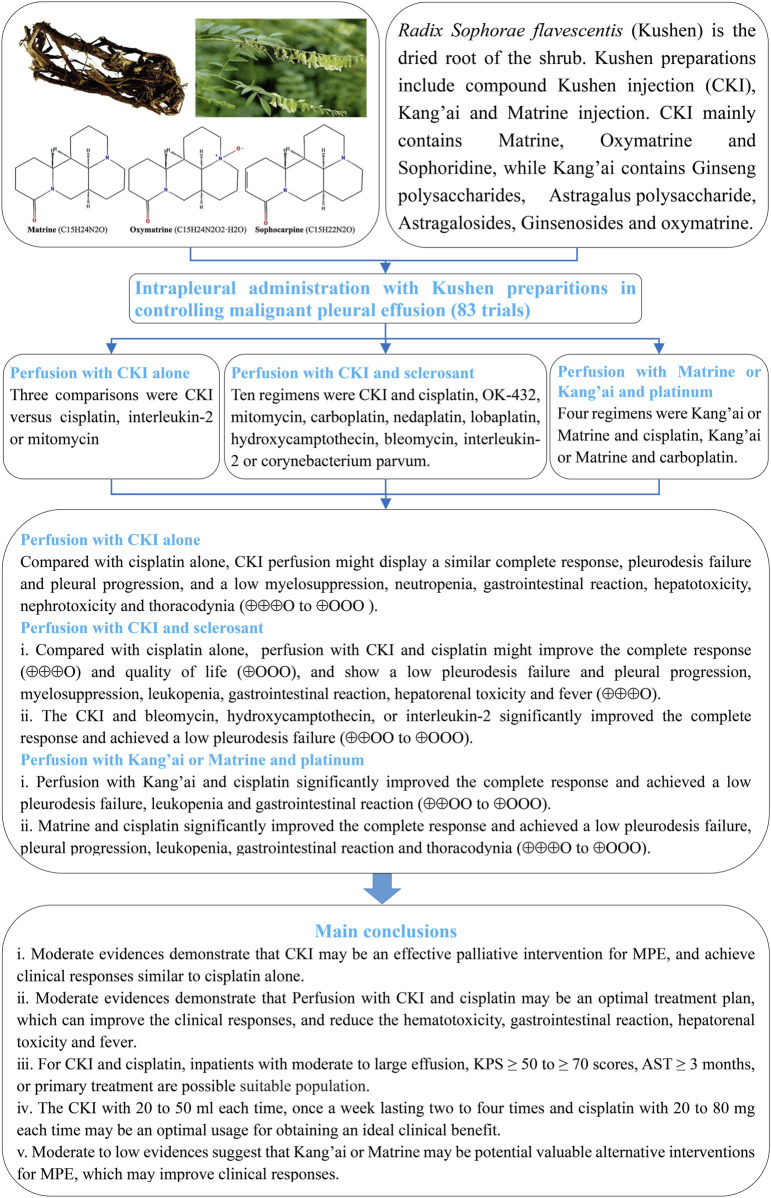 FIGURE 7
FIGURE 7| First author, year | Malignant pleural effusions | Interventions | Evaluation times | Criteria | Outcomes | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tumor | Volume | KPS | TH | AST | E/C | M/F | Years | DM |
| Sclerosants | ||||
| a | ||||||||||||||
| CKI versus cisplatin (nine trials) | ||||||||||||||
|
| MTs | Un | ≥40 | PT | Un | 26/26 | 32/20 | 36–87 | IPC | 20 mL, 2–3 times/w, 4–6 times | 40 mg/m2 | 6–7 weeks | Millar, Un | O1-3 |
|
| LC | Small to large | ≥50 | Un | >3 | 20/20 | 25/15 | 62–67 | IPC | 20 mL, 2 times/w, 4 times | 30 mg | 9 weeks | Millar, Un | O1-3 |
|
| MTs | Large | Un | Un | Un | 28/30 | 31/27 | 59–77 | IPC | 20 mL, 1 time/w, 3 times | 30 mg/m2 | 2 years | Millar, WHO | O1,3,4 |
|
| MTs | Un | >50 | Un | Un | 56/54 | Un | 35–83 | IPC | 20 mL, 1 time/w, 3–4 times | 40 mg/m2 | 7–8 weeks | Ostrowskimj, WHO | O1-3 |
|
| MTs | Moderate to large | ≥70 | Un | Un | 40/40 | 46/34 | 20–82 | IPC | 40 mL, 1 time/w, 4 times | 40 mg/m2 | 8 weeks | Millar, Un | O1-3 |
|
| LC | Moderate to large | >50 | Un | ≥3 | 45/42 | 52/35 | 43–79 | IPC | 20 mL, 1–2 time/w, 4 times | 40–60 mg | 8 weeks | Millar, Un | O1-3 |
|
| MTs | Un | >60 | Un | >3 | 20/30 | Un | 45–81 | IPC | 20 mL, 1 time/w, 4 times | 40 mg | 8 weeks | Ostrowskimj, Un | O1-3 |
|
| MTs | Un | Un | PT | Un | 30/30 | 51/39 | 36–81 | IPC | 40 mL, 2 times/w, 7 times | 40 mg | 8 weeks | Ostrowskimj, WHO | O1,3 |
|
| BC | Small to large | Un | Un | >3 | 16/15 | 0/31 | 57–75 | IPC | 50 mL, 2 times/48 h,i2 times | 40 mg | 6 weeks | Millar, Un | O1,3 |
| CKI versus Interleukin-2 (one trial) | ||||||||||||||
|
| HCC | Un | Un | Un | Un | 65/63 | 117/11 | 45.3 ± 3.2/44.8 ± 2.9 | Un | 20 mL, 1 time/day, 5 times | 1 MU | 7 weeks | Ostrowskimj, Un | O1 |
| CKI versus mitomycin (one trial) | ||||||||||||||
|
| MTs | Un | >60 | Un | >3 | 50/50 | 68/32 | 38–76 | IPC | 40 mL, 1 time/w, 3 times | 10 mg | 7 weeks | Ostrowskimj, Un | O1-3 |
| b. Intrapleural administration with CKI and sclerosants | ||||||||||||||
| CKI and cisplatin versus cisplatin (41Trials) | ||||||||||||||
|
| LC | Large | Un | Un | >1 | 20/18 | 28/10 | 35–70 | Thora* | 20 mL, 1 time/w, 1-2 times | 40 mg | 5–6 weeks | Ostrowskimj, Un | O1,3 |
|
| MTs | Moderate to large | Un | Un | Un | 33/33 | 40/26 | 36–75 | Thora* | 20 mL, 1 time/w, Un | 60 mg | Un | Millar, Un | O1,3 |
|
| MTs | Un | ≥60 | Un | Un | 36/34 | 43/27 | 60 ± 21 | IPC | 30 mL, 1 time/w, 2–4 times | 40 mg | 6–8 weeks | Ostrowskimj, WHO | O1-3 |
|
| MTs | Un | >60 | PT | Un | 28/23 | 27/24 | 31–80 | IPC | 20 mL, 1 time/w, 4 times | 20 mg | 8 weeks | Ostrowskimj, Un | O1 |
|
| MTs | Un | ≥60 | Un | ≥3 | 31/30 | 41/20 | 38–76 | IPC | 20 mL, 1 time/w, 3 times | 30 mg | 7 weeks | Ostrowskimj, WHO | O1-3 |
|
| LC | Un | Un | Un | >1 | 30/30 | 49/11 | 35–70 | Thora* | 20 mL, 1 time/w, Un | 40 mg | 8 weeks | Ostrowskimj, Un | O1,3 |
|
| LC | Moderate to large | ≥50 | RT | >3 | 24/20 | 25/19 | 39–75 | IPC | 40 mL, 1 time/w, 3 times | 40 mg | 7 weeks | Ostrowskimj, WHO | O1,3 |
|
| MTs | Un | >60 | Un | >3 | 24/24 | Un | 55–82 | IPC | 20 mL, 2 times/w, 8 times | 40 mg | 8 weeks | Ostrowskimj, Un | O1,3 |
|
| MTs | Un | ≥60 | Un | Un | 84/84 | Un | 38–85 | IPC | 60 mL, 1 time/w,3-5 times | 40–60 mg | 3 years | Ostrowskimj, Un | O1,3,4 |
|
| MTs | Un | Un | Un | Un | 35/35 | 40/30 | 21–75 | IPC | 20 mL, 1 time/w, 4 times | 40 mg | 8 weeks | Ostrowskimj, Un | O1 |
|
| MTs | Moderate to large | ≥60 | Un | Un | 43/43 | 60/26 | 35–68 | IPC | 30 mL, 1 time/w, 4 times | 60 mg/m2 | 8 weeks | Millar, WHO | O1,3 |
|
| LC | Un | >50 | PT | >3 | 28/28 | 35/21 | 41–91 | IPC | 12–20 mL, 1time/w, 2-4 times | 20–40 mg | 8 weeks | Millar, WHO | O1-3 |
|
| MTs | Moderate to large | ≥60 | Un | ≥3 | 39/39 | 43/35 | 33–76 | IPC | 25 mL, 1 time/w, 4 times | 40–60 mg | 8 weeks | Ostrowskimj, CTEC3.0 | O1-3 |
|
| HM | Un | Un | Un | Un | 24/22 | 23/23 | 15–81 | Thora* | 10 mL, 1 time/w, 3–6 times | 20 mg/m2 | 7–10 weeks | Millar, WHO | O1,3 |
|
| MTs | Moderate to large | ≥50 | PT | Un | 31/31 | Un | 18–72 | IPC | 20 mL, 1 time/w, 4 times | 40 mg | 7–10 weeks | Ostrowskimj, WHO | O1-3 |
|
| MTs | Un | >60 | Un | >3 | 90/90 | 93/87 | 34–82 | IPC | 40 mL, 1 time/w, 3 times | 20 mg/m2 | 7 weeks | Millar, WHO | O1-4 |
|
| MTs | Un | >50 | Un | >3 | 31/31 | Un | 51–78 | IPC | 30 mL, 1–2 times/w, Un | 30 mg/m2 | Un | Ostrowskimj, WHO | O1,3 |
|
| MTs | Moderate to large | ≥70 | Un | Un | 28/28 | 30/26 | 35–82 | IPC | 20 mL, 1 time/w, 4–6 times | 60 mg | 8–10 weeks | Millar, Un | O1,3 |
|
| MTs | Moderate to large | Un | PT | Un | 30/30 | 38/22 | 60–83 | IPC | 20 mL, 1 time/w, 4 times | 40 mg | 8 weeks | Ostrowskimj, Un | O1-3 |
|
| MTs | Un | Un | Un | Un | 34/34 | 37/31 | 34–81 | IPC | 20 mL, 1 time/w, 6 times | 60 mg | 10 weeks | Ostrowskimj, Un | O1-3 |
|
| MTs | Un | ≥60 | Un | Un | 30/30 | 36/24 | 32–79 | Thora* | 60 mL, 1 time/w, 2–4 times | 80 mg | 6–8 weeks | Millar, Un | O1,3 |
|
| MTs | Un | Un | Un | Un | 32/32 | 34/30 | 39–82 | Thora* | 40 mL, 1 time/w, 6 times | 40 mg | 10 weeks | Ostrowskimj, Un | O1-2 |
|
| LC | Un | >60 | PT | >3 | 46/42 | 48/40 | 60.2 ± 8.2 | IPC | 20 mL, 1 time/w, 3 times | 40–60 mg | 8 weeks | Millar, Un | O1-3 |
|
| MTs | Un | ≥70 | Un | Un | 59/59 | 64/54 | 42–73 | IPC | 25 mL, 1 time/w, 4 times | 50 mg | 8 weeks | Ostrowskimj, Un | O1,3 |
|
| MTs | Un | >60 | Un | >3 | 35/30 | Un | 45–81 | IPC | 20 mL, 1time/w, 4 times | 40 mg | 8 weeks | Ostrowskimj, Un | O1-3 |
|
| MTs | Un | Un | Un | Un | 32/32 | Un | 38–76 | IPC | 20 mL, 1time/w, Un | 60 mg | Un | Ostrowskimj, Un | O1,3 |
|
| MTs | Un | >60 | Un | >3 | 30/30 | 43/17 | 62.8 ± 7.7; 3.3 ± 8.1 | IPC | 20 mL, 1 time/w, 4 times | 40 mg | 8 weeks | Ostrowskimj, Un | O1,3 |
|
| LC | Moderate to large | ≥50 | PT | Un | 30/30 | Un | 32–76 | IPC | 20 mL, 1 time/w, 4 times | 40 mg | 8 weeks | Ostrowskimj, WHO | O1-3 |
|
| LC | Large | ≥50 | PT | Un | 30/30 | 39/21 | 34–78 | IPC | 20 mL, 1 time/w, 4 times | 40 mg | 8 weeks | Ostrowskimj, WHO | O1-3 |
|
| LC | Large | ≥50 | PT | Un | 30/30 | Un | 33–77 | IPC | 60 mL, 2 times/w, 6 times | 40 mg | 7 weeks | Ostrowskimj, WHO | O1-3 |
|
| LC | Un | Un | Un | Un | 25/25 | 30/20 | 39–68 | IPC | 40–60 mL, 1–2 times/w, 3–6 times | 40–60 mg | 8–9 weeks | Millar, WHO | O1-3 |
|
| LC | Un | Un | Un | Un | 45/45 | 49/41 | 58–75 | IPC | 20 mL, 1 time/w, 3 times | 40–60 mg | 7 weeks | Millar, Un | O1-3 |
|
| LC | Un | Un | Un | Un | 25/25 | 29/22 | 41–70 | IPC | 40 mL, 3 times/w, 12 times | 30 mg | 8 weeks | Millar, Un | O1,3 |
|
| LC | Moderate | >60 | RT | >3 | 34/34 | 39/29 | 43–79 | IPC | 30 mL, 1 times/w, 3 times | 40 mg | 7 weeks | Millar, WHO | O1-3 |
|
| MTs | Un | Un | Un | Un | 30/30 | 46/14 | 25–65 | Thora* | 20 mL, 1 time/w, 4 times (40 mg) | 60 mg | 8 weeks | Ostrowskimj, WHO | O1,3 |
|
| MTs | Un | Un | Un | Un | 40/40 | 46/34 | 29–69 | Thora* | 20 mL, 1 time/w, Un (30 mg) | 60 mg | Un | Ostrowskimj, WHO | O1,3 |
|
| MTs | Un | Un | Un | Un | 32/32 | 51/13 | 29–73 | IPC | 20 mL, 1 time/w, 4 times (40 mg) | 60 mg | 8 weeks | Ostrowskimj, WHO | O1,3 |
|
| MTs | Moderate to large | Un | Un | Un | 30/30 | 34/26 | 40–80 | IPC | 20 mL, 1 time/w, 2–3 times (40 mg) | 60 mg | 6–7 weeks | Ostrowskimj, Un | O1,3 |
|
| MTs | Un | >60 | Un | >3 | 30/30 | 33/27 | 35–79 | IPC | 25 mL, 1 time/w, 2–4 times (40 mg) | 60 mg | 6–8 weeks | Ostrowskimj, WHO | O1-3 |
|
| MTs | Un | Un | Un | Un | 30/30 | 44/16 | 43–71 | IPC | 20mL, un (20 mg) | 40 mg | Un | Millar, Un | Q1,3 |
|
| MTs | Small to large | ≥60 | PT | >3 | 26/26 | 29/23 | 34–76 | IPC | 30 mL, 1time/w, 3 times | 40 mg | 7 weeks | Ostrowskimj, WHO | O1-3 |
| CKI and nedaplatin versus Nedaplatin (Three trials) | ||||||||||||||
|
| MTs | Moderate to large | ≥50 | PT | >3 | 37/37 | Un | 36–78 | IPC | 25 mL, 2 times/w, 4 times | 40–60 mg | 6 weeks | Ostrowskimj, WHO | O1-3 |
|
| LC | Un | >60 | Un | >3 | 56/56 | 68/44 | 35–78 | IPC | 30 mL, 1 time/w, 4 times | 60 mg | 8 weeks | Ostrowskimj, Un | O1-4 |
|
| MTs | Un | >60 | Un | >3 | 36/36 | 38/34 | 40–79 | IPC | 30 mL, 1 time/w, 4 times | 60 mg | 8 weeks | Ostrowskimj, Un | O1-3 |
| CKI and carboplatin versus carboplatin (One trial) | ||||||||||||||
|
| MTs | Moderate to large | Un | Un | >3 | 21/20 | 22/19 | Un | IPC | 40 mL, 1 time/w, 4 times | 400 mg | 8 weeks | Millar, WHO | O1,3 |
| CKI and lobaplatin versus lobaplatin (two trials) | ||||||||||||||
|
| LC | Moderate to large | Un | Un | Un | 30/30 | 62/28 | 32–76 | Thora* | 30 mL, 1 time/w, 4 times | 30 mg | 8 weeks | Ostrowskimj, Un | O1,3 |
|
| LC | Un | Un | Un | Un | 25/25 | 27/23 | 44–81 | IPC | 30 mL, 1 time/w, Un | 30 mg | Un | Millar, Un | O1 |
| CKI and bleomycin versus bleomycin (three trials) | ||||||||||||||
|
| MTs | Large | Un | Un | Un | 15/14 | 18/11 | 40–75 | IPC | 20 mL, 1 time/w, 2 times (40 mg) | 60 mg | 8 weeks | Ostrowskimj, WHO | O1,3 |
|
| MTs | Un | >60 | Un | >3 | 37/30 | 37/30 | 45–76 | IPC | 20 mL, 1 time/w, 4 times | 40 mg | 8 weeks | Ostrowskimj, WHO | O1-3 |
|
| MTs | Un | ≥40 | Un | >3 | 25/25 | 31/19 | 42–81 | IPC | 20 mL, 1 time/w, 4 times | 45 mg | 8 weeks | Ostrowskimj, Un | O1-3 |
| CKI and hydroxycamptothecin versus hydroxycamptothecin (Three trials) | ||||||||||||||
|
| MTs | Un | Un | Un | Un | 30/30 | 45/15 | 27–64 | Thora* | 30 mL, 1 time/w, 4 times | 10 mg | 8 weeks | Ostrowskimj, WHO | O1,3 |
|
| LC | Un | Un | Un | Un | 42/40 | 50/32 | 60–82 | Thora* | 30 mL, 1 time/w, 4 times | 5 mg | 8 weeks | Millar, Un | O1,3 |
|
| LC | Large | Un | Un | ≥3 | 48/48 | 59/37 | 65.3 ± 7.1; 66.0 ± 7.2 | IPC | 30 mL, 1 time/w, 4 times | 5 mg | 8 weeks | Ostrowskimj, Un | O1,3 |
| CKI and interleukin-2 versus interleukin-2 (two trials) | ||||||||||||||
|
| MTs | Un | Un | Un | Un | 26/21 | 33/14 | 45–83 | IPC | 20 mL, 1 time/w, 3 times | 2MU | 7 weeks | Millar, WHO | O1,3 |
|
| LC | Small to large | >40 | PT | >3 | 30/30 | 42/18 | 60–85 | IPC | 30 mL, 1 time/w, 4 times | 2MU | 8 weeks | Ostrowskimj, WHO | O1,3 |
| CKI and OK-432 versus OK-432 (two trials) | ||||||||||||||
|
| MTs | Un | Un | Un | Un | 40/40 | 45/35 | Un | IPC | 20 mL, 3 time/w, 3 times | d1:5 KE, d4,d7:10 KE | Un | Ostrowskimj, Un | O1,3 |
|
| MTs | Un | >40 | Un | Un | 44/44 | 49/39 | Un | IPC | 20 mL, 3 time/w, 3 times | d1:5 KE, d4,d7:10 KE | 5 weeks | Ostrowskimj, Un | O1,3 |
| CKI and mitomycin versus mitomycin (one trial) | ||||||||||||||
|
| MTs | Moderate to large | >40 | Un | >3 | 60/60 | 67/53 | 49–76 | IPC | 40 mL, 1 time/w, 3 times | 10 mg | 7 weeks | Ostrowskimj, Un | O1-3 |
| CKI and | ||||||||||||||
|
| LC | moderate to large | >50 | PT | >3 | 45/45 | 47/43 | 40–77 | IPC | 30 mL, 1 time/w, 4 times | 4 mL (24*109) | 8 weeks | Millar, WHO | O1-3 |
| c. Intrapleural administration with | ||||||||||||||
|
| ||||||||||||||
|
| MTs | Un | ≥60 | Un | Un | 20/21 | 19/22 | 36–72 | IPC | 60 mL, 1 time/w, 1–3 times | 80 mg | 7 weeks | Ostrowskimj, WHO | O1,3 |
|
| LC | Large | >50 | Un | >1 | 36/35 | 43/28 | 45–80 | IPC | 60 mL, 1 time/w, 2–4 times | 40 mg/m2 | 6–8 weeks | Ostrowskimj, WHO | O1,3 |
|
| MTs | Un | ≥50 | Un | >3 | 33/33 | 44/22 | 56 ± 4.7 | IPC | 40 mL, 2 times/w, 4 times | 60 mg | 6 weeks | Ostrowskimj, Un | O1-3 |
|
| MTs | Un | ≥70 | Un | Un | 20/20 | 24/16 | 45–72 | Un | 60 mL, 1 time/w, 1–3 times | 80 mg | 6–10 weeks | Millar, WHO | O1,3,4 |
|
| LC | Moderate to large | >60 | PT | >3 | 24/22 | 27/19 | 46–84 | IPC | 50 mL,1 time/w, 3 times | 40–60 mg | 8 weeks | Ostrowskimj, Un | O1-3 |
|
| LC | Large | Un | Un | >1 | 35/35 | 44/26 | 64.5 ± 8.7 | IPC | 60 mL, 1 time/w, Un | 40 mg/m2 | Un | Ostrowskimj, Un | O1 |
|
| ||||||||||||||
|
| MTs | Un | ≥50 | Un | Un | 25/23 | 26/22 | 53–82 | IPC | 60 mL, 1 time/week, 2–4 times | 300 mg | 6–8 weeks | Ostrowskimj, WHO | O1,3 |
| d. Intrapleural administration with matrine injection (matrine) | ||||||||||||||
| Matrine and cisplatin versus cisplatin (six trials) | ||||||||||||||
|
| MTs | Un | Un | Un | Un | 40/36 | 39/37 | 39–78 | IPC | 200 mg, 1 time/w, 3-6 times | 20 mg | 7–10 weeks | Millar, Un | O1,3 |
|
| MTs | Moderate to large | Un | Un | >2 | 30/30 | Un | 47–73 | Thora* | 500 mg, 1 time/w, 4 times (40 mg) | 60 mg | 8 weeks | Ostrowskimj, Un | O1,3 |
|
| MTs | Un | >50 | Un | >3 | 47/36 | 38/45 | 30–70 | IPC | 800 mg, 1 time/w, 3 times | 30 mg/m2 | 10 weeks | Ostrowskimj, WHO | O1,3 |
|
| MTs | Un | ≥60 | Un | >3 | 20/20 | Un | 32–76 | IPC | 150 mg, 1 time/w, 3 times | 60 mg | 8 weeks | Ostrowskimj, WHO | O1-3 |
|
| MTs | Un | >50 | Un | >3 | 30/30 | 27/33 | 33–74 | Thora* | 200 mg, 1 time/w, 4 times (40 mg) | 60 mg | 8 weeks | Ostrowskimj, WHO | O1-3 |
|
| MTs | Un | Un | Un | Un | 82/70 | 90/62 | 35–85 | IPC | 200 mg, 1 time/w, 2 times | 40 mg | 8–10 weeks | Millar, Un | O1 |
| Matrine and carboplatin versus carboplatin (one trial) | ||||||||||||||
|
| MTs | Un | Un | Un | Un | 40/38 | 41/37 | 35–76 | Un | 200 mg, 1 time/w, 3–6 times | 50–100 mg | 7–10 weeks | Millar, Un | O1,3,4 |
| Outcomes | Trials |
| Sclerosants (events/total) | Statistical method | Odds ratios 95% CI |
|
|
|---|---|---|---|---|---|---|---|
| a. Compound | |||||||
| CKI versus cisplatin | |||||||
| Complete response | 9 | 87/281 | 85/287 | Fixed-effects model | 1.10 [0.76, 1.60] | 0% | p = 0.60 |
| Pleurodesis failure | 9 | 87/281 | 103/287 | Fixed-effects model | 0.80 [0.56, 1.14] | 0% | p = 0.21 |
| Pleural progression | 6 | 18/175 | 26/173 | Fixed-effects model | 0.63 [0.33, 1.21] | 0% | p = 0.17 |
| CKI versus interleukin-2 | |||||||
| Complete response | 1 | 45/65 | 31/63 | Not applicable | 2.32 [1.13, 4.78] | No |
|
| Pleurodesis failure | 1 | 9/65 | 25/63 | Not applicable | 0.24 [0.10, 0.58] | No |
|
| CKI versus mitomycin | |||||||
| Complete response | 1 | 16/50 | 15/50 | Not applicable | 1.10 [0.47, 2.56] | No |
|
| Pleurodesis failure | 1 | 22/50 | 21/50 | Not applicable | 1.09 [0.49, 2.40] | No |
|
| b. CKI and sclerosants ( | |||||||
| CKI and cisplatin versus cisplatin | |||||||
| Complete response | 41 | 649/1,424 | 342/1,399 | Fixed-effects model | 2.71 [2.30, 3.19] | 0% | p < 0.00001 |
| Pleurodesis failure | 41 | 235/1,424 | 590/1,399 | Fixed-effects model | 0.26 [0.22, 0.32] | 0% | p < 0.00001 |
| Pleural progression | 13 | 25/481 | 90/475 | Fixed-effects model | 0.22 [0.14, 0.36] | 0% | p < 0.00001 |
| CKI and nedaplatin versus nedaplatin | |||||||
| Complete response | 3 | 44/129 | 30/129 | Fixed-effects model | 1.72 [0.99, 2.98] | 0% |
|
| Pleurodesis failure | 3 | 28/129 | 58/129 | Fixed-effects model | 0.33 [0.19, 0.57] | 0% |
|
| CKI and lobaplatin versus lobaplatin | |||||||
| Complete response | 2 | 26/55 | 20/55 | Fixed-effects model | 1.57 [0.73, 3.36] | 44% | p = 0.25 |
| Pleurodesis failure | 2 | 9/55 | 18/55 | Fixed-effects model | 0.35 [0.13, 0.93] | 0% | p = 0.04 |
| Pleural progression | 1 | 1/25 | 1/25 | Not applicable | 0.11 [0.01, 0.95] | No | p = 0.04 |
| CKI and bleomycin versus bleomycin | |||||||
| Complete response | 3 | 33/77 | 16/69 | Fixed-effects model | 2.62 [1.23, 5.58] | 0% | p = 0.01 |
| Pleurodesis failure | 3 | 12/77 | 30/69 | Fixed-effects model | 0.23 [0.11, 0.52] | 0% | p = 0.0004 |
| CKI and hydroxycamptothecin versus hydroxycamptothecin | |||||||
| Complete response | 2 | 41/78 | 21/78 | Fixed-effects model | 3.01 [1.54, 5.87] | 0% | p = 0.001 |
| Pleurodesis failure | 3 | 15/120 | 33/118 | Fixed-effects model | 0.37 [0.19, 0.72] | 0% | p = 0.004 |
| CKI and interleukin-2 versus interleukin-2 | |||||||
| Complete response | 2 | 29/56 | 13/51 | Fixed-effects model | 3.21 [1.41, 7.34] | 0% | p = 0.006 |
| Pleurodesis failure | 2 | 9/56 | 22/51 | Fixed-effects model | 0.24 [0.10, 0.60] | 0% | p = 0.002 |
| Pleural progression | 1 | 0/26 | 4/21 | Not applicable | 0.07 [0.00, 1.45] | No | p = 0.09 |
| CKI and OK-432 versus OK-432 | |||||||
| Complete response | 2 | 24/84 | 17/84 | Fixed-effects model | 1.58 [0.77, 3.21] | 0% | p = 0.21 |
| Pleurodesis failure | 2 | 24/84 | 17/84 | Fixed-effects model | 0.32 [0.16, 0.67] | 0% | p = 0.002 |
| CKI and mitomycin versus mitomycin | |||||||
| Complete response | 1 | 14/60 | 13/60 | Not applicable | 1.10 [0.47, 2.59] | No | p = 0.83 |
| Pleurodesis failure | 1 | 11/60 | 21/60 | Not applicable | 0.42 [0.18, 0.97] | No | p = 0.04 |
| CKI and carboplatin versus carboplatin | |||||||
| Complete response | 1 | 11/21 | 6/20 | Not applicable | 2.57 [0.71, 9.27] | No | p = 0.15 |
| Pleurodesis failure | 1 | 3/21 | 9/20 | Not applicable | 0.20 [0.05, 0.92] | No | p = 0.04 |
| Pleural progression | 1 | 0/21 | 3/20 | Not applicable | 0.12 [0.01, 2.41] | No | p = 0.16 |
| CKI and | |||||||
| Complete response | 1 | 18/45 | 13/45 | Not applicable | 1.64 [0.68, 3.95] | No | p = 0.27 |
| Pleurodesis failure | 1 | 4/45 | 16/45 | Not applicable | 0.18 [0.05, 0.58] | No | p = 0.004 |
| c. | |||||||
|
| |||||||
| Complete response | 5 | 56/144 | 25/144 | Fixed-effects model | 3.04 [1.76, 5.26] | 0% |
|
| Pleurodesis failure | 6 | 26/168 | 69/166 | Fixed-effects model | 0.23 [0.14, 0.41] | 0% | P < 0.00001 |
| Pleural progression | 1 | 3/20 | 8/20 | Not applicable | 0.26 [0.06, 1.21] | No | p = 0.09 |
|
| |||||||
| Complete response | 1 | 9/25 | 6/23 | Not applicable | 1.59 [0.46, 5.50] | No | p = 0.46 |
| Pleurodesis failure | 1 | 4/25 | 8/23 | Not applicable | 0.36 [0.09, 1.41] | No | p = 0.14 |
| d. Matrine injection ( | |||||||
| Matrine and cisplatin versus cisplatin (six trials) | |||||||
| Complete response | 6 | 106/249 | 66/222 | Fixed-effects model | 1.87 [1.26, 2.78] | 0% | p = 0.002 |
| Pleurodesis failure | 6 | 32/249 | 74/222 | Fixed-effects model | 0.27 [0.17, 0.44] | 0% | P < 0.00001 |
| Pleural progression | 2 | 4/122 | 11/106 | Fixed-effects model | 0.29 [0.09, 0.95] | 0% | p = 0.04 |
| Matrine and carboplatin versus carboplatin | |||||||
| Complete response | 1 | 23/40 | 16/38 | Not applicable | 1.86 [0.76, 4.57] | No | p = 0.18 |
| Pleurodesis failure | 1 | 4/40 | 12/38 | Not applicable | 0.24 [0.07, 0.83] | No | p = 0.02 |
| Pleural progression | 1 | 1/40 | 6/38 | Not applicable | 0.14 [0.02, 1.20] | No | p = 0.07 |
| Outcomes | Trials |
| Sclerosants (events/total) | Statistical method | Odds ratios 95% CI |
|
|
|---|---|---|---|---|---|---|---|
| a. Compound kushen injection (CKI) versus cisplatin | |||||||
| Quality of life ( | 6 | 144/207 | 127/212 | Random-effects model | 1.52 [0.69, 3.35] | 67% |
|
| Myelosuppression ( | 6 | 3/193 | 109/197 | Random-effects model | 0.02 [0.00, 0.15] | 69% |
|
| Leukopenia ( | 3 | 2/88 | 22/90 | Fixed-effects model | 0.10 [0.03, 0.35] | 0% |
|
| Gastrointestinal reaction ( | 9 | 10/281 | 167/287 | Random-effects model | 0.03 [0.01, 0.12] | 67% |
|
| Hepatotoxicity ( | 6 | 1/201 | 22/197 | Fixed-effects model | 0.09 [0.02, 0.33] | 0% |
|
| Nephrotoxicity ( | 7 | 1/221 | 26/217 | Fixed-effects model | 0.09 [0.03, 0.29] | 0% |
|
| Cardiotoxicity ( | 1 | 0/30 | 0/30 | Not applicable | Not estimable | No | No |
| Thoracodynia ( | 6 | 22/175 | 74/173 | Random-effects model | 0.15 [0.04, 0.48] | 69% | p = 0.002 |
| Fever ( | 5 | 29/159 | 31/158 | Random-effects model | 0.67 [0.12, 3.76] | 81% |
|
| b. CKI and cisplatin versus cisplatin | |||||||
| Quality of life ( | 19 | 497/682 | 298/670 | Fixed-effects model | 3.60 [2.84, 4.56] | 0% | p < 0.00001 |
| Myelosuppression ( | 17 | 149/574 | 229/558 | Fixed-effects model | 0.34 [0.24, 0.47] | 0% |
|
| Leukopenia ( | 20 | 178/711 | 291/703 | Fixed-effects model | 0.35 [0.26, 0.46] | 0% |
|
| Anemia ( | 2 | 5/120 | 7/118 | Fixed-effects model | 0.69 [0.21, 2.24] | 0% |
|
| Thrombocytopenia ( | 5 | 7/215 | 9/213 | Fixed-effects model | 0.76 [0.27, 2.12] | 0% |
|
| Gastrointestinal reaction ( | 31 | 254/1,053 | 440/1,035 | Fixed-effects model | 0.36 [0.29, 0.44] | 8% |
|
| Hepatotoxicity ( | 22 | 43/837 | 87/824 | Fixed-effects model | 0.42 [0.28, 0.63] | 0% |
|
| Nephrotoxicity ( | 31 | 75/1,105 | 169/1,090 | Fixed-effects model | 0.32 [0.24, 0.44] | 0% | p < 0.00001 |
| Cardiotoxicity ( | 5 | 0/152 | 0/151 | Not applicable | Not estimable | No | No |
| Thoracodynia ( | 11 | 49/402 | 66/394 | Fixed-effects model | 0.65 [0.42, 1.00] | 0% |
|
| Fever ( | 26 | 65/853 | 97/828 | Fixed-effects model | 0.50 [0.30, 0.82] | 0% |
|
| TRAEs ( | 3 | 0/144 | 0/140 | Not applicable | Not estimable | No | No |
| c. | |||||||
| Quality of life ( | 2 | 34/57 | 15/55 | Fixed-effects model | 3.95 [1.78, 8.74] | 0% | p = 0.0007 |
| Leukopenia ( | 4 | 31/113 | 67/110 | Fixed-effects model | 0.20 [0.11, 0.38] | 25% |
|
| Gastrointestinal reaction ( | 5 | 42/133 | 65/131 | Fixed-effects model | 0.34 [0.19, 0.63] | 0% |
|
| Hepatotoxicity ( | 1 | 0/24 | 0/22 | Not applicable | Not estimable | No | No |
| Nephrotoxicity ( | 2 | 0/57 | 0/55 | Not applicable | Not estimable | No | No |
| Thoracodynia ( | 2 | 5/60 | 10/57 | Fixed-effects model | 0.41 [0.13, 1.29] | 0% |
|
| Fever ( | 1 | 2/36 | 2/35 | Not applicable | 0.97 [0.13, 7.30] | No |
|
| TRAEs ( | 1 | 0/24 | 0/22 | Not applicable | Not estimable | No | No |
| d. Matrine and cisplatin versus cisplatin | |||||||
| Quality of life ( | 2 | 32/50 | 20/50 | Fixed-effects model | 2.95 [1.25, 6.97] | 0% | p = 0.02 |
| Myelosuppression ( | 3 | 14/97 | 19/86 | Fixed-effects model | 0.49 [0.21, 1.11] | 43% | P = 0.09 |
| Leukopenia ( | 2 | 7/70 | 31/66 | Random-effects model | 0.10 [0.02, 0.61] | 66% | P = 0.01 |
| Anemia ( | 1 | 14/30 | 26/30 | Not applicable | 0.13 [0.04, 0.48] | No |
|
| Thrombocytopenia ( | 1 | 8/30 | 9/30 | Not applicable | 0.85 [0.28, 2.61] | No |
|
| Gastrointestinal reaction ( | 5 | 36/167 | 55/152 | Fixed-effects model | 0.35 [0.19, 0.66] | 0% |
|
| Hepatotoxicity ( | 3 | 15/117 | 22/102 | Fixed-effects model | 0.52 [0.23, 1.15] | 0% |
|
| Nephrotoxicity ( | 4 | 7/137 | 11/122 | Fixed-effects model | 0.56 [0.19, 1.59] | 0% |
|
| Cardiotoxicity ( | 1 | 0/20 | 0/20 | Not applicable | Not estimable | No | No |
| Thoracodynia ( | 4 | 9/120 | 31/116 | Fixed-effects model | 0.21 [0.10, 0.48] | 0% |
|
| Fever ( | 4 | 7/147 | 15/132 | Fixed-effects model | 0.41 [0.16, 1.07] | 0% |
|
| TRAEs ( | 1 | 0/20 | 0/20 | Not applicable | Not estimable | No | No |
| Subgroups | Trials | Cases | Complete response | Pleurodesis failure | ||||
|---|---|---|---|---|---|---|---|---|
| Odds ratios (95%CI) | Univariable* | Multiple* | Odds ratios (95%CI) | Univariable* | Multiple* | |||
| a. Subgroups analysis via primary disease ( | ||||||||
| Miscellaneous tumors | 28 | 2053 | 2.77 [2.29, 3.37] | 0.69 | 0.65 | 0.25 [0.20, 0.31] | 0.89 | 0.89 |
| Lung cancer | 12 | 724 | 2.68 [1.93, 3.72] | 0.29 [0.21, 0.40] | ||||
| Hematologic malignancies | 1 | 46 | 1.10 [0.30, 3.98] | 0.58 [0.16, 2.07] | ||||
| b Subgroup analysis via pleural effusion ( | ||||||||
| Small to large | 1 | 52 | 1.87 [0.52, 6.73] | 0.12 | 0.28 | 0.47 [0.23, 0.95] | 0.49 | 0.71 |
| Moderate to large | 10 | 640 | 2.15 [1.51, 3.05] | 0.30 [0.21, 0.43] | ||||
| Large | 3 | 158 | 2.32 [1.20, 4.50] | 0.28 [0.13, 0.59] | ||||
| Unclear | 27 | 1973 | 2.98 [2.45, 3.63] | 0.25 [0.20, 0.31] | ||||
| c. Subgroups analysis via Karnofsky performance status score ( | ||||||||
| Karnofsky performance status score (≥50) | 7 | 404 | 2.24 [1.44, 3.49] | 0.94 | 0.38 | 0.29 [0.19, 0.45] | 0.15 | 0.55 |
| Karnofsky performance status score (≥60) | 15 | 1,195 | 2.67 [2.07, 3.44] | 0.22 [0.17, 0.29] | ||||
| Karnofsky performance status score (≥70) | 2 | 174 | 2.97 [1.52, 5.79] | 0.27 [0.12, 0.61] | ||||
| Unclear | 17 | 1,050 | 2.91 [2.22, 3.80] | 0.31 [0.23, 0.41] | ||||
| d. Subgroup analysis via anticipated survival time ( | ||||||||
| Anticipated survival time (unclear) | 26 | 1803 | 2.83 [2.31, 3.47] | 0.74 | 0.77 | 0.28 [0.23, 0.35] | 0.53 | 0.52 |
| Anticipated survival time (≥3 months) | 13 | 922 | 2.41 [1.79, 3.25] | 0.22 [0.16, 0.31] | ||||
| Anticipated survival time (≥1 months) | 2 | 98 | 3.30 [1.40, 7.82] | 0.38 [0.15, 0.99] | ||||
| e. Subgroup analysis via treatment history ( | ||||||||
| Primary treatment | 9 | 549 | 2.49 [1.71, 3.63] | 0.23 | 0.88 | 0.28 [0.19, 0.41] | 0.47 | 0.60 |
| Retreatment | 2 | 112 | 1.57 [0.67, 3.67] | 0.36 [0.16, 0.81] | ||||
| Others | 30 | 2,162 | 2.84 [2.35, 3.43] | 0.25 [0.21, 0.31] | ||||
| f. Subgroup analysis via the drainage method ( | ||||||||
| Indwelling pleural catheter | 33 | 2,349 | 2.63 [2.19, 3.16] | 0.68 | 0.76 | 0.24 [0.20, 0.29] | 0.04 | 0.08 |
| Thoracentesis | 8 | 474 | 3.09 [2.09, 4.56] | 0.40 [0.26, 0.62] | ||||
| g. Subgroups analysis via CKI dosage ( | ||||||||
| Compound | 31 | 2045 | 2.60 [2.15, 3.16] | 0.72 | 0.61 | 0.27 [0.22, 0.33] | 0.92 | 0.90 |
| Compound | 8 | 676 | 3.27 [2.32, 4.59] | 0.24 [0.17, 0.34] | ||||
| Compound | 2 | 102 | 1.71 [0.71, 4.13] | 0.37 [0.16, 0.89] | ||||
| h. Subgroups analysis via treatment frequency ( | ||||||||
| One time/week | 35 | 2,493 | 2.62 [2.20, 3.11] | 0.25 | 0.67 | 0.27 [0.23, 0.33] | 0.34 | 0.96 |
| Others (1–2 times/week or 2–3 time/week) | 6 | 330 | 3.66 [2.18, 6.14] | 0.20 [0.12, 0.34] | ||||
| i Subgroups analysis via treatment times ( | ||||||||
| Two to four times | 25 | 1783 | 2.49 [2.02, 3.06] | 0.27 | 0.59 | 0.27 [0.22, 0.34] | 0.76 | 0.46 |
| Others (>4 times or unclear) | 16 | 1,040 | 3.13 [2.39, 4.11] | 0.25 [0.19, 0.34] | ||||
| j Subgroup analysis via cisplatin dosage ( | ||||||||
| Cisplatin (20–30 mg each time) | 6 | 450 | 2.47 [1.60, 3.83] | 0.31 | 0.62 | 0.23 [0.15, 0.36] | 0.92 | 0.93 |
| Cisplatin 40–50 mg each time) | 18 | 1,119 | 2.55 [1.98, 3.29] | 0.28 [0.21, 0.37] | ||||
| Cisplatin (60–80 mg each time) | 11 | 724 | 2.71 [1.95, 3.77] | 0.31 [0.22, 0.44] | ||||
| Cisplatin (others) | 6 | 530 | 3.31 [2.25, 4.85] | 0.22 [0.15, 0.33] | ||||
| k Subgroups analysis via dosage difference of cisplatin ( | ||||||||
| Equivalent dosage | 35 | 2,439 | 2.58 [2.16, 3.08] | 0.33 | 0.43 | 0.26 [0.21, 0.31] | 0.49 | 0.95 |
| Low vs. high dosage | 6 | 384 | 3.64 [2.34, 5.67] | 0.31 [0.19, 0.50] | ||||
| l Subgroups analysis via criterion ( | ||||||||
| Millar | 28 | 1867 | 2.49 [2.04, 3.04] | 0.16 | 0.18 | 0.27 [0.21, 0.33] | 0.88 | 0.86 |
| Ostrowskimj | 13 | 956 | 3.23 [2.40, 4.33] | 0.26 [0.19, 0.35] | ||||
| Indicators | Trials | Compound | Cisplatin (events/total) | OR (95% CI) | Egger’s test | Risk assessment | ||
|---|---|---|---|---|---|---|---|---|
| Coefficient | 95% CI | P>|t| | ||||||
| Complete response | 41 | 649/1,424 | 342/1,399 | 2.71 [2.30, 3.19] | −1.07 | −2.52 to 0.38 | 0.14 | Objective |
| Pleurodesis failure | 41 | 235/1,424 | 590/1,399 | 0.26 [0.22, 0.32] | 0.13 | −1.35 to 1.60 | 0.87 | Objective |
| Pleural progression | 13 | 25/481 | 90/475 | 0.22 [0.14, 0.36] | −0.28 | −2.93 to 2.37 | 0.82 | Objective |
| Quality of life | 19 | 497/682 | 298/670 | 3.60 [2.84, 4.56] | −2.47 | −4.62 to -0.32 | 0.03 | Underestimation |
| Myelosuppression | 17 | 149/574 | 229/558 | 0.34 [0.24, 0.47] | 1.20 | −1.76 to 4.16 | 0.39 | Objective |
| Leukopenia | 20 | 178/711 | 291/703 | 0.35 [0.26, 0.46] | −0.45 | −1.59 to 0.67 | 0.41 | Objective |
| Gastrointestinal reactions | 31 | 254/1,053 | 440/1,035 | 0.36 [0.29, 0.44] | −1.46 | −2.71 to -0.21 | 0.02 | Underestimation |
| Hepatotoxicity | 22 | 43/837 | 87/824 | 0.42 [0.28, 0.63] | −0.007 | −0.76 to 0.78 | 0.98 | Objective |
| Nephrotoxicity | 31 | 75/1,105 | 169/1,090 | 0.32 [0.24, 0.44] | −0.15 | −0.91 to 0.60 | 0.67 | Objective |
| Thoracodynia | 11 | 49/402 | 66/394 | 0.66 [0.43, 1.02] | 0.06 | −1.49 to 1.61 | 0.93 | Objective |
| Fever | 26 | 65/853 | 97/828 | 0.50 [0.33, 0.76] | 0.35 | −1.42 to 2.13 | 0.68 | Objective |
| Outcomes | Before excluding trials | Excluded trials with high risk and over-estimating efficacy and safety | After excluding trials | Sensitivity | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Trials | SM | OR (95% CI) | I2 | P | Trials | SM | OR (95% CI) | I2 | P | |||
| a. Compound | ||||||||||||
| CKI versus cisplatin | ||||||||||||
| Complete response | 9 | FEM | 1.10 [0.76, 1.60] | 0% |
| Poor*: ( | 8 | FEM | 1.07 [0.73, 1.58] | 0% | p = 0.72 | Robustness |
| Pleurodesis failure | 9 | FEM | 0.80 [0.56, 1.14] | 0% | p = 0.21 | Poor*: ( | 8 | FEM | 0.76 [0.52, 1.11] | 0% | p = 0.15 | Robustness |
| Pleural progression | 6 | FEM | 0.63 [0.33, 1.21] | 0% | p = 0.17 | Poor*:no, Under*:no | 6 | FEM | 0.63 [0.33, 1.21] | 0% | p = 0.17 | Robustness |
| Quality of life | 6 | REM | 1.52 [0.69, 3.35] | 67% | p = 0.30 | Poor*: ( | No | No | No | No | No | Poor |
| Myelosuppression | 6 | REM | 0.02 [0.00, 0.15] | 69% | p < 0.0001 | Poor*:no ( | 1 | No | 0.46 [0.09, 2.41] | No |
| Poor |
| Neutropenia | 4 | FEM | 0.10 [0.03, 0.35] | 0% |
| Poor*: ( | 2 | FEM | 0.07 [0.01, 0.60] | 0% | p = 0.01 | Robustness |
| Gastrointestinal reaction | 9 | REM | 0.03 [0.01, 0.12] | 67% |
| Poor*: ( | 2 | REM | 0.26 [0.02, 3.08] | 57% | p = 0.28 | Poor |
| Hepatotoxicity | 6 | FEM | 0.09 [0.02, 0.33] | 0% | p = 0.0003 | Poor*: ( | 4 | FEM | 0.19 [0.04, 0.92] | 0% | p = 0.04 | Robustness |
| Nephrotoxicity | 7 | FEM | 0.09 [0.03, 0.29] | 0% |
| Poor*: ( | 5 | FEM | 0.16 [0.04, 0.63] | 0% |
| Robustness |
| Thoracodynia | 6 | REM | 0.15 [0.04, 0.48] | 69% | p = 0.002 | Poor*: ( | 1 | Not | 0.97 [0.34, 2.78] | No | p = 0.96 | Poor |
| Fever | 5 | REM | 0.67 [0.12, 3.76] | 81% |
| Poor*: ( | 3 | REM | 1.96 [0.09, 43.10] | 88% | p = 0.67 | Robustness |
| b. CKI and sclerosants | ||||||||||||
| CKI and cisplatin versus cisplatin | ||||||||||||
| Complete response | 41 | FEM | 2.71 [2.30, 3.19] | 0% | p < 0.00001 | Poor*: ( | 26 | FEM | 1.94 [1.56, 2.43] | 0% | p < 0.00001 | Robustness |
| Pleurodesis failure | 41 | FEM | 0.26 [0.22, 0.32] | 0% | p < 0.00001 | Poor*: | 14 | FEM | 0.41 [0.29, 0.56] | 0% | p < 0.00001 | Robustness |
| Pleural progression | 13 | FEM | 0.22 [0.14, 0.36] | 0% | p < 0.00001 | Poor*:no, Under*: ( | 9 | FEM | 0.35 [0.19, 0.64] | 0% | P = 0.0006 | Robustness |
| Quality of life | 19 | FEM | 3.60 [2.84, 4.56] | 0% | p < 0.00001 | Poor*: ( | No | No | No | No | No | Poor |
| Myelosuppression | 17 | FEM | 0.34 [0.24, 0.47] | 0% | p < 0.00001 | Poor*: ( | 5 | FEM | 0.35 [0.18, 0.69] | 0% | p = 0.002 | Robustness |
| Neutropenia | 20 | FEM | 0.35 [0.26, 0.46] | 0% | p < 0.00001 | Poor*: ( | 4 | FEM | 0.43 [0.23, 0.82] | 0% | P = 0.01 | Robustness |
| Thrombocytopenia | 5 | FEM | 0.76 [0.27, 2.12] | 0% | p = 0.61 | Poor*: ( | 2 | Not | Not | Not | Not | Poor |
| Anemia | 2 | FEM | 0.69 [0.21, 2.24] | 0% | p = 0.54 | Poor*: ( | No | No | No | No | No | Poor |
| Gastrointestinal reaction | 31 | FEM | 0.37 [0.30, 0.47] | 8% | p < 0.00001 | Poor*: ( | 7 | FEM | 0.48 [0.31, 0.74] | 0% | P = 0.0009 | Robustness |
| Hepatotoxicity | 22 | FEM | 0.42 [0.28, 0.63] | 0% | p < 0.0001 | Poor*: ( | 11 | FEM | 0.37 [0.22, 0.63] | 0% | p = 0.0002 | Robustness |
| Nephrotoxicity | 31 | FEM | 0.32 [0.24, 0.44] | 0% | p < 0.0001 | Poor*: ( | 12 | FEM | 0.35 [0.21, 0.59] | 0% | p < 0.0001 | Robustness |
| Thoracodynia | 11 | FEM | 0.65 [0.42, 1.00] | 0% | p = 0.05 | Poor*: ( | 6 | FEM | 0.50 [0.28, 0.89] | 0% | p = 0.02 | Robustness |
| Fever | 15 | FEM | 0.50 [0.30, 0.82] | 0% | p = 0.006 | Poor*: ( | 7 | FEM | 0.35 [0.15, 0.79] | 0% | p = 0.01 | Robustness |
| CKI and nedaplatin versus nedaplatin | ||||||||||||
| Complete response | 3 | FEM | 1.72 [0.99, 2.98] | 0% | p = 0.05 | Poor*:no, Over*:no | 3 | FEM | 1.72 [0.99, 2.98] | 0% | p = 0.05 | Robustness |
| Pleurodesis failure | 3 | FEM | 0.33 [0.19, 0.57] | 0% | p < 0.0001 | Poor*:no, Under*: ( | No | No | No | No | No | Poor |
| CKI and lobaplatin versus lobaplatin | ||||||||||||
| Complete response | 2 | FEM | 1.57 [0.73, 3.36] | 44% | p = 0.25 | Poor*:no, Over *:no | 2 | FEM | 1.57 [0.73, 3.36] | 44% | p = 0.25 | Robustness |
| Pleurodesis failure | 2 | FEM | 0.35 [0.13, 0.93] | 0% | p = 0.04 | Poor*:no, Under*: ( | 1 | No | 0.46 [0.08, 2.75] | No | p = 0.40 | Poor |
| CKI and bleomycin versus bleomycin | ||||||||||||
| Complete response | 3 | FEM | 2.62 [1.23, 5.58] | 0% | p = 0.01 | Poor*:no, Over *: ( | 2 | FEM | 2.17 [0.91, 5.16] | 0% | p = 0.08 | Poor |
| Pleurodesis failure | 3 | FEM | 0.23 [0.11, 0.52] | 0% | p = 0.0004 | Poor*:no, Under*: ( | 1 | No | 0.13 [0.01, 1.29] | No | p = 0.08 | Poor |
| CKI and hydroxycamptothecin versus hydroxycamptothecin | ||||||||||||
| Complete response | 2 | FEM | 3.01 [1.54, 5.87] | 0% | p = 0.001 | Poor*:no, Under*: ( | No | No | No | No | No | Poor |
| Pleurodesis failure | 3 | FEM | 0.37 [0.19, 0.72] | 0% | p = 0.004 | Poor*: ( | 1 | No | 0.55 [0.16, 1.93] | No | p = 0.35 | Poor |
| CKI and interleukin-2 versus interleukin-2 | ||||||||||||
| Complete response | 2 | FEM | 3.21 [1.41, 7.34] | 0% | p = 0.006 | Poor*:no, Under*: ( | 1 | No | 2.67 [0.92, 7.70] | No | p = 0.07 | Poor |
| Pleurodesis failure | 2 | FEM | 0.24 [0.10, 0.60] | 0% | p = 0.002 | Poor*:no, Under*: ( | No | No | No | No | No | Poor |
| CKI and OK-432 versus OK-432 | ||||||||||||
| Complete response | 2 | FEM | 1.58 [0.77, 3.21] | 0% | p = 0.21 | Poor*:no, Over*:no | 2 | FEM | 1.58 [0.77, 3.21] | 0% | p = 0.21 | Robustness |
| Pleurodesis failure | 2 | FEM | 0.32 [0.16, 0.67] | 0% | p = 0.002 | Poor*:no, Under*: ( | No | No | No | No | No | Poor |
| c. | ||||||||||||
| Complete response | 5 | FEM | 3.04 [1.76, 5.26] | 0% | p < 0.0001 | Poor*:no, Over*: ( | 2 | FEM | 2.00 [0.72, 5.57] | 0% | p = 0.18 | Poor |
| Pleurodesis failure | 6 | FEM | 0.23 [0.14, 0.41] | 0% | P < 0.00001 | Poor*: ( | 2 | FEM | 0.49 [0.18, 1.31] | 0% | P = 0.15 | Poor |
| Quality of life | 2 | FEM | 3.95 [1.78, 8.74] | 0% | p = 0.0007 | Poor*: ( | No | No | No | No | No | Poor |
| Neutropenia | 4 | FEM | 0.20 [0.11, 0.38] | 25% | p < 0.0001 | Poor*: ( | No | No | No | No | No | Poor |
| Gastrointestinal reaction | 5 | FEM | 0.34 [0.19, 0.63] | 0% | p = 0.0006 | Poor*: ( | No | No | No | No | No | Poor |
| Thoracodynia | 2 | FEM | 0.41 [0.13, 1.29] | 0% | p = 0.13 | Poor*: ( | No | No | No | No | No | Poor |
| d. Matrine and cisplatin versus cisplatin (six trials) | ||||||||||||
| Complete response | 6 | FEM | 1.87 [1.26, 2.78] | 0% | p = 0.002 | Poor*:no, Over*: ( | 5 | FEM | 1.73 [1.13, 2.66] | 0% | p = 0.01 | Robustness |
| Pleurodesis failure | 6 | FEM | 0.27 [0.17, 0.44] | 0% | P < 0.00001 | Poor*:no, Under*: ( | 2 | FEM | 0.32 [0.16, 0.64] | 0% | P = 0.001 | Robustness |
| Pleural progression | 2 | FEM | 0.29 [0.09, 0.95] | 0% | p = 0.04 | Poor*:no, Under*:no | 2 | FEM | 0.29 [0.09, 0.95] | 0% | p = 0.04 | Robustness |
| Quality of life | 2 | FEM | 2.93 [1.23, 6.96] | 0% | p = 0.02 | Poor*: ( | No | No | No | No | No | Poor |
| Myelosuppression | 3 | FEM | 0.49 [0.21, 1.11] | 43% | P = 0.09 | Poor*: ( | No | No | No | No | No | Poor |
| Neutropenia | 2 | REM | 0.10 [0.02, 0.61] | 66% | P = 0.01 | Poor*:no, Under*: ( | 1 | No | 0.26 [0.05, 1.40] | No | P = 0.12 | Poor |
| Gastrointestinal reaction | 5 | FEM | 0.35 [0.19, 0.66] | 0% | p = 0.001 | Poor*: ( | 1 | No | 0.42 [0.07, 2.45] | No | p = 0.34 | Poor |
| Hepatotoxicity | 3 | FEM | 0.52 [0.23, 1.15] | 0% | p = 0.10 | Poor*: ( | 2 | FEM | 0.40 [0.16, 1.04] | 0% | p = 0.06 | Robustness |
| Nephrotoxicity | 4 | FEM | 0.56 [0.19, 1.59] | 0% | p = 0.27 | Poor*: ( | 2 | FEM | 0.56 [0.19, 1.59] | 0% | p = 0.27 | Robustness |
| Thoracodynia | 4 | FEM | 0.21 [0.10, 0.48] | 0% | p = 0.0007 | Poor*: ( | 2 | FEM | 0.24 [0.09, 0.64] | 0% | p = 0.004 | Robustness |
| Fever | 4 | FEM | 0.41 [0.16, 1.07] | 0% | p = 0.07 | Poor*: ( | 2 | FEM | 0.57 [0.17, 1.86] | 0% | p = 0.35 | Robustness |
| Outcomes (trials, patients) | Relative risk reduction (RRR) | Incidence | I2 | D2 | RIS | % of RIS attained | Z-curve passed conventional boundaries? | Z-curve passed TSA/futility boundaries? | Z-curve passed RIS? |
|---|---|---|---|---|---|---|---|---|---|
| a. Compound | |||||||||
| Complete response (9 trials, n = 568) | 25% | 30% | 0% | 0% | 1,081 | 52.54 | No | Yes | No |
| Pleurodesis failure (9 trials, n = 568) | 25% | 36% | 0% | 0% | 837 | 67.86 | No | Yes | No |
| Pleural progression (6 trials, n = 348) | 25% | 16% | 0% | 0% | 2,363 | 14.73 | No | No | No |
| b. CKI and cisplatin versus cisplatin ( | |||||||||
| Complete response (41 trials, n = 2,823) | 25% | 24% | 0% | 0% | 1,447 | 195.09 | Yes | Yes | Yes |
| Pleurodesis failure (41 trials, n = 2,823) | 25% | 42% | 0% | 0% | 662 | 426.44 | Yes | Yes | Yes |
| Pleural progression (13 trials, n = 956) | 25% | 19% | 0% | 0% | 1929 | 49.56 | Yes | Yes | No |
| Quality of life (19 trials, n = 1,352) | 25% | 44% | 0% | 0% | 615 | 219.84 | Yes | Yes | Yes |
| Myelosuppression (17 trials, n = 1,132) | 20% | 38% | 0% | 0% | 1,224 | 92.48 | Yes | Yes | No |
| Neutropenia (20 trials, n = 1,414) | 20% | 41% | 0% | 0% | 1,088 | 130.00 | Yes | Yes | Yes |
| Gastrointestinal reaction (31 trials, n = 2088) | 20% | 41% | 19% | 22% | 1,394 | 149.78 | Yes | Yes | Yes |
| Hepatotoxicity (22 trials, n = 1,661) | 20% | 11% | 0% | 0% | 5,787 | 28.70 | Yes | Yes | No |
| Nephrotoxicity (31 trials, n = 2,195) | 20% | 16% | 0% | 0% | 3,780 | 58.07 | Yes | Yes | No |
| Fever (15 trials, n = 954) | 20% | 10% | 0% | 0% | 6,429 | 14.84 | 9 | No | No |
| c. | |||||||||
| Complete response (5 trials, n = 288) | 25% | 17% | 0% | 0% | 2,201 | 13.08 | Yes | No | No |
| Pleurodesis failure (6 trials, n = 334) | 25% | 42% | 0% | 0% | 662 | 50.45 | Yes | Yes | No |
| c. Matrine and cisplatin versus cisplatin ( | |||||||||
| Complete response (6 trials, n = 471) | 25% | 30% | 0% | 0% | 1,081 | 43.57 | Yes | No | No |
| Pleurodesis failure (6 trials, n = 471) | 25% | 33% | 0% | 0% | 948 | 49.68 | Yes | Yes | No |
| Outcomes (trials) | Quality assessment | Malignant pleural effusion | Clinical effectiveness and safety | Quality | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| i | ii | iii | iv | v | RSF | Sclerosants | Odds ratios (95% CI) | Absolute effect | ||
| a. Compound | ||||||||||
| Complete response (9) | Serious | Not | Not | Not | None | 86/281 (30.6%) | 86/287 (30%) | 1.07 (0.74–1.54) | 14 more per 1,000 (from 59 fewer to 98 more) | ⊕⊕⊕Ο |
| Pleurodesis failure (9) | Serious | Not | Not | Not | None | 86/281 (30.6%) | 104/287(36.2%) | 0.77 (0.54 to 1.1) | 58 fewer per 1,000 (from 128 fewer to 22 more) | ⊕⊕⊕Ο |
| Pleural progression (6) | Serious | Not | Not | Not | None | 16/175 (9.1%) | 28/173 (16.2%) | 0.51 (0.26 to 0.98) | 72 fewer per 1,000 (from 3 fewer to 114 fewer) | ⊕⊕⊕Ο |
| Quality of life (6) | Very serious | Serious | Not | Not | None | 144/207 (69.6%) | 127/212 (59.9%) | 1.52 (0.69–3.35) | 95 more per 1,000 (from 91 fewer to 234 more) | ⊕ΟΟΟ |
| Myelosuppression (6) | Sery serious | serious | Not | Not | None | 3/193 (1.6%) | 109/197 (55.3%) | 0.02 (0 to 0.15) | 529 fewer per 1,000 (from 397 fewer to 553 fewer) | ⊕ΟΟΟ |
| Neutropenia (3) | Serious | Not | Not | Serious | none | 2/88 (2.3%) | 22/90 (24.4%) | 0.1 (0.03–0.35) | 213 fewer per 1,000 (from 143 fewer to 235 fewer) | ⊕⊕ΟΟ |
| Gastrointestinal reaction (9) | Very serious | Serious | Not | Not | None | 10/281 (3.6%) | 167/287 (58.2%) | 0.03 (0.01 to 0.12) | 542 fewer per 1,000 (from 439 fewer to 568 fewer) | ⊕ΟΟΟ |
| Hepatotoxicity (6) | Serious | Not | Not | Not | None | 1/201(0.5%) | 22/197(11.2%) | 0.09 (0.02 to 0.33) | 100 fewer per 1,000 (from 72 fewer to 109 fewer) | ⊕⊕⊕Ο |
| Nephrotoxicity (6) | Serious | Not | Not | Not | None | 1/221 (0.5%) | 26/217 (12%) | 0.09 (0.03 to 0.29) | 108 fewer per 1,000 (from 82 fewer to 116 fewer) | ⊕⊕⊕Ο |
| Thoracodynia (6) | Very serious | Serious | Not | Not | None | 17/159 (10.7%) | 63/158 (39.9%) | 0.14 (0.03 to 0.61) | 314 fewer per 1,000 (from 111 fewer to 379 fewer) | ⊕ΟΟΟ |
| Fever (5) | Serious | Not | Not | Not | None | 29/159 (18.2%) | 31/158 (19.6%) | 0.94 (0.55–1.59) | 10 fewer per 1,000 (from 78 fewer to 83 more) | ⊕⊕⊕Ο |
| Table 8b. Intrapleural administration with CKI and sclerosants | ||||||||||
| CKI and Cisplatin versus cisplatin | ||||||||||
| Complete response (41) | Serious | Not | Not | Not | None | 649/1,424 (45.6%) | 342/1,399 (24.4%) | 2.71 (2.3 to 3.19) | 223 more per 1,000 (from 182 more to 263 more) | ⊕⊕⊕Ο |
| Pleurodesis failure (41) | Serious | Not | Not | Not | None | 235/1,424 (16.5%) | 590/1,399 (42.2%) | 0.26 (0.22 to 0.32) | 262 fewer per 1,000 (from 233 fewer to 283 fewer) | ⊕⊕⊕Ο |
| Pleural progression (13) | Serious | Not | Not | Not | None | 25/481 (5.2%) | 90/475 (18.9%) | 0.22 (0.14–0.36) | 141 fewer per 1,000 (from 112 fewer to 158 fewer) | ⊕⊕⊕Ο |
| Quality of life (19) | Very serious | Not | Not | Not | Reporting bias | 497/682 (72.9%) | 298/670 (44.5%) | 3.56 (2.8 to 4.53) | 296 more per 1,000 (from 247 more to 339 more) | ⊕ΟΟΟ |
| Myelosuppression (17) | Serious | Not | Not | Not | None | 149/574 (26%) | 229/558 (41%) | 0.34 (0.24 to 0.47) | 219 fewer per 1,000 (from 164 fewer to 267 fewer) | ⊕⊕⊕Ο |
| Neutropenia (20) | Serious | Not | Not | Not | None | 178/711 (25%) | 291/703 (41.4%) | 0.35 (0.27–0.46) | 216 fewer per 1,000 (from 169 fewer to 254 fewer) | ⊕⊕⊕Ο |
| Thrombocytopenia (5) | Very serious | Not | Not | Not | None | 7/215 (3.3%) | 9/213 (4.2%) | 0.76 (0.27–2.12) | 10 fewer per 1,000 (from 30 fewer to 43 more) | ⊕⊕ΟΟ |
| Anemia (2) | Very serious | Not | Not | Serious | None | 5/120 (4.2%) | 7/118 (5.9%) | 0.69 (0.21–2.24) | 18 fewer per 1,000 (from 46 fewer to 64 more) | ⊕ΟΟΟ |
| Gastrointestinal reaction (31) | Serious | Not | Not | Not | None8i | 254/1,053 (24.1%) | 440/1,035 (42.5%) | 0.36 (0.29 to 0.44) | 215 fewer per 1,000 (from 180 fewer to 249 fewer) | ⊕⊕⊕Ο |
| Hepatotoxicity (22) | Serious | Not | Not | Not | None | 43/837 (5.1%) | 87/824 (10.6%) | 0.42 (0.28 to 0.63) | 58 fewer per 1,000 (from 36 fewer to 74 fewer) | ⊕⊕⊕Ο |
| Nephrotoxicity (31) | Serious | Not | Not | Not | None | 75/1,105 (6.8%) | 169/1,090 (15.5%) | 0.32 (0.24 to 0.44) | 100 fewer per 1,000 (from 80 fewer to 113 fewer) | ⊕⊕⊕Ο |
| Thoracodynia (11) | Very serious | Not | Not | Not | None | 49/402 (12.2%) | 66/394 (16.8%) | 0.65 (0.42–1) | 52 fewer per 1,000 (from 90 fewer to 0 more) | ⊕⊕ΟΟ |
| Fever (15) | Serious | Not | Not | Not | None | 25/481 (5.2%) | 47/473 (9.9%) | 0.5 (0.3–0.82) | 47 fewer per 1,000 (from 16 fewer to 67 fewer) | ⊕⊕⊕Ο |
| CKI and Nedaplatin versus nedaplatin | ||||||||||
| Complete response (3) | Serious | Not | Not | Serious | None | 44/129 (34.1%) | 30/129 (23.3%) | 1.72 (0.99–2.98) | 110 more per 1,000 (from 2 fewer to 242 more) | ⊕⊕ΟΟ |
| Pleurodesis failure (3) | Serious | Not | Not | Serious | None | 28/129 (21.7%) | 58/129 (45%) | 0.33 (0.19–0.57) | 237 fewer per 1,000 (from 132 fewer to 315 fewer) | ⊕⊕ΟΟ |
| CKI and lobaplatin versus lobaplatin | ||||||||||
| Complete response (2) | Serious | Not | Not | Serious | None | 26/55 (47.3%) | 20/55 (36.4%) | 1.57 (0.73–3.36) | 109 more per 1,000 (from 69 fewer to 294 more) | ⊕⊕ΟΟ |
| Pleurodesis failure (2) | Serious | Not | Not | Serious | None | 9/55 (16.4%) | 18/55 (32.7%) | 0.35 (0.13–0.93) | 182 fewer per 1,000 (from 16 fewer to 268 fewer) | ⊕⊕ΟΟ |
| CKI and bleomycin versus bleomycin | ||||||||||
| Complete response (3) | Serious | Not | Not | Serious | None | 33/77 (42.9%) | 16/69 (23.2%) | 2.62 (1.23–5.58) | 210 more per 1,000 (from 39 more to 396 more) | ⊕⊕ΟΟ |
| Pleurodesis failure (3) | Serious | Not | Not | Serious | None | 12/77 (15.6%) | 30/69 (43.5%) | 0.23 (0.11–0.52) | 284 fewer per 1,000 (from 149 fewer to 357 fewer) | ⊕⊕ΟΟ |
| CKI and hydroxycamptothecin versus hydroxycamptothecin | ||||||||||
| Complete response (2) | Serious | Not | Not | Serious | None | 41/78 (52.6%) | 21/78 (26.9%) | 3.01 (1.54–5.87) | 257 more per 1,000 (from 93 more to 415 more) | ⊕⊕ΟΟ |
| Pleurodesis failure (3) | Very serious | Not | Not | Serious | None | 15/120 (12.5%) | 33/118 (28%) | 0.37 (0.19–0.72) | 154 fewer per 1,000 (from 61 fewer to 211 fewer) | ⊕ΟΟΟ |
| CKI and interleukin-2 versus interleukin-2 | ||||||||||
| Complete response (2) | Serious | Not | Not | Serious | None | 29/56 (51.8%) | 13/51 (25.5%) | 3.21 (1.41–7.34) | 268 more per 1,000 (from 71 more to 460 more) | ⊕⊕ΟΟ |
| Pleurodesis failure (2) | Serious | Not | Not | Serious | None | 9/56 (16.1%) | 22/51 (43.1%) | 0.24 (0.1–0.6) | 277 fewer per 1,000 (from 119 fewer to 361 fewer) | ⊕⊕ΟΟ |
| CKI and OK-432 versus OK-432 | ||||||||||
| Complete response (2) | Serious | Not | Not | Serious | None | 24/84 (28.6%) | 17/84 (20.2%) | 1.58 (0.77–3.21) | 84 more per 1,000 (from 39 fewer to 246 more) | ⊕⊕ΟΟ |
| Pleurodesis failure (2) | Serious | Not | Not | Serious | None | 14/84 (16.7%) | 32/84 (38.1%) | 0.32 (0.16–0.67) | 216 fewer per 1,000 (from 89 fewer to 291 fewer) | ⊕⊕ΟΟ |
| c. Intrapleural administration with | ||||||||||
| Complete response (5) | Very serious | Not | Not | Not | None | 56/144 (38.9%) | 25/144 (17.4%) | 3.04 (1.76–5.26) | 216 more per 1,000 (from 96 more to 351 more) | ⊕⊕ΟΟ |
| Pleurodesis failure (6) | Very serious | Not | Not | Not | None | 26/168 (15.5%) | 69/166 (41.6%) | 0.23 (0.14–0.41) | 275 fewer per 1,000 (from 190 fewer to 325 fewer) | ⊕⊕ΟΟ |
| Quality of life (2) | Very serious | Not | Not | Serious | None | 34/57 (59.6%) | 15/55 (27.3%) | 3.95 (1.78–8.74) | 324 more per 1,000 (from 128 more to 493 more) | ⊕ΟΟΟ |
| Neutropenia (4) | Very serious | Serious | Not | Serious | None | 31/113 (27.4%) | 67/110 (60.9%) | 0.2 (0.11–0.38) | 372 fewer per 1,000 (from 237 fewer to 463 fewer) | ⊕ΟΟΟ |
| Gastrointestinal reaction (5) | Very serious | Not | Not | Serious | None | 42/133 (31.6%) | 65/131 (49.6%) | 0.34 (0.19–0.63) | 245 fewer per 1,000 (from 113 fewer to 339 fewer) | ⊕ΟΟΟ |
| Thoracodynia (2) | Very serious | Not | Not | Serious | None | 5/60 (8.3%) | 10/57 (17.5%) | 0.41 (0.13–1.29) | 95 fewer per 1,000 (from 149 fewer to 40 more) | ⊕ΟΟΟ |
| d. Intrapleural administration with matrine and cisplatin versus cisplatin | ||||||||||
| Complete response (6) | Serious | Not | Not | Not | None | 106/249 (42.6%) | 66/222 (29.7%) | 1.87 (1.26–2.78) | 144 more per 1,000 (from 50 more to 243 more) | ⊕⊕⊕Ο |
| Pleurodesis failure (6) | Serious | Not | Not | Not | None | 32/249 (12.9%) | 74/222 (33.3%) | 0.27 (0.17–0.44) | 214 fewer per 1,000 (from 153 fewer to 255 fewer) | ⊕⊕⊕Ο |
| Pleural progression (2) | Serious | Not | Not | Serious | None | 4/122 (3.3%) | 11/106 (10.4%) | 0.29 (0.09–0.95) | 71 fewer per 1,000 (from 5 fewer to 93 fewer) | ⊕⊕ΟΟ |
| Quality of life (2) | Very serious | Not | Not | Serious | None | 32/50 (64%) | 20/50 (40%) | 2.95 (1.25–6.97) | 263 more per 1,000 (from 55 more to 423 more) | ⊕ΟΟΟ |
| Myelosuppression (3) | Very serious | Serious | Not | Serious | None | 14/97 (14.4%) | 19/86 (22.1%) | 0.49 (0.21–1.11) | 99 fewer per 1,000 (from 165 fewer to 18 more) | ⊕ΟΟΟ |
| Neutropenia (2) | Serious | Serious | Not | Serious | None | 7/70 (10%) | 31/66 (47%) | 0.1 (0.02–0.61) | 388 fewer per 1,000 (from 119 fewer to 452 fewer) | ⊕ΟΟΟ |
| Gastrointestinal reaction (5) | Very serious | Not | Not | No | None | 36/167 (21.6%) | 55/152 (36.2%) | 0.35 (0.19–0.66) | 196 fewer per 1,000 (from 90 fewer to 265 fewer) | ⊕⊕ΟΟ |
| Hepatotoxicity (3) | Serious | Not | Not | Serious | None | 15/117 (12.8%) | 22/102 (21.6%) | 0.52 (0.23–1.15) | 91 fewer per 1,000 (from 156 fewer to 25 more) | ⊕⊕ΟΟ |
| Nephrotoxicity (4) | Serious | Not | Not | Serious | None | 7/137 (5.1%) | 11/122 (9%) | 0.56 (0.19–1.59) | 38 fewer per 1,000 (from 72 fewer to 46 more) | ⊕⊕ΟΟ |
| Thoracodynia (4) | Serious | Not | Not | Serious | None | 9/120 (7.5%) | 31/116 (26.7%) | 0.21 (0.1–0.48) | 196 fewer per 1,000 (from 118 fewer to 232 fewer) | ⊕⊕ΟΟ |
| Fever (4) | Serious | Not | Not | Serious | None | 7/147 (4.8%) | 15/132 (11.4%) | 0.41 (0.16–1.07) | 64 fewer per 1,000 (from 94 fewer to 7 more) | ⊕⊕ΟΟ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPleural and Pulmonary Diseases
1 Introduction
The dried root of the shrub Sophora flavescens Aiton (Chinese name: kushen) is an important herbal medicine in China, Japan, Korea, India, and in some of Europe (He et al., 2015;Liang et al., 2019). It contains active components such as matrine, oxymatrine, sophoridine, flavonoids, alkylxanthones, quinones, triterpene glycosides, fatty acids, and essential oils (Cao and He, 2020; Chen et al., 2021; Chen et al., 2022). Its matrine and oxymatrine show significant anti-tumor activities by inhibiting tumor cell proliferation, inducing apoptosis, regulating the tumor microenvironment, and down-regulating cancer-related inflammation (Guo et al., 2015; Ma et al., 2016; Cao and He, 2020; Chen et al., 2021; Chen et al., 2022; Liu et al., 2023). In China, three traditional Chinese medicine injections (TCMIs)—compound kushen injection (CKI), kang’ai, and matrine injection—were developed, with S. flavescens extracts including matrine and oxymatrine as the core components (Supplementary Material S1 and Supplementary Table S1). In this analysis, we defined three types of injection as S. flavescens (kushen) preparations. CKI mainly contains ethanol and water extracts such as matrine, oxymatrine, and sophoridine, which are extracted from S. flavescens Aiton (kushen) and Heterosmilax yunnanensis Gagnep (baituling) (Guo et al., 2015; Ma et al., 2016; Liu et al., 2023). Kang’ai injection contains multiple ingredients including Astragalus polysaccharides, astragalosides, ginsenosides, ginseng polysaccharides, and oxymatrine, which are extracted from kushen, ginseng (Panax ginseng C.A. Mey), and Astragalus membranaceus (Fisch.) Bunge (Fabaceae) (Wan et al., 2018; Sun et al., 2021). Matrine injection is a chemical drug derived from kushen. Clinically, three types of kushen preparations have been approved by the China Food and Drug Administration for adjuvant therapy of solid tumors (Ma et al., 2016; Wang et al., 2016; Li H. et al., 2019; Liu et al., 2022; Liu et al., 2023).
Malignant pleural effusion (MPE), a frequent complication often secondary to metastases to the pleura, originates from intra- or extra-thoracic malignant tumors (Hassan et al., 2021; Gayen, 2022). Patients with MPE often experience progressive breathlessness, tumor progression, and poor survival. Currently, effective control of pleural effusion, improvement of clinical symptoms, and quality of life (QOL) have become the main treatment goals for symptomatic MPE and suspected expandable lung patients (Bibby et al., 2018; Feller-Kopman et al., 2018). Excluding malignant tumors, CKI, kang’ai, and matrine injections are commonly used to control MPE through intrapleural perfusion (Yang et al., 2016; Wu et al., 2018; Li B. et al., 2019; Xu et al., 2022). According to the Cochrane systematic evaluation, five systematic reviews/meta-analyses (SRs/meta-analyses) (Tang et al., 2014; Biaoxue et al., 2015; Xu et al., 2015; Yang et al., 2016; Wu et al., 2018) reported that kushen preparations might increase clinical response rate and improve QOL with a low adverse drug reactions (ADRs) in MPE. But these SRs/meta-analyses (Tang et al., 2014; Biaoxue et al., 2015; Xu et al., 2015; Yang et al., 2016; Wu et al., 2018) exhibited significant clinical heterogeneity, conducted inappropriate data analysis, and involved 16 ineligible studies (Supplementary Tables S3, S4). They also lacked rigorous and reasonable methodologies such as prior planning and systematic retrieval. These deficiencies undermine the credibility of their conclusions, which easily mislead clinical decision-making.
At present, no evaluation has revealed their clinical value for perfusion with kushen preparation alone for MPE. No evidence has confirmed its optimal treatment plan, indications, usage, and how to reasonably apply kushen preparation to achieve expected clinical efficacy and safety. Since the publication of the latest SR/meta-analysis in 2018, (Wu et al., 2018), 23 trials (Supplementary Material S3) have been published (Huang, 2021; Feng and Shi, 2023; Lin et al., 2023; Wang R. et al., 2023). We further performed a registered SR/meta-analysis to verify the therapeutic value of kushen preparations for controlling MPE, reveal their optimal treatment plan, suitable population and usage, and demonstrate their clinical effectiveness and safety. A new evidence framework will be developed for clinical decision-making about the reasonable application of kushen preparations to control MPE and further new research projects.
2 Materials and methods
Kushen preparations mainly include CKI, kang’ai, and matrine. To verify their therapeutic value for controlling MPE, we systematically and comprehensively collected all eligible studies about kushen preparations for controlling MPE (Figure 1). These were clustered into multiple homogeneous and implementable treatment units such as CKI alone, and CKI, kang’ai, or matrine and cisplatin, nedaplatin, or carboplatin. We then further evaluated their methodological quality and pooled the data from each treatment unit and finally summarized and developed an evidence framework for rational drug use decision-making and future research projects. We registered this analysis on PROSPERO (CRD42023430139) and reported all findings according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA 2020 Checklist) (Page et al., 2021). During the retrieval, selection, evaluation of methodological quality, data collection, statistical analysis, and summary of evidence, any disagreements were resolved through discussion with each other or with Zheng Xiao. Ethical approval was not required as the materials were published studies.
Implementation framework.
2.1 Inclusion and exclusion criteria
According to the PICOS model, we established the following criteria for all eligible studies to meet.
- (i). Only optimum trials as randomized controlled trials (RCTs) without restrictions on follow-up, institutions, language, and publication time.
- (ii). All patients presented with MPE and dyspnea which was diagnosed by thorax imaging, pleural fluid analysis, cytology, or pleural biopsy. All patients had normal liver, kidney, and heart function, and no limitations on tumor type and pleural fluid volume.
- (iii). The interventions were kushen preparations such as CKI, kang’ai, and matrine injection through intrapleural perfusion. Both groups did not receive any intrapleural perfusion 1 month before treatment. The experimental groups received kushen preparation alone or in combination with other sclerosants, and the controls received sclerosants alone such as chemical drugs, biological response modifiers (BRMs), or TCMI.
- (iv). The main outcomes are clinical response and survival, and secondary outcomes are QOL and adverse events.
All ineligible studies must meet the following criteria: studies about patients with ascites or pericardial effusion; all patients receiving systemic chemotherapy, local hyperthermia or oral traditional Chinese medicine (TCM); both groups receiving kushen preparation; studies with unclear objectives; without any data about clinical responses, survivals, QOL, or adverse events.
2.2 Outcomes definition
The primary outcomes are clinical response and survival. Referring to previous studies (Paladine et al., 1976; Kessinger and Wigton, 1987; Keeratichananont et al., 2015; Jie Wang et al., 2018; Dipper et al., 2020; Xiao et al., 2020a), we integrated both Millar and Ostrowskimj criteria to measure the clinical responses as: (i) complete response (CR) is the disappearance of pleural effusion for more than 30 days, or the lack of accumulation of fluid; (ii) partial response (PR) is less than 50% reduction of pleural effusion for more than 30 days; (iii) no response (NR)/stable disease (SD) is less than 50% reduction of pleural effusion or less than 25% increase or the recurrence of fluid accumulation without further therapy; (iv) pleural progression (PP) is more than 25% increase of pleural effusion or symptomatic fluid accumulation again requiring further therapy. We set the pleurodesis failure as no response or stable disease plus pleural progression and assessed the clinical responses using complete response, pleurodesis failure, and pleural progression (Supplementary Material S2). Long-term survival was assessed by using overall survival (OS), progression-free survival (PFS), OS, and PFS rates. According to the Karnofsky performance status (KPS) scale, when a KPS score increased ≥10 after treatment, QOL was improved.
Adverse events (AEs) were assessed by using ADRs and thoracentesis-related adverse events (TRAEs). According to World Health Organization (WHO) or Common Terminology Criteria for Adverse Events (CTCAEs) criteria (Miller et al., 1981; Trotti et al., 2003), ADRs were measured by using the indicators myelosuppression, neutropenia, thrombocytopenia, anemia, hepatorenal toxicity, gastrointestinal reactions, thoracodynia, and fever. TRAEs were measured by using indicators including treatment-related death, respiratory failure, dyspnea, pneumothorax, chest infection, drainage tube detachment, tumor metastasis along the indwelling duct, catheter-related infection, or subcutaneous emphysema.
2.3 Retrieval and selection strategies
Adhering to a retrieval logic of patient plus intervention, we customized the retrieval strategies for each database using MeSH and free words (Supplementary Material S3). Yan Zhang and Hui Liu independently searched all related studies about “Kushen preparations in controlling MPE” from Chinese and English electronic databases (to February 2025) including the Guizhou Digital Library, SinoMed, China National Knowledge Infrastructure Database, WanFang Database, Chinese Scientific Journals Full-text Database, PubMed, Embase, Web of Science, and Cochrane Central Register of Controlled Trials (Issue 2, February 2025). We collected ongoing trials from the Chinese Clinical Trial Registry (http://www.chictr.org.cn), WHO International Clinical Trials Registry Platform (http://apps.who.int/trialsearch/), and US clinical trials (https://clinicaltrials.gov). Finally, we also identified eligible studies from the references of relevant SRs or network meta-analysis. Hui Liu and Yan Zhang independently selected eligibles and excluded ineligible studies following a predesigned inclusion and exclusion criteria.
2.4 Assessment of methodological quality
For clinical responses, survivals, QOL, or adverse events, Da-chun Cai and Jiao Xu independently applied a revised Cochrane tool (RoB 2) to assess methodological quality arising from five domains: randomization process (D1), intended interventions (D2), missing outcome data (D3), outcomes measurement (D4), and selective reporting of results (D5) (Sterne et al., 2019; Higgins et al., 2021). We judged each quality based on the domain algorithm and made an overall judgment.
2.5 Data collection
Yao-Qin Luo and Da-chun Cai independently collected all data using a predesigned data extraction form. The data were first author, time of publication, methodological features, demographic characteristics and cases; characteristics of patients as tumor types, pleural fluid volume, anticipated survival time (AST), KPS score, treatment history, and recurrence; drainage methods as indwelling pleural catheters (IPCs) or thoracentesis; kushen preparations, treatment dose, frequency and times, and sclerosants and uses; follow-up protocol, research institutions, criterion and time of evaluation. The outcomes were: complete response, pleurodesis failure, pleural progression, PFS, OS, QOL, ADRs, and TRAEs. Additionally, the authors of papers were contacted about available survival data. If they were unavailable, the Kaplan–Meier survival curves were transformed into data using Engauge Digitizer 4.1 (Guyot et al., 2012; Xiao et al., 2018).
2.6 Statistical analysis
All eligible studies were clustered into multiple homogeneous treatment units, and we further analyzed their clinical effectiveness and safety. The odds ratios (ORs) and their 95% confidence interval (CI) were applied to measure the complete response, pleurodesis failure, pleural progression, OS rate, QOL, ADRs, and TRAEs, with p < 0.05 being identified as statistically significant. Cochran’s χ^2^ test and I ^2^ statistic were performed to identify statistical heterogeneity among each unit. If the results showed significant heterogeneity and inconsistent directions or involved a single trial, we used forest plots to describe the result. When p ≥ 0.1 and I ^2^ ≤ 50%, a fixed-effects model (FEM) was applied to pool the OR and their 95% CI. When p < 0.1, I ^2^ > 50%, and the results had consistent direction, a random-effects model (REM) was applied. Yan Zhang and Feng Luo independently applied Review Manager 5.4 to pool the data from each unit. If the outcomes involved more than ten trials, a funnel plot and Egger’s test (STATA V.15.0 software, 401506209499) were applied to identify potential publication bias.
Referring to previous experience (Xiao et al., 2020b; Wang et al., 2021; Wang et al., 2022; Wang C. Q. et al., 2023), a subgroup analysis was implemented to reveal the potential clinical heterogeneity among the main treatment plans with enough trials to analyze the effects of patient related factors, interventions, and evaluation criteria on clinical responses and to further identify the suitable population and optimum usage. We further implemented univariate random effects meta-regression analysis to reveal the correlation between each factor and clinical responses and post hoc multiple regression analysis to identify it.
Following underestimation of effectiveness/safety, we implemented sensitivity analysis to identify robustness (Xiao et al., 2020b; Wang et al., 2021; Wang et al., 2022; Wang C. Q. et al., 2023). The consistency of results before and after excluding both trials with high risk and overestimation were analyzed. If consistency was good, the result was robust; otherwise, it was poor. To identify the required information size (RIS) for the results of main treatment units (Thorlund et al., 2016), we further applied Trial Sequential Analysis (TSA) software (version 0.9.5.10 Beta) to implement the analysis. In the light of previous experience, we set the risk of type I error as 5% with a power of 80%, relative risk reduction (RRR) as 25% for clinical responses and QOL, and 20% for adverse events (AEs) (Wetterslev et al., 2008; Thorlund et al., 2009). We used control event rates from this analysis for these calculation, and adjusted the information size for diversity (Wetterslev et al., 2009).
2.7 Summary of evidence quality
We integrated the results of sensitivity analysis into the GRADE approach (Guyatt et al., 2008; Xiao et al., 2020b; Wang et al., 2021; Wang et al., 2022; Wang C. Q. et al., 2023) and developed a revised approach to summarize the evidence. Quality was identified as “high”, moderate”, “low”, and “very low” following five domains: risk-of-bias of results, heterogeneity, indirectness, imprecision, and publication bias (Supplementary Material S2). Jun Huang and Yan-Yan Jin independently applied the GRADE profiler to summarize the evidence quality and generated the absolute estimates of effect for outcomes.
3 Results
3.1 Search results
After retrieval, 1,269 records were identified. Two reviewers read the titles, excluded duplicates, and identified 443 records. After screening abstracts and excluding irrelevant and non RCTs, 147 RCTs, six SRs/meta-analyses (Tian et al., 2010; Tang et al., 2014; Biaoxue et al., 2015; Xu et al., 2015; Yang et al., 2016; Wu et al., 2018) and four network meta-analyses (Yang et al., 2017; Li B. et al., 2019; Li, 2022; Xu et al., 2022) were selected. Further evaluating full-texts and excluding 64 ineligible studies (Supplementary Material S3), 83 were considered eligible. Additionally, 42 studies were selected from previous studies. Finally excluding duplicates, 83 eligible studies were selected for this analysis (Figure 2).
PRISMA 2020 flow diagram for selecting eligible studies.
3.2 Characteristics of included studies
We clustered the 83 eligible studies from 2001 to 2023 into four themes: intrapleural perfusion with CKI alone, CKI and sclerosants, kang’ai or matrine, and platinum for controlling MPE. Eleven trials reported CKI alone (Table 1a). CKI and sclerosant developed three comparisons as CKI-versus-cisplatin (Yuan, 2007; Hu Q. et al., 2008; Chen, 2010; Liang et al., 2011; Chen, 2013; Xing, 2013; Wang and Zhou, 2016; Yan et al., 2016; Wang R. et al., 2023), mitomycin (Zhang, 2011), or interleukin-2 (Huang, 2013). All trials recruited 796 inpatients—426 male and 244 female patients aged 20–82 years. Receiving CKI were 396 patients, while another 400 received sclerosants alone. Perfusion with CKI and sclerosants was reported in 59 trials (Table 1b). The CKI and chemical drug or BRM developed ten treatment plans: perfusion with CKI and cisplatin, nedaplatin (Li, 2014; Zhang S. et al., 2015; Li et al., 2017), bleomycin (Chen and He, 2003; Liu and Wan, 2011; Sun, 2012), hydroxycamptothecin (He et al., 2009; Wu et al., 2014; Cai and Wang, 2019), lobaplatin (Liu and Xu, 2016; Huang, 2021), carboplatin (He and Xie, 2010), mitomycin (Zhang et al., 2013), interleukin-2 (Hao and Liang, 2007; Zhou et al., 2010), OK-432 (Wei et al., 2014; Zhong et al., 2015), and Corynebacterium parvum (Huang et al., 2012). There were 41 trials which evaluated perfusion with CKI and cisplatin, recruiting 2,823 inpatients aged 15–91, with 1,346 male and 909 female patients. Some 1,424 patients received perfusion with CKI and cisplatin, while another 1,399 received cisplatin alone. CKI was administrated 10–60 mL/time, once to thrice per week, lasting one to twelve times; the cisplatin was administrated with 20–80 mg/time. Kang’ai or matrine and platinum developed four plans. Six trials involving 334 inpatients aged 36–84 years (Zhang, 2006; Hu J. et al., 2008; Xu and Xiong, 2008; He, 2011; Qu et al., 2012; Wang, 2016) evaluated perfusion with kang’ai and cisplatin (Table 1c). Received kang’ai and cisplatin were 168 patients, while another 166 received only cisplatin. Kang’ai was administrated 40–60 mL/time, once or twice per week, lasting one to four times. Six trials recruiting 319 inpatients aged 30–85 (Du et al., 2009; Li and Yang, 2009; He, 2010; Wang et al., 2010; Ji, 2011; Ji et al., 2012) evaluated perfusion with matrine and cisplatin (Table 1d). A total of 167 patients received matrine and cisplatin, while another 152 only received cisplatin. Matrine was administrated 150–800 mg/time, once a week, lasting 2 to 6 weeks.
Of 83 eligible studies, 58 (69.88%, 58/83) involved inpatients with miscellaneous tumors, 24 (28.92%, 24/83) with lung cancer, and only one with hematologic malignancies (Huang, 2013) or breast cancer (Wang R. et al., 2023). Most studies described demographic characteristics, but only 16 to 50 (19.28%, 16/83% to 60.24%, 50/83) reported the pleural fluid volume, KPS, AST, and treatment history. All studies reported the drainage methods and characteristics of interventions and assessed the clinical responses 5–10 weeks after treatment began using Ostrowskimj or Millar criteria. Only 36 studies (43.37%, 36/83) reported the QOL, and six reported overall survival (Cui et al., 2008; Chen, 2010; He, 2011; Han, 2013; Zhang S. et al., 2015). Some 79 studies (95.18%, 79/83) reported the AEs, 38 (45.78%, 38/83) assessed ADRs using WHO or CTEC3.0 criteria, and only four assessed TRAEs (Wang et al., 2010; Yang, 2012; Wei et al., 2014; Liu and Li, 2015; Song and Jia, 2015). No study reported conflicts of interest.
3.3 Methodological quality
Of 83 studies, 79 (95.18%, 79/83) expressed concerns at overall bias for clinical responses, and four showed high risk (Qu et al., 2012; Wu et al., 2014; Wang and Zhou, 2016; Lin et al., 2023). At domain-level, only one study had low risk at D1 (Liu and Li, 2015), one showed high risk at D1 (Lin et al., 2023) or D2 (Wang and Zhou, 2016), and others had some concerns. All had low risk at D3 and D4. Two studies showed high risk at D5 (Qu et al., 2012; Wu et al., 2014), and others had low risk (Figure 3A; Supplementary Figures S1, S2). For overall survival, five studies had concerns of overall bias (Cui et al., 2008; Chen, 2010; He, 2011; Han, 2013; Zhang S. et al., 2015). All had some concerns at D1 and D2, and low risk at D3, D4, and D5 (Supplementary Figure S4).
Risk-of-bias of compound kushen injection and cisplatin. (a) Clinical responses; (b) quality of life; (c) adverse events.
Since studies were limited, we only assessed the methodological quality of QOL and adverse events in CKI versus cisplatin, and perfusion with CKI, kang’ai, or matrine and cisplatin. QOL was reported by 29 studies and showed high risk at overall bias. Only one study (Liu and Li, 2015) had low risk, and one (Lin et al., 2023) had high risk at D1. All showed some concern at D2, low risk at D3 and D5, and high risk at D4 (Figure 3B and S3). A total of 57 studies reported AEs, 35 (61.40%, 35/57) showed high risk at overall bias, and 21 had some concerns. There were 55 studies (96.49%, 55/57) with some concerns at D1and D2, two with low risk at D1 (Liu and Li, 2015; Lin et al., 2023), and one with high risk at D2 (Wang and Zhou, 2016). All studies had low risk at D3. High risk was shown by 16 studies (28.07%, 16/57), and 39 had low risk at D4. A total of 34 studies (59.65%, 34/57) showed high risk, and 21 had low risk at D5 (Figure 3C and Figure. S5).
3.4 Clinical responses
Nine trials reported clinical responses about CKI versus cisplatin (Table 2a; Supplementary Figures S6–S8). Cochran’s χ^2^ test and I ^2^ statistic revealed no heterogeneity (I ^2^ = 0%). We pooled the OR using a FEM. The results of meta-analyses revealed that CKI perfusion displayed a complete response (1.10, 95% CI 0.76 to 1.60), pleurodesis failure (0.80, 95% CI 0.56 to 1.14), and pleural progression (0.63, 95% CI 0.33 to 1.21) similar to cisplatin alone. Only single trial reported that CKI achieved clinical response similar to mitomycin and better than interleukin-2.
The CKI and chemical drug or BRM developed ten treatment plans (Table 2b; Figure 4C; Figure 5). Perfusion with CKI and cisplatin was evaluated by 41 trials. With no statistical heterogeneity (I ^2^ = 0%), an FEM was used to pool the OR. The results demonstrated it significantly improving the complete response (2.71, 95% CI 2.30 to 3.19) and displaying a low pleurodesis failure (0.26, 95% CI 0.22 to 0.32) and pleural progression (0.22, 95% CI 0.14–0.36) than cisplatin alone. One to three trials reported nine other treatment plans. Compared with sclerosants alone, the results revealed that nine treatment plans achieved a low pleurodesis failure, while only CKI and bleomycin, hydroxycamptothecin, or interleukin-2 significantly improved the complete response.
Clinical responses of compound kushen injection in MPE. (A) Meta-analysis of complete response; (B) meta-analysis of pleurodesis failure; (C) forest plot of pleural progression.
Forest plot of overall survivals.
Kang’ai or matrine and platinum developed four treatment plans (Table 2c, 2d; Supplementary Figures S9–S11). With no statistical heterogeneity (I ^2^ = 0%), an FEM was used. The results demonstrated that perfusion with kang’ai or matrine and cisplatin significantly improved the complete response (3.04, 95% CI 1.76 to 5.26 and 1.87, 95% CI 1.26–2.78) and achieved a low pleurodesis failure (0.23, 95% CI 0.14 to 0.41 and 0.27, 95% CI 0.17–0.44) than cisplatin alone. Additionally, matrine and cisplatin achieved a low pleural progression (0.29, 95% CI 0.09–0.95).
3.5 Overall survivals
Of 83 studies, only six (Cui et al., 2008; Chen, 2010; Chen et al., 2011; He, 2011; Han, 2013; Zhang S. et al., 2015) reported the OS of perfusion with CKI alone, CKI and cisplatin or nedaplatin, kang’ai and cisplatin, or matrine and carboplatin (Figure 5). Compared with sclerosants alone, only one trial reported that perfusion with CKI and cisplatin might improve the 0.5-year OS rate (Han, 2013), and it might prolong median survival time and PFS (Chen et al., 2011). Perfusion with CKI and nedaplatin might improve the 1-year OS rate (Zhang S. et al., 2015), and matrine and carboplatin might improve the 0.5-year, 1-year, and 1.5-year OS rates (Cui et al., 2008).
3.6 Quality of life
Due to limited trials, we only assessed the QOL of perfusion with CKI alone, CKI, kang’ai, or matrine and cisplatin (Table 3; Supplementary Figures S12, S13). Six trials reported the QOL about CKI alone (Yuan, 2007; Hu Q. et al., 2008; Liang et al., 2011; Chen, 2013; Xing, 2013; Yan et al., 2016). Statistical heterogeneity (I ^2^ = 67%) was found, and an REM was used. Compared with cisplatin alone, CKI perfusion acquired a similar QOL. There were 21 trials reporting QOL about perfusion with CKI, kang’ai, or matrine and cisplatin. No heterogeneity was found (I ^2^ = 0%), and an FEM was used to pool the OR. Compared with cisplatin alone, the results demonstrated that perfusion with CKI, kang’ai or matrine and cisplatin significantly improved QOL (3.60, 95% CI 2.84 to 4.56; 3.95, 95% CI 1.78 to 8.74 and 2.95, 95% CI 1.25–6.97).
3.7 Adverse events
Nine trials reported eight AEs about CKI alone (Table 3a; Supplementary Figures S14, S15, S18–S23). Cochran’s χ^2^ test and I ^2^ statistic only identified statistical heterogeneity for myelosuppression (I^2^ = 69%), gastrointestinal reaction (I^2^ = 67%), thoracodynia (I^2^ = 69%), and fever (I^2^ = 81%), and an REM or FEM was used to synthesize the OR. Compared with cisplatin alone, meta-analysis revealed that perfusion with CKI alone showed a low myelosuppression (0.02, 95% CI 0.00 to 0.15), leukopenia (0.10, 95% CI 0.03–0.35), gastrointestinal reaction (0.03, 95% CI 0.01 to 0.12), hepatotoxicity (0.09, 95% 0.02–0.33), nephrotoxicity (0.09, 95% CI 0.03 to 0.29), and thoracodynia (0.15, 95% CI 0.04 to 0.48).
Ten AEs were reported by 38 trials about CKI and cisplatin (Table 3; Supplementary Figures S14–S23). We only identified minimal heterogeneity for gastrointestinal reaction (I^2^ = 8%), and an FEM was used. The results demonstrated that perfusion with CKI and cisplatin showed a low myelosuppression (0.34, 95% CI 0.24–0.47), neutropenia (0.35, 95% CI 0.26 to 0.46), gastrointestinal reaction (0.36, 95% CI 0.29–0.44), and hepatorenal toxicity (0.42, 95% CI 0.28 to 0.63 and 0.32, 95% CI 0.24–0.44) and fever (0.50, 95% CI 0.30–0.82).
Five trials reported six AEs to kang’ai and cisplatin (Table 3c; Supplementary Figures S15–S24). We only identified minimal heterogeneity leukopenia (I ^2^ = 25%), and an FEM was used. The results revealed that kang’ai and cisplatin showed low neutropenia (OR = 0.20, 95% CI 0.11–0.38) and gastrointestinal reaction (OR = 0.34, 95% CI 0.19–0.63).
Five trials reported ten AEs to matrine and cisplatin (Table 3d; Supplementary Figures S14–S23). We only identified statistical heterogeneity for neutropenia (I ^2^ = 66%) and minimal heterogeneity for myelosuppression (I ^2^ = 43%), and an REM or FEM was used. The results revealed that matrine and cisplatin showed low neutropenia (0.10, 95% CI 0.02–0.61), gastrointestinal reaction (0.35, 95% CI 0.19–0.66), and thoracodynia (0.21, 95% CI 0.10–0.48).
3.8 Subgroup analysis
In targeting perfusion with CKI and cisplatin, subgroup analysis revealed that under different primary tumors, drainage, and evaluation criteria, this treatment plan obtained significant improvement in the complete response and low pleurodesis failure. For patients with moderate-to-large effusion, KPS ≥50 to ≥70 scores, AST ≥3 months, or primary treatment, it significantly improved clinical responses. Perfusion with CKI (20–50 mL/time, once per week, two to four times) and cisplatin (20–80 mg/time) could significantly improve the clinical responses. Moreover, perfusion with low-dosage cisplatin and CKI could obtain clinical responses like high-dosage. However, the univariate regression and multiple meta-regression analysis did not reveal any correlation between clinical response and each variable (Table 4; Supplementary Figures S25–S72).
3.9 Publication bias analysis
Only perfusion with CKI and cisplatin was included in more than ten trials (Table 5; Supplementary Figures S73–S83). The funnel plot and Egger’s test did not identify publication bias for the complete response, pleurodesis failure, pleural progression, myelosuppression, neutropenia, hepatorenal toxicity, thoracodynia, and fever, which were objectively reported. Significant publication bias was identified for QOL (coefficient = –2.47, 95% CI –4.62 to –0.32) and gastrointestinal reaction (coefficient = –1.49, 5% CI –2.71 to –0.21); both results were under-estimated.
3.10 Sensitivity analysis
In CKI versus cisplatin, 11 outcomes were pooled using meta-analysis. Before and after excluding the trials with high risk and over-estimating efficacy/safety, the OR of QOL, myelosuppression, gastrointestinal reaction, and thoracodynia showed poor robustness, and the others had good robustness. In perfusion with CKI and cisplatin, 13 outcomes were pooled, and QOL, thrombocytopenia and anemia showed poor robustness. In CKI and nedaplatin, lobaplatin, bleomycin, hydroxycamptothecin, interleukin-2, or OK-432, 12 outcomes were pooled, and only the complete response of CKI and nedaplatin, lobaplatin, or OK-432 showed good robustness. In kang’ai and cisplatin, six outcomes were pooled, showing poor robustness. In matrine and cisplatin, 11 outcomes were pooled, and the QOL, myelosuppression, neutropenia, and gastrointestinal reaction showed poor robustness (Table 6).
3.11 Trial sequential analyses
Since the trials were limited, we only assessed the RIS for clinical responses in CKI versus cisplatin. The TSA identified firm information size for supporting a similar complete response and pleurodesis failure between CKI and cisplatin, and no reliable information for pleural progression. We further assessed the RIS for clinical responses, QOL, and AEs in perfusion with CKI and cisplatin. Further analysis identified sufficient and conclusive information sizes for complete response, pleurodesis failure, QOL, neutropenia, and gastrointestinal reaction, and firm information for pleural progression, myelosuppression, and hepatorenal toxicity. Finally, we only assessed the RIS for clinical responses in kang’ai or matrine and cisplatin. The analysis identified firm information sizes for pleurodesis failure in both treatments and no reliable information for complete response (Table.7; Figure 6; Supplementary Figures S84–S94).
Trial sequential analyses in compound kushen injection and cisplatin. (a) Complete response; (b) pleurodesis failure; (c) pleural progression; (d) quality of life; (e) neutropenia; (f) gastrointestinal reaction.
3.12 Evidence quality
We applied a revised GRADE approach to identify the evidence quality as “high”, “moderate”, “low”, and “very low”. In CKI versus cisplatin, 11 results were pooled. Clinical responses, hepatorenal toxicity, and fever were summarized as moderate quality, while other five results were low to very low (Table 8a). In perfusion with CKI and cisplatin, 13 results were pooled. Clinical responses, myelosuppression, neutropenia, gastrointestinal reaction, hepatorenal toxicity, and fever were summarized as moderate, while the other four were low to very low. In CKI and nedaplatin, lobaplatin, bleomycin, hydroxycamptothecin, interleukin-2, or OK-432, 12 results were pooled. The clinical responses were very low to low (Table 8b). In kang’ai and cisplatin, six results were pooled at low to very low (Table 8c). In matrine and cisplatin, 11 results were pooled. The complete response and pleurodesis failure were summarized as moderate, with the other nine results as low to very low (Table 8d).
4 Discussion
After integrating previous six SRs/meta-analyses (Tian et al., 2010; Tang et al., 2014; Biaoxue et al., 2015; Xu et al., 2015; Yang et al., 2016; Wu et al., 2018) and four network meta-analyses (Yang et al., 2017; Li B. et al., 2019; Li, 2022; Xu et al., 2022), we collected 83 RCTs for analysis and supplemented 39 trials in previous studies. We found three kushen preparations—CKI, kang’ai and matrine injection—which were administrated for controlling MPE through intrapleural perfusion. For kushen preparation alone, nine trials evaluated perfusion with CKI versus cisplatin alone. CKI mainly contains matrine, oxymatrine, and sophoridine, which have significant anti-tumor activity, regulate tumor microenvironment, and downregulate tumor-associated inflammation (Guo et al., 2015; Ma et al., 2016; Cao and He, 2020; Chen et al., 2021; Chen et al., 2022; Liu et al., 2023). The meta-analysis results demonstrated that perfusion with CKI alone showed clinical responses similar to cisplatin and a lower hepatorenal toxicity (Figure 7). These results were of moderate quality following the revised GRADE approach (Wang et al., 2022; Wang C. Q. et al., 2023), and the TSA found firm information sizes for supporting them. CKI perfusion showed low hematotoxicity, gastrointestinal reaction, and thoracodynia of low to very low quality. Zhang Z. et al. (2015), Zhong et al. (2015), Zhu and Hou (2021), Fan et al. (2022); Feng and Shi (2023) reported that CKI perfusion might prevent pleural effusion recurrence by downregulating the vascular endothelial cell growth factor and reducing angiogenesis. In all, these results suggest that CKI may serve as a new palliative intervention for MPE. Clinically, CKI, kang’ai, and matrine injections have been widely used as an adjuvant therapy for various solid tumors (Ma et al., 2016; Wang et al., 2016; Li H. et al., 2019; Liu et al., 2022; Liu et al., 2023). Apparently, this analysis further revealed a new therapeutic value and clinical application population of CKI. Unfortunately, no evidence supports the possibility of using kang’ai and matrine alone to treat MPE, which requires new trials to investigate.
Evidence framework of kushen preparations for MPE.
Clinically, CKI is often combined with other sclerosants to control MPE through intrapleural perfusion. We found that CKI combined with seven chemical drugs or three BRMs to build ten homogenous treatment plans. The clinical values of perfusion with CKI and cisplatin have been reported by 41 trials. Compared with cisplatin alone, the results of meta-analyses demonstrated that perfusion with CKI and cisplatin significantly improved complete response and QOL with a low pleurodesis failure and pleural progression, and showed a low incidence rate of hematotoxicity, gastrointestinal reaction, and hepatorenal toxicity. Excluding QOL, these results were moderate quality following the revised GRADE approach (Wang et al., 2022; Wang C. Q. et al., 2023). The results of pleural progression, myelosuppression, and hepatorenal toxicity had firm information in support, while other results obtained sufficient and conclusive information support. In all, these results demonstrate that CKI infusion can improve clinical responses and QOL and reduce ADRs. Like high dosage, the subgroup analysis revealed that CKI combined with low-dosage cisplatin also obtained similar clinical responses. These results indicate that CKI and cisplatin have cooperative effect, and CKI may reduce cisplatin dosage while ensuring similar clinical benefits. Previous SR/meta-analyses have reported that as important BRMs, staphylococcal enterotoxin C (Jiang et al., 2022) and mannatide (Zhang et al., 2011; Chen et al., 2013) perfusion showed a high risk of fever. In this analysis, we found that perfusion with CKI might reduce the risk of fever. This finding may be the unique value of CKI in controlling MPE. The results of meta-analysis of other nine treatment plans further revealed that perfusion with CKI and lobaplatin, nedaplatin, bleomycin, hydroxycamptothecin, interleukin-2, or OK-432 might also improve clinical responses. However, the results had very low to low quality and lacked sufficient or firm information sizes in support. Comprehensively examining both information sizes and methodological quality, we conclude that among ten treatment plans, perfusion with CKI and cisplatin may be an optimal treatment plan for MPE, which shows significant improvement in clinical responses and low incidence of ADRs, especially fever (Figure 7). Further subgroup analysis revealed that perfusion with CKI (20–50 mL each time, once a week lasting two to four times) and cisplatin (20–80 mg each time) could obtain ideal clinical responses for MPE inpatients with moderate to large effusion, KPS ≥50 to ≥70 scores, AST ≥3 months, or primary treatment. Furthermore, the primary tumor, drainages or evaluation criteria showed no negative effect on clinical responses. These results suggest that inpatients with moderate-to-large effusion, KPS ≥ 50 to ≥ 70 scores, AST ≥ 3 months, or primary treatment are a possible suitable population. The CKI with 20 to 50 ml each time, once a week lasting two to four times and cisplatin with 20 to 80 mg each perfusion may be an optimal usage for obtaining desired responses and safety (Figure 7). Unfortunately, both meta-regression analyses did not find any correlation. These results require new evidence for confirmation.
Matrine and kang’ai are also important kushen preparations. Kang’ai mainly contains Astragalus polysaccharides, astragalosides, ginsenosides, ginseng polysaccharides, and oxymatrine (Wan et al., 2018; Sun et al., 2021). Six trials each evaluated the clinical benefit of perfusion with kang’ai or matrine and cisplatin (Zhang, 2006; Hu J. et al., 2008; Xu and Xiong, 2008; He, 2011; Qu et al., 2012; Wang, 2016). The meta-analysis results showed that perfusion with kang’ai and cisplatin significantly improved the complete response and QOL with low pleurodesis failure. Matrine is a principal active ingredient of CKI and kang’ai. The results further demonstrated that matrine and cisplatin could improve complete response and QOL with low pleurodesis failure and pleural progression. These results provide a theoretical basis for the clinical value of kang’ai or CKI in MPE. Perfusion with kang’ai or matrine and cisplatin all showed low neutropenia and gastrointestinal reaction. However, only the pleurodesis failure of both treatment plans had a firm quantity of information in support, and no reliable information indicated that both can improve the complete response. For matrine and cisplatin, the complete response and pleurodesis failure had moderate quality, while other results were low to very low. Overall, these results suggest that kang’ai or matrine may be potentially valuable alternative interventions which may improve clinical responses with firm information size (Figure 7). Further rigorous trials will be needed to reveal their clinical significance, suitable population, and optimal usage.
Kushen preparations alone or plus chemical drugs or BRMs form rich treatment plans. To validate their therapeutic value for MPE, we applied clustering SR/meta-analysis, successfully addressing clinical heterogeneity and revealing their clinical efficacy and safety based on homogeneous treatment units. First, we found that CKI may serve as a new palliative intervention for MPE. This analysis confirmed the clinical possibility of using CKI perfusion to control MPE and further revealed its new therapeutic value and clinical application population. Second, among ten treatment plans, we found that perfusion with CKI and cisplatin may be an optimal treatment plan for MPE. Subgroup analysis results further provide a suitable population and optimal use for perfusion with CKI and cisplatin treating MPE. Third, we found that kang’ai or matrine may be potential valuable alternative interventions for MPE. In all, this analysis confirms and reveals the therapeutic value and clinical application population for using kushen preparations to control MPE. These findings will be beneficial for developing rational medication strategies based on kushen preparations to improve clinical benefits and reduce ADRs and medication costs in MPE.
There were some limitations to this new SR/meta-analysis. This analysis customized its retrieval strategies and retrieved both Chinese and English databases, which may exhibit potential bias risk. Among 14 treatment plans, most—like perfusion with CKI, kang’ai, or matrine and other sclerosants—only had limited trials reporting their clinical benefit. In particular, only single trials reported the clinical benefit between CKI and interleukin-2 (Huang, 2013) or mitomycin (Zhang, 2011), as well as perfusion with CKI and carboplatin (He and Xie, 2010), mitomycin (Zhang et al., 2013), or corynebacterium parvum (Huang et al., 2012). Most treatment plans lacked reliable information support, and their results were low to very low quality. Obviously, their clinical effectiveness, safety, indications, and optimal usage still require more high-quality evidence and sufficient information to confirm them. Regarding methodological quality, most studies had some concerns at overall bias about clinical response and overall survival. For both outcomes, D1 and D2 had some concerns.
QOL about perfusion with CKI alone were reported by 29 studies, and CKI, kang’ai, or matrine and cisplatin. All had high risk of overall bias, and D4 was a high-risk domain. AEs were reported by 57 studies. High risk of overall bias was evident in 35 studies, with D4 and D5 as high-risk domains. Such findings suggest that strengthening random allocation, concealment, and blinding methods, and emphasizing the measurement and complete report of indicators will become key issues for improving methodological quality in future trials. Regarding PICO features, most studies did not clearly report patient characteristics such as pleural fluid volume, KPS, AST, or treatment history. Most studies failed to clearly report the TRAEs. Six studies reported overall survival (Cui et al., 2008; Chen, 2010; He, 2011; Han, 2013; Zhang S. et al., 2015). Only single study reported that perfusion with CKI and cisplatin (Chen et al., 2011; Han, 2013) or nedaplatin (Zhang S. et al., 2015) and matrine and carboplatin (Cui et al., 2008) might improve overall survival or progression-free survival. Additionally, no evidence reported recurrence and hospitalization time or conflicts of interest. Such shortcomings of PICO are important issues for design and quality improvement in future trials.
5 Conclusion
Current moderate evidence demonstrates that CKI may be an effective palliative intervention for controlling MPE. Perfusion with CKI and cisplatin may be an optimal treatment plan which can improve clinical responses and QOL and reduce ADRs, especially fever. This analysis further confirms a suitable population and optimal usage for CKI and cisplatin perfusion. CKI, kang’ai, or matrine and chemical drugs or BRMs formed rich treatment plans for MPE. More rigorous trials with low-risk and standardized PICOs will be needed to reveal their clinical significance, suitable populations, and optimal usage.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Biaoxue R. Shuxia M. Wenlong G. Shuanying Y. (2015). Thoracic perfusion of matrine as an adjuvant treatment improves the control of the malignant pleural effusions. World J. Surg. Oncol. 13, 329. 10.1186/s 12957-015-0729-9 26631104 PMC 4668654 · doi ↗ · pubmed ↗
- 2Bibby A. C. Dorn P. Psallidas I. Porcel J. M. Janssen J. Froudarakis M. (2018). ERS/EACTS statement on the management of malignant pleural effusions. Eur. Respir. J. 52, 1800349. 10.1183/13993003.00349-2018 30054348 · doi ↗ · pubmed ↗
- 3Cai H. Wang Q. (2019). Effect of Compound Kushen Injection on elderly patients with lung cancer complicated with malignant pleural effusion. Contemp. Med. Symp. 17, 161–162.
- 4Cao X. He Q. (2020). Anti-tumor activities of bioactive phytochemicals in Sophora flavescens for breast cancer. Cancer Manag. Res. 12, 1457–1467. 10.2147/CMAR.S 243127 32161498 PMC 7051174 · doi ↗ · pubmed ↗
- 5Chen B. Xu X.-M. Yu T.-T. Yang J. (2013). Meta analysis of Lifein combined with Cisplatin in chest catheterization perfusion chemotheapy for malignant pleural effusion. Med J Wuhan Univ 34, 755–761. 10.14188/j.1671-8852.2013.05.039 · doi ↗
- 6Chen F. Liao D. (2012). Clinical observation of compound Kushen injection combined with cisplatin on malignant pleural effusion. World Health Dig. 9, 49–50. 10.3969/j.issn.1672-5085.2012.42.039 · doi ↗
- 7Chen F. Pan Y. Xu J. Liu B. Song H. (2022). Research progress of matrine's anticancer activity and its molecular mechanism. J. Ethnopharmacol. 286, 114914. 10.1016/j.jep.2021.114914 34919987 · doi ↗ · pubmed ↗
- 8Chen L. (2013). Effect of compound matrine injection on malignant pleural effusion. Chin. J. New Drugs 22, 2069–2070+2074.