In Which Scenarios Do Preceptors and Students Agree, Disagree, or Remain Neutral About Learner Mistreatment?
Alejandra Colón-López, Anne Zinski

TL;DR
Medical students and preceptors often disagree on what counts as mistreatment, which could affect how mistreatment is reported and addressed in training.
Contribution
This study compares students’ and preceptors’ perceptions of learner mistreatment using vignettes, revealing discrepancies in their evaluations.
Findings
Students and preceptors agreed on 12 of 17 vignettes regarding learner mistreatment.
Students more often viewed public embarrassment as mistreatment, while preceptors emphasized terms of endearment and career-based denial of training.
Preceptors were more likely to select neutral responses compared to students across most vignettes.
Abstract
In recent years, nearly half of graduating medical students in the USA and Canada reported personal mistreatment experiences during training. Prior scholarship reports heterogeneous opinions of learner mistreatment behaviors among trainees, and resulting unaligned perceptions may influence reporting, feedback, and policy. However, fewer studies compare students’ and preceptors’ views about learner mistreatment using vignettes of student-preceptor interactions. We surveyed 141 students and 203 preceptors at an MD-granting institution. Participants indicated their agreement on a 5-point scale on whether behaviors in 17 written vignettes constituted learner mistreatment. Descriptive statistics and bivariate tests were executed to identify areas in which students’ and preceptors’ mistreatment views differed. Student and preceptor responses converged on 12 of 17 vignettes. More students…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
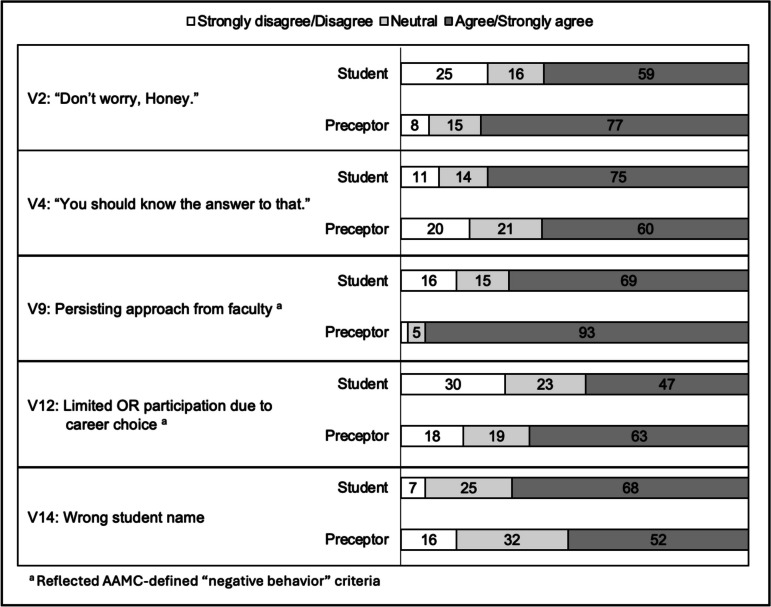 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsWorkplace Violence and Bullying · Communication in Education and Healthcare · Legal Issues in Education
Introduction
The continued prevalence of learner mistreatment in medical education remains a pressing issue in learning environment research and institutional reports [1–6]. In each year since 2018, approximately 40% of graduating medical students in the USA and Canada reported personal experiences with at least one of 16 negative behaviors, excluding public embarrassment, as defined by the Association of American Medical Colleges (AAMC), and 88% of these reported behaviors occurred in clinical settings [7]. Mistreatment has been shown to have direct detrimental effects on the learning environment as a whole, affecting medical students’ content learning, skill acquisition, and confidence [8, 9]. Additional evidence has linked reconsideration of specialty choice and reports of poor mental health to learner mistreatment [10–13]. Furthermore, physicians who report a history of experiencing mistreatment as trainees may be more likely to mistreat patients and healthcare team members [14].
Previous research shows that learners have different opinions of what constitutes mistreatment, and this lack of consensus likely influences reporting decisions [15–18]. Beyond fear of retaliation and lack of trust in processes for addressing problems in the learning environment, students’ reporting decisions are also susceptible to their peers’ and preceptors’ ability to recognize mistreatment behaviors [19, 20]. While medical schools often employ robust reporting systems to monitor the learning environment and act upon reported mistreatment behaviors [20], differing views of whether an event constitutes learner mistreatment are likely to affect awareness, reporting, and potential for intervention [18, 20, 21]. According to Bell et al. [19], peer and faculty feedback can also shape students’ interpretation of acceptable behaviors in the learning environment, and unaligned views can discourage students from reporting mistreatment incidents [22].
To date, very few studies examine whether learner views of mistreatment differ from those of their faculty preceptors [16, 23]. However, Peckston et al. [24] demonstrated differences in faculty and student perceptions of mistreatment related to gender, career choice, public humiliation, and requests to perform unreasonable tasks, providing compelling rationale to further explore these differences. In this study, we use vignettes that illustrate an array of interactions between students and faculty, residents, or other healthcare professionals to examine whether students and preceptors perceive mistreatment differently. Additionally, we consider differences in participants’ neutral responses to vignette cases, as they may reflect uncertainty about mistreatment and/or willingness to reconsider their initial viewpoints [15, 23, 25–27].
Vignettes are widely used for evaluating adult perceptions of behavior as well as instructional tools for cultivating awareness among faculty and trainees, and prior work shows the value of utilizing written cases and descriptive vignettes to evaluate individual views of mistreatment [15–17, 22–27]. This study utilizes 17 written vignettes to examine the perceptions among students and preceptors to address two aims: (1) assess medical students and preceptors’ perceptions of mistreatment, including neutral views, and (2) determine which behaviors yield differing views between these two groups.
Materials and Methods
Survey Setting
In February 2023, we invited medical students, graduate trainees, and faculty from an academic medical center in the Southeastern USA with three regional clinical campus sites to complete an online cross-sectional survey about the learning environment. Participants had the opportunity to submit their responses within a 5-week window. Recruitment consisted of invitations from the school’s leadership team, emailed invitations, and newsletter advertising sent to undergraduate medical students, faculty, and graduate trainees. Eligible participants received three reminder emails while the survey was open. Respondents completed an informed consent process prior to completing the survey. The Institutional Review Board at the investigators’ home institution provided ethical review for this study.
Data Collection Instrument
Written vignettes were designed to evaluate and compare preceptors’ and students’ perceptions of learner mistreatment. The vignettes in this study reflected commonly reported mistreatment behaviors between 2020 and 2022 at the selected institution [28], as well as areas of concern that were reported via a series of discussions with local and regional campus deans, administrators, student services representatives, and students. The authors also reviewed previously published written and video vignettes, as well as training resources used in prior studies, eventually selecting and/or adapting nine previously tested and published cases [15, 16, 23, 24, 29, 30]. Based on qualitative excerpts from Kristoffersson and colleagues [31], as well as input from our institution’s recent graduates, ten additional vignettes were generated.
The authors agreed to explore two main areas of mistreatment behaviors. The first list included behaviors that were reported by recent graduating students on the local AAMC GQ survey: denied training or reward opportunities based on gender; public embarrassment or humiliation; and negative or offensive behaviors based on characteristics other than gender, race/ethnicity, or sexual orientation. The second list included behaviors used in prior publications or those reported locally that were not included in the AAMC list of negative behaviors [32]. This combination contributed to a preliminary list of potential vignettes for this study.
Next, authors iteratively refined each case description for piloting. Two students and one faculty educator provided extensive feedback on 19 pilot vignettes, including one “control” vignette. In subsequent discussions, two cases were removed from the preliminary list, and the sequence in which they appeared in the survey was arranged based on length and portrayed behavior. The final list included 17 vignettes; six cases described behaviors that reflected AAMC-defined “negative behaviors” criteria [32] and 11 cases did not strictly meet these definitions.
The authors used the Qualtrics Survey application to construct and disseminate the survey tool [33]. Participants first indicated their role (i.e., medical student, faculty, resident or fellow, other), and whether they had received training related to the learning environment. For the subsequent portion of the survey, participants were asked to indicate on a 5-point Likert scale the extent to which they agreed or disagreed that each written vignette demonstrated learner mistreatment. In the closing questions, participants reported their gender identity and year of medical school training (MS) or years of teaching experience.
Statistical Analysis
For each vignette, we assigned values of 1–5 to each Likert-type scale category: 1 for “Strongly disagree,” 2 for “Disagree,” 3 for “Neutral,” 4 for “Agree,” and 5 “Strongly agree” [16, 22–24, 27]. Categories in each vignette were subsequently recoded to generate a three-category outcome for each vignette 1 for “Strongly disagree or Disagree,” 1 for “Neutral,” and 3 for “Agree or Strongly agree” [24, 34]. To examine “Neutral” responses specifically, an additional binary variable was generated: 1 for “Strongly disagree, Disagree, Agree, or Strongly agree” and 2 for “Neutral.”
Due to low participation of respondents who identified their role as “Resident or Fellow” and “Other,” we combined these observations with “Faculty” observations, as they would represent the preceptor role. This resulted in two groups of respondents classified as 1 for “Student” and 2 “Preceptor.”
Descriptive statistics were generated to summarize demographic characteristics and responses to vignettes for students and preceptors separately. Listwise deletion was applied to address challenges associated with missing data. This approach yielded an analytic sample of 271 complete observations.
Fisher’s exact tests with Pagano and Halvorsen-computed p values [35] were employed to test differences in the proportions of students’ and preceptors’ Likert-type scale responses for each vignette. Additional Fisher’s exact tests were executed for vignettes that yielded significant results in initial bivariate testing to determine the difference in proportions of “strongly agree or agree” responses between students and preceptors. An additional set of Fisher’s exact tests was performed to test the difference in proportions of students and preceptors who selected “neutral” in each vignette [36]. All statistical analyses were performed using Stata/SE 18 [37].
Results
A total of 351 participants (141 medical students; 203 preceptors) responded to the survey. Table 1 presents the demographic characteristics of medical students (n = 100) and preceptors (n = 171) who completed the entire survey. At the time of the survey, 89% of student respondents identified as male (42%) or female (47%), and 92% of preceptors identified as male (56%) or female (36%). More than half of students identified as first or second year students (MS1 29%; MS2 28%), and 38% identified as a third or fourth year medical students. One-third of preceptors reported teaching only in the clinical setting (35%), another third reported teaching in both pre-clinical and clinical settings (33%), 14% provided pre-clinical training only, and 9% were not teaching medical students at the time that they completed the survey. Table 1. Sample characteristics (N = 271)Student (N = 100)Preceptor (N = 171)(%)(%)GenderGender Male42 (42) Male96 (56) Female47 (47) Female61 (36) Non-binary or non-conforming3 (3) Non-binary or Non-conforming1 (1) Other0 (0) Other1 (1) Prefer not to say8 (8) Prefer not to say12 (7)Medical school yearTeaching setting MS129 (29) Pre-clinical only24 (14) MS228 (28) Pre-clinical and clinical57 (33) MS324 (24) Clinical only60 (35) MS414 (14) I don't teach students16 (9)Graduate program or other leave5 (5) Prefer not to say14 (8)N, observations; MS1, first year; MS2, second year; MS3, third year; MS4, fourth year
Table 2 presents the proportions of medical students’ and preceptors’ responses to each written vignette. Over 75% of both preceptors and students agreed that five of the 17 vignettes (V5, V10, V11, V15, and V16) constituted learner mistreatment. Most preceptors also agreed that behaviors described on V2 and V9 constituted learner mistreatment. Nearly all students agreed that the behaviors in V4 constituted learner mistreatment. Preceptors (86%) and students (82%) also responded similarly to V11 (control vignette). Table 2. The proportion of students’ and preceptors’ (i.e., Faculty, Residents, Fellows, and Other) Likert-scale responses to each vignette and results from Fisher’s exact tests determining difference in students’ and preceptors’ perceptions in each vignette (n = 271)VignetteStudentPreceptorp value(N = 100)(N = 171)V1: Limited Ob/Gyn participation for male student (%)0.092 Strongly disagree or disagree37 (37)42 (25)** Neutral19 (19)36 (21) Agree or** strongly agree44 (44)93 (54)V2: "Don't worry, Honey." (%)0.001 Strongly disagree or disagree25 (25)14 (8)** Neutral16 (16)25 (15) Agree or** strongly agree59 (59)132 (77)V3: Limited OR participation for female student (%)0.789 Strongly disagree or disagree13 (13)27 (16)** Neutral15 (15)27 (16) Agree or** strongly agree72 (72)117 (68)V4: "You should know the answer to that." (%)0.035 Strongly disagree or disagree11 (11)34 (20)** Neutral14 (14)35 (21) Agree or** strongly agree75 (75)102 (60)V5: Student’s preferred pronouns (%)1.000 Strongly disagree or disagree6 (6)10 (6)** Neutral6 (6)11 (6) Agree or** strongly agree88 (88)150 (88)V6: EKG interpretation (Control) (%)0.347 Strongly disagree or disagree82 (82)147 (86)** Neutral12 (12)12 (7) Agree or** strongly agree6 (6)12 (7)V7: "I bet you were a great athlete." (%)0.602 Strongly disagree or disagree18 (18)24 (14)** Neutral23 (23)46 (27) Agree or** strongly agree59 (59)101 (59)V8: Family planning and career choice (%)0.501 Strongly disagree or disagree53 (53)79 (46)** Neutral25 (25)53 (31) Agree or** strongly agree22 (22)39 (23)V9: Persisting approach from faculty (%)** < 0.001**** Strongly disagree or** disagree16 (16)3 (2)** Neutral15 (15)9 (5) Agree or** strongly agree69 (69)159 (93)V10: Misleading report from resident (%)0.101 Strongly disagree or disagree2 (2)14 (8)** Neutral5 (5)10 (6) Agree or** strongly agree93 (93)147 (86)V11: Caregiving tasks (%)0.425 Strongly disagree or disagree8 (8)7 (4)** Neutral16 (16)28 (16) Agree or** strongly agree76 (76)136 (80)V12: Limited OR participation due to career choice (%)0.022 Strongly disagree or disagree30 (30)30 (18)** Neutral23 (23)33 (19) Agree or** strongly agree47 (47)108 (63)V13: Orientation for selected group of students (%)0.237 Strongly disagree or disagree42 (42)78 (46)** Neutral26 (26)54 (32) Agree or** strongly agree32 (32)39 (23)V14: Wrong student name (%)0.017 Strongly disagree or disagree7 (7)28 (16)** Neutral25 (25)54 (32) Agree or** strongly agree68 (68)89 (52)V15: Manuscript authorship (%)0.059 Strongly disagree or disagree3 (3)2 (1)** Neutral4 (4)1 (1) Agree or** strongly agree93 (93)168 (98)V16: Interjecting feedback-English fluency (%)0.067 Strongly disagree or disagree4 (4)12 (8)** Neutral8 (8)28 (16) Agree or** strongly agree88 (88)131 (77)V17: Missed training opportunity (%)0.210 Strongly disagree or disagree37 (37)47 (28)** Neutral20 (20)46 (27) Agree or strongly agree**43 (43)78 (46)n, observations; Ob/Gyn, obstetrics and gynecology; EKG, electrocardiogram; OR, operating room
Student and preceptor perceptions differed significantly on five of the 17 vignettes: V2 (p = 0.001), V4 (p = 0.035), V9 (p < 0.001), V12 (p = 0.022), and V14 (p = 0.017) (see Table 2 and Fig. 1). More students than preceptors agreed that V4 (student = 75%; preceptor = 60%, p = 0.012) and V14 (student = 68%; preceptor = 52%, p = 0.011) constituted learner mistreatment. Compared to students, more preceptors agreed that V2 (student = 59%; preceptor = 77%, p = 0.002), V9 (student = 69%; preceptor = 93%, p < 0.001), and V12 (student = 47%; preceptor = 63%, p = 0.011) demonstrated mistreatment behaviors.Fig. 1. Student and preceptor perceptions on five vignettes with significantly different responses
Table 3 presents the percentages of medical students and preceptors who selected the neutral response for each vignette. The proportion of neutral responses was higher among preceptors for ten of the 17 vignettes (V1, V3, V4, V7, V8, V10, V13, V14, V16, and V17). Compared to preceptors, a greater proportion of students had neutral responses to V9 (student = 15%; preceptor = 5%, p < 0.013). Table 3. The proportion of students and preceptors (i.e., Faculty, Residents, Fellows, and Other) who selected “neutral” in each vignette and results from Fisher’s exact tests testing the difference in the proportion of neutral responses between students and preceptors in each vignette (n = 271)VignetteStudentPreceptorp value(n = 100)(n = 171)**V1: Limited Ob/Gyn participation for male student (%)**0.755Not neutral81 (81)135 (79)Neutral19 (19)36 (21)**V2: "Don’t worry, Honey." (%)**0.861Not neutral84 (84)146 (85)Neutral16 (16)25 (15)**V3: Limited OR participation for female student (%)**1.000Not neutral85 (85)144 (84)Neutral15 (15)27 (16)**V4: "You should know the answer to that." (%)**0.195Not neutral86 (86)136 (80)Neutral14 (14)35 (20)**V5: Student's preferred pronouns (%)**1.000Not neutral94 (94)160 (94)Neutral6 (6)11 (6)**V6: EKG interpretation (Control) (%)**0.186Not neutral88 (88)159 (93)Neutral12 (12)12 (7)**V7: "I bet you were a great athlete." (%)**0.564Not neutral77 (77)125 (73)Neutral23 (23)46 (27)**V8: Family planning and career choice (%)**0.332Not neutral75 (75)118 (69)Neutral25 (25)53 (31)V9: Persisting approach from faculty (%)****0.013Not neutral85 (85)162 (95)Neutral15 (15)9 (5)**V10: Misleading report from resident (%)**1.000Not neutral95 (5)161 (94)Neutral5 (5)10 (6)**V11: Caregiving tasks (%)**1.000Not neutral84 (84)143 (84)Neutral16 (16)28 (16)**V12: Limited OR participation due to career choice (%)**0.534Not neutral77 (77)138 (81)Neutral23 (23)33 (19)**V13: Orientation for selected group of students (%)**0.408Not neutral74 (74)117 (68)Neutral26 (26)54 (32)**V14: Wrong student name (%)**0.270Not neutral75 (75)117 (68)Neutral25 (25)54 (32)**V15: Manuscript authorship (%)**0.064Not neutral96 (96)170 (99)Neutral4 (4)1 (1)**V16: Interjecting feedback-English fluency (%)**0.063Not neutral92 (92)143 (84)Neutral8 (8)28 (16)**V17: Missed training opportunity (%)**0.241Not neutral80 (80)125 (73)Neutral20 (20)46 (27)n, observations; Ob/Gyn, obstetrics and gynecology; EKG, electrocardiogram; OR, operating room
Discussion
Students’ and preceptors’ perceptions did not differ significantly for 13 of the 17 vignettes that were employed in this study. Nearly all participating students and preceptors agreed that one vignette describing the denial of a training opportunity based on gender (V11) and one example of being denied a training opportunity based on training stage (V15) constituted learner mistreatment. Most students and preceptors agreed that one case with comments regarding gender groups (V5), and one case of interjecting feedback about language fluency during a student presentation (V16) constituted learner mistreatment. For these cases, shared mistreatment perceptions among preceptors and students could reflect institution-specific training on appropriate behavior in the learning environment. The majority of students and preceptors responded similarly to V6 (EKG interpretation-control and V10 (misleading report from resident), which is consistent with findings observed in prior studies that employed these cases [24, 29].
Discrepancies in students’ and preceptors’ perceptions of mistreatment were observed for five cases. A higher proportion of preceptors agreed that mistreatment behaviors that could be classified as overt, such as persistent requests to meet with a preceptor outside of work settings (V9) and denial of a training opportunity due to career choice (V12), constituted learner mistreatment. More students agreed that being publicly embarrassed (V4) and being addressed with another student’s name (V14) constituted learner mistreatment, suggesting that students may respond differently to cases that may be more subtle, or in scenarios that are employed less often in mistreatment literature [24]. This finding aligns with prior studies that showed disagreement between students and preceptors regarding mistreatment behaviors that are less overt or that may be shaped by a broader range of contextual factors [16, 23, 24].
Unique to this investigation, we paid special attention to vignettes that illustrated AAMC-defined negative behaviors in order to determine whether these influence whether students’ and preceptors’ mistreatment perceptions align. This was supported by our findings, as differing perceptions were observed in cases that did not resemble AAMC-defined mistreatment behaviors. These results may reflect students’ and preceptors’ familiarity or ability to identify AAMC-defined negative behaviors [7, 19, 38]. Future research should elaborate on factors that shape preceptors’ and students’ interpretations of student-faculty interactions, in order to identify which behaviors most affect decisions about whether mistreatment has taken place, as well as what type of conduct needs addressing, and what interventions are most appropriate [38].
With respect to language, more faculty agreed that addressing students with the term “honey” (V12) constituted learner mistreatment. Hildebrand and colleagues’ [39] showed that “terms of endearment” may be perceived differently by gender. In another study, more female academic hospitalists reported being addressed with terms of endearment than their male counterparts, and participants believed this behavior was disrespectful towards their role in medicine [40]. Further examination of how terms of endearment are used and perceived in medical training may lend important insights on acceptability of this type of behavior, with potential considerations for gender, role, institution, and region.
Not surprisingly, a greater proportion of students (75%) than preceptors (60%) agreed that the case describing a student who may feel embarrassed in front of an audience of peers (V4) constituted learner mistreatment. The proportion of students who considered V4 an example of learner mistreatment may reflect students’ potentially overlapping classification of “public embarrassment” and “public humiliation” reported in prior scholarship [41, 42]. As preceptors may employ Socratic teaching tenets to publicly engage learners in question-based dialog, a student may experience embarrassment if they cannot answer correctly [43]. Several studies have linked public humiliation to specific negative behaviors [44–47], yet learners and preceptors may require structured explanations of expectations along with mistreatment definitions to effectively differentiate public embarrassment and public humiliation [48, 49]. Additional efforts that reinforce definitions of public embarrassment and public humiliation, including the role of intent, are warranted. Professional development on appropriate bedside teaching methods, as well as learner orientation to the purpose of various educational tactics, may decrease conflated reports of public embarrassment and public humiliation events [41].
While most faculty (88%) and students (88%) agreed that disregarding a student’s preferred pronouns constitutes learner mistreatment (V5), this type of behavior is rarely featured in studies and training content regarding gender-related mistreatment. As current definitions of gender- or identity-related mistreatment may not explicitly list preferred pronouns, this finding calls for further investigation and potential revision of mistreatment definitions, categories, and resources to incorporate language preferences [3, 50, 51]. In addition, offering students and preceptors training related to acknowledging the language preferences of their colleagues and peers, as well as incorporating policies that guide this type of professional behavior in the learning environment, is warranted [52–54].
Additional analysis of students’ and preceptors’ selection of “neutral” responses generated important findings. Over 25% of students and faculty remained neutral about whether offering an orientation session for a traditionally minoritized group of students (V13) constituted learner mistreatment. More than a quarter of preceptors selected neutral responses for three additional vignettes (V8, V14, and V17). More students than preceptors were selected neutral responses for V9, in which a preceptor repeatedly asks a student to meet socially outside of the clinical setting. While neutral responses may indicate indecisiveness due to absent contextual information [36], further research and education about how and when learners and preceptors make decisions about mistreatment could generate additional factors that contribute to, or impede mistreatment decisions [25, 38]. The concept of “neutrality” or choosing to remain neutral toward a learning environment scenario has not been published extensively in mistreatment literature, and this study’s findings suggest instances in which learners and preceptors may or may not make decisions about whether a learner has been mistreated.
This study’s findings should be interpreted in light of several limitations; as results are based on data from one institution, vignettes were not designed to illustrate all potential forms of mistreatment behaviors, and not all vignettes included behaviors that met existing parameters for negative behaviors [32]. Additionally, social desirability bias may have prompted participants to select answers that do not reflect their true interpretation of the vignettes [55]. Lastly, the survey instructions did not ask respondents to adopt a particular position (e.g., student, preceptor, third-party observer); rather, participants were only instructed to identify whether a behavior in a scenario constituted learner mistreatment. However, the influence of participants’ real or imagined role, as well as influences of past or present training experiences on their responses, is an important area for further exploration.
These findings add a unique contribution to ongoing mistreatment scholarship by exploring perceptions of written vignettes among students and preceptors from a Southern USA MD-granting institution, including whether respondents made decisions about mistreatment at all (i.e., “neutral” response). The survey tool used in this study incorporated adapted cases from prior vignette studies and prior mistreatment investigations, as well as locally developed cases, and the sample was not limited to persons who have experienced or previously reported mistreatment, which may better represent the general population [15, 16, 23, 24, 29, 31].
Conclusion
The lack of consensus reported in this study is a key finding, as students’ and preceptors’ divergent views on behaviors that constitute learner mistreatment may interfere with identification, decisions to report, and potential intervention, thus perpetuating cycles of unaddressed mistreatment [19, 38]. Students’ and preceptors’ perceptions primarily differed in areas in which existing definitions may be less explicit; prior training regarding professional conduct, as well as individual experiences, may in part explain differing views that were observed [16, 24]. Shared definitions of mistreatment behaviors supply learners, faculty, and administrators with clear concepts and descriptions (e.g., harassment, discrimination) to monitor the learning environment and distinguish behaviors that interrupt the learning process. As learners’ training experiences may still be disturbed by behaviors that may not fit commonly accepted mistreatment definitions, such as unfavorable treatment based on career choice or other characteristics [3, 51, 56, 57], ongoing work is necessary to mitigate gaps and create resources based on a shared understanding of appropriate behavior, including contextual factors, particularly in health professions-specific learning environments.
Highlighted areas of discrepancy reported in this study can inform educational exploration and intervention to increase awareness, refine definitions, enhance shared understanding, and ideally decrease incidence of mistreatment in health professions training environments [22, 58]. Follow-up research is essential for understanding perception, interpretation, and decision-making to improve experiences for all stakeholders in the learning environment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Henning MA, Stonyer J, Chen Y, et al. Medical students’ self-perceptions of harassment during clinical placement. Med Sci Educ 2023/10/27 2023. 10.1007/s 40670-023-01926-510.1007/s 40670-023-01926-5PMC 1094871438510407 · doi ↗ · pubmed ↗
- 2Crombie KE, Crombie KD, Salie M, Seedat S. Medical students’ experiences of mistreatment by clinicians and academics at a South African university. Teach Learn Med 2023;1–10. 10.1080/10401334.2023.216720710.1080/10401334.2023.216720736647677 · doi ↗ · pubmed ↗
- 3AAMC. Medical School Graduate Questionnaire: 2022 All Schools Summary Report. 2022. https://www.aamc.org/media/55736/download
- 4Medicine U So. Understanding and reporting mistreatment. https://hsc.unm.edu/medicine/education/leo/reporting/
- 5Qualtrics. Version 2023. 2020. https://www.qualtrics.com
- 6Vanstone M, Cavanagh A, Molinaro M, et al. How medical learners and educators decide what counts as mistreatment: a qualitative study. Med Educ 2023;57(10). 10.1111/medu.1506510.1111/medu.1506536815430 · doi ↗ · pubmed ↗
- 7Kost A, Chen FM. Socrates was not a pimp: changing the paradigm of questioning in medical education. Acad Med. 2015;90(1):20–4.10.1097/ACM.000000000000044625099239 · doi ↗ · pubmed ↗
- 8Rees CE, Monrouxe LV. “A morning since eight of just pure grill”: a multischool qualitative study of student abuse. Acad Med. 2011;86(11):124–33.10.1097/ACM.0b 013e 3182303 c 4c 21952053 · doi ↗ · pubmed ↗