Invisible Until It Burst: Unexpected Subarachnoid Hemorrhage From a Rapid-Onset Infectious Aneurysm in a Patient With Endocarditis
Tatsuya Tanaka, Talgat Tilyeubyek, Furitsu Shimada, Yuki Takeuchi, Akira Matsuno

TL;DR
A patient with endocarditis developed a sudden, fatal brain aneurysm rupture despite normal earlier imaging, showing how unpredictable these complications can be.
Contribution
Highlights the rapid and unpredictable formation of infectious intracranial aneurysms in endocarditis patients, even when initial imaging is normal.
Findings
A patient with endocarditis developed a fatal ruptured aneurysm three days after normal imaging.
Initial imaging failed to detect the aneurysm, emphasizing the difficulty in predicting its formation.
The case underscores the need for frequent imaging follow-up in endocarditis patients.
Abstract
Infective endocarditis (IE) can lead to serious neurological complications, including septic embolism and infectious intracranial aneurysms (IIAs). Although IIAs are rare, their rupture often results in catastrophic outcomes. Predicting their formation, especially within a short period, remains a clinical challenge. We present the case of a man in his 70s who was newly diagnosed with colon cancer. During preoperative evaluation, transthoracic echocardiography revealed vegetations on the aortic and mitral valves, leading to a diagnosis of IE caused by Streptococcus sanguinis. On the third day of hospitalization, the initial brain magnetic resonance imaging (MRI) revealed asymptomatic cerebral infarction, but magnetic resonance angiography (MRA) did not show any aneurysms. Despite appropriate antibiotic therapy, the patient developed sudden left hemiparesis and impaired consciousness on…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
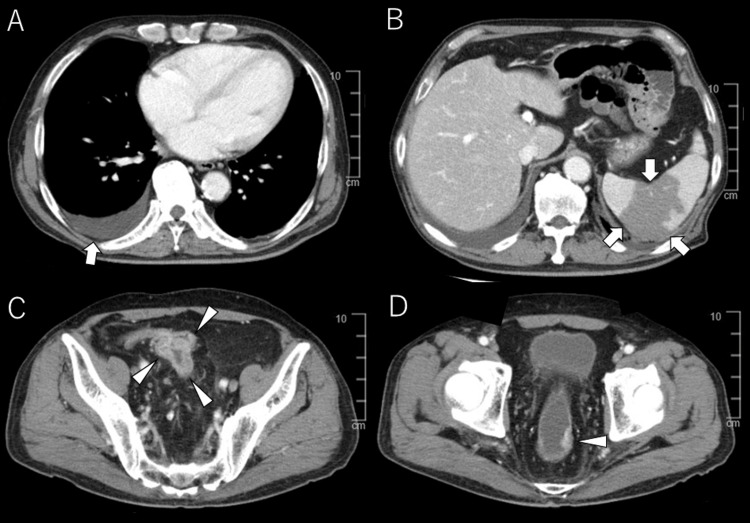 Figure 1
Figure 1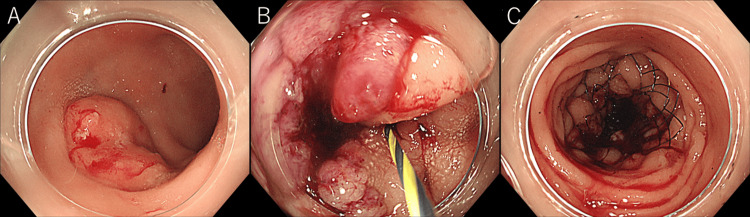 Figure 2
Figure 2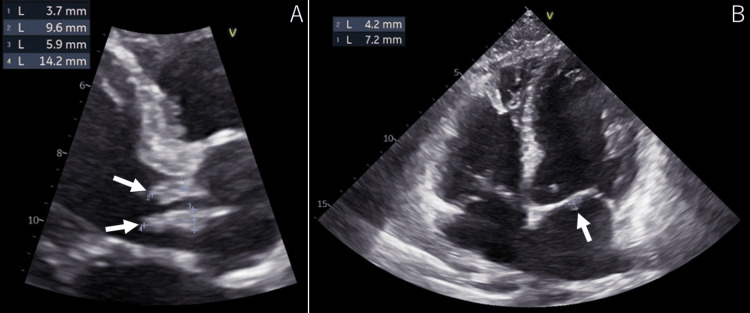 Figure 3
Figure 3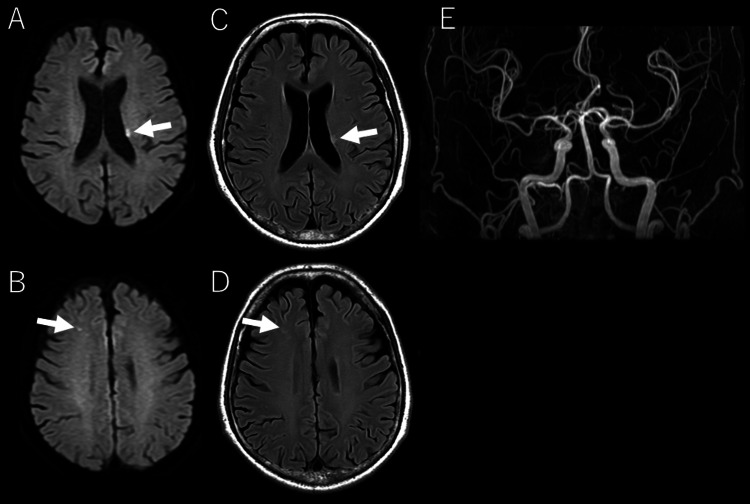 Figure 4
Figure 4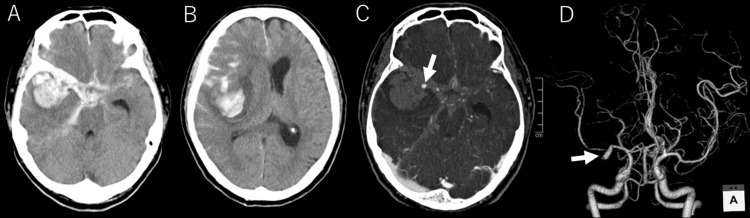 Figure 5
Figure 5| Laboratory test | Result | Normal range |
| White blood cells | 8,220/μL | 4,000-8,000 /μL |
| Red blood cells | 2.65 x 106/μL | 4.35-5.55 x 106/μL |
| Hemoglobin | 7.2 g/dL | 13.7-16.8 g/dL |
| Hematocrit | 23.70% | 40.7%-550.1% |
| MCV | 89.4 fL | 83.6-98.2 fL |
| MCHC | 30.40% | 31.7%-35.3 % |
| RDW | 15.5 fL | 11.8-14.5 fL |
| MPV | 10.7 fL | 8-12 fL |
| Platelet count | 158,000/μL | 140,000-340,000/μL |
| Neutrophils | 87% | 38.5%-80.5% |
| Lymphocytes | 6.90% | 16.5%-49.5% |
| Monocytes | 6.40% | 2.0%-10.0% |
| Eosinophils | 0.00% | 0.0-8.5% |
| Basophils | 0.10% | 0.0-2.5% |
| Glucose | 139 mg/dL | 73-109 mg/dL |
| BUN | 22 mg/dL | 8.0-20.0 mg/dL |
| Creatinine | 0.87 mg/dL | 0.65-1.07 mg/dL |
| Sodium | 139 mEq/L | 138-145 mEq/L |
| Potassium | 3.8 mEq/L | 3.6-4.8 mEq/L |
| Chloride | 108 mEq/L | 101-108 mEq/L |
| Calcium | 8.1 mg/dL | 8.8-10.1 mg/dL |
| Protein (Total) | 6.9 g/dL | 6.6-8.1 g/dL |
| Albumin | 2.9 g/dL | 3.4-5.4 g/dL |
| Bilirubin (Total) | 0.9 mg/dL | 0.4-1.5 mg/dL |
| ALT | 139 U/L | 10-42 U/L |
| AST | 116 U/L | 13-30 U/L |
| Alkaline phosphatase | 176 U/L | 38-113 U/L |
| C-reactive protein | 5.75 mg/dL | 0.00-0.14 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Infectious Aortic and Vascular Conditions · Bacterial Infections and Vaccines
Introduction
Infective endocarditis (IE) remains a life-threatening disease characterized by microbial infection of the endocardial surface of the heart, frequently leading to systemic complications due to septic embolization [1,2]. Among these, neurological events occur in up to 30%-40% of cases, with cerebral infarction being the most common [1,2]. Although rare, infectious intracranial aneurysms (IIAs) are among the most feared complications due to their high risk of rupture and resulting morbidity and mortality [3-5].
IIAs typically arise when septic emboli lodge in cerebral arteries, damaging the vascular endothelium and leading to localized infection, inflammation, and subsequent aneurysm formation [6]. Diagnosis is often delayed, as IIAs can be asymptomatic until rupture [3-5]. Furthermore, the natural history of IIA progression remains poorly defined, and there are no established guidelines for optimal surveillance or the timing of intervention [1,2,7].
Recent reports suggest that IIAs may form and rupture within a matter of days, even in patients with previously normal neurovascular imaging [3-5]. This case highlights such a scenario: a patient with IE developed fatal subarachnoid hemorrhage due to a newly formed ruptured IIA just three days after negative magnetic resonance angiography (MRA), emphasizing the diagnostic difficulties and the importance of close follow-up in high-risk patients.
Case presentation
The patient is a male in his 70s with a history of hypertension, controlled with medication, smoking (20 cigarettes/day for 20 years), and excessive alcohol consumption (50 g/day). He presented to a local medical institution approximately two weeks prior with complaints of loss of appetite and epigastric pain. Blood tests revealed anemia, and black stools were noted. Upper and lower gastrointestinal endoscopy suggested sigmoid colon and rectal cancer, and a biopsy confirmed the diagnosis of advanced colorectal cancer. The patient was subsequently referred to our hospital for further management.
On day 1, clinical laboratory results showed an elevated white blood cell count (WBC 8,220/μL), anemia (hemoglobin 7.2 g/dL), liver dysfunction (alanine aminotransferase [ALT] 139 U/L, aspartate aminotransferase [AST] 116 U/L, and alkaline phosphatase 176 U/L), and elevated inflammatory markers (C-reactive protein [CRP] 5.75 mg/dL). The initial clinical tests are summarized in Table 1.
Contrast-enhanced chest and abdominal computed tomography (CT) revealed cardiomegaly and right-sided pleural effusion (Figure 1A).
Abdominal contrast-enhanced CT.(A) Cardiomegaly with right-sided pleural effusion is observed (arrow).(B) An irregular hypodense area in the spleen is noted, suggestive of splenic infarction (arrow).(C) A localized wall thickening is observed in the sigmoid colon, with heterogeneous post-contrast enhancement, suggestive of sigmoid colon cancer (arrowhead).(D) A small protruding lesion is noted on the left wall of the rectum, consistent with rectal cancer (arrowhead).
Localized wall thickening with heterogeneous enhancement in the sigmoid colon, consistent with sigmoid colon cancer, was observed (Figure 1B). Additionally, a protruding lesion on the left wall of the rectum was consistent with rectal cancer (Figure 1C). An irregular hypodense area in the spleen, suggestive of splenic infarction, was observed (Figure 1D).
On Day 2, a self-expanding metallic stent was placed in the sigmoid colon due to circumferential narrowing caused by colon cancer, resulting in successful lumen expansion (Figure 2).
Lower gastrointestinal endoscopy.(A) A 20 mm protruding lesion is seen in the rectum. (B) Circumferential colon cancer is observed in the sigmoid colon, with narrowing of the lumen. (C) A self-expanding metal stent has been placed.
On Day 3, echocardiography revealed multiple club-shaped masses on the aortic and mitral valves, some exceeding 10 mm in size. The patient was diagnosed with IE complicated by severe aortic and mitral valve regurgitation (Figure 3).
Echocardiography.(A) A club-shaped mass is observed on the aortic and mitral valves (arrow). (B) A mass is observed in the aortic valve annulus (arrow).
Empirical antimicrobial therapy with Sulbactam/Ampicillin (3 g three times daily) and Ceftriaxone (2 g once daily) was initiated. Blood cultures subsequently grew Streptococcus sanguinis. On the same day, head magnetic resonance imaging (MRI) and MRA were performed, revealing asymptomatic subacute ischemic infarction, with no aneurysms identified (Figure 4).
Head MRI and MRA.DWI (A, B) and FLAIR (C, D) show high signal areas in the left corona radiata and frontal lobe, consistent with acute to subacute ischemic infarction.MRA (E) reveals no significant aneurysms.DWI, diffusion-weighted imaging; FLAIR, fluid-attenuated inversion recovery; MRI, magnetic resonance imaging; MRA, magnetic resonance angiography
In the future, open-heart surgery for IE and surgery for colorectal cancer were planned. The average blood pressure from Day 1 to Day 6 was 133/67 mmHg (range: 122-140/52-78).
On Day 6, the patient developed altered consciousness and was found in the bathroom. Physical examination revealed left-sided hemiparesis, and the Japanese Coma Scale score was 100. Pupillary examination revealed a right pupil of 4 mm and a left pupil of 3 mm, with sluggish light reflexes. Vital signs showed a heart rate of 90 bpm, blood pressure of 130/55 mmHg, and oxygen saturation of 93% on room air. A head CT scan was promptly performed, revealing subcortical hemorrhage in the right temporal lobe, along with subarachnoid hemorrhage (SAH) associated with a thick hematoma in the right Sylvian fissure. Compression and narrowing of the right lateral ventricle with a midline shift were also noted (Figures 5A, 5B).
Head CT and CTA.(A, B) Subarachnoid hemorrhage is observed from the basal cistern to the suprasellar cistern, along the bilateral Sylvian fissures, and in the right hemisphere sulci. A subcortical hemorrhage is noted in the right temporal lobe. There is significant compression of the right lateral ventricle with a midline shift to the left.(C, D) A 12 x 3 mm contrast-enhancing mass is observed protruding dorsally from the proximal M1 segment of the right middle cerebral artery, consistent with a pseudoaneurysm (arrow).CTA, computed tomography angiography; CT, computed tomography
Three-dimensional computed tomography angiography (3D CTA) identified a newly formed 12 × 3 mm aneurysm at the proximal M1 segment of the right middle cerebral artery (Figures 5C, 5D).
Given that no aneurysm was seen on the MRA performed on Day 3, it was concluded that an IIA had formed and ruptured within a short period.
Following consultation with the neurosurgery team, several life-saving measures, including external decompression, parent vessel occlusion, and bypass surgery, were considered. However, given the progression of the colorectal cancer and IE, both life expectancy and functional prognosis were deemed extremely poor. After discussions with the patient's family, the decision was made to forgo aggressive treatment, and best supportive care was initiated. The patient's condition gradually worsened, and he passed away on Day 6.
Discussion
IIAs are rare but severe complications of IE, with an incidence reported to range from 2% to 10% of all IE cases [7-10]. The pathophysiology of IIAs involves direct bacterial invasion of the cerebral arterial wall via bacteremia or damage caused by septic emboli, leading to vascular weakening and the subsequent formation of aneurysms [3-6]. The mortality rate for patients with unruptured IIAs is reported to range from 10% to 30%, but it can rise to as high as 80% in cases where rupture occurs [11]. Therefore, timely detection of unruptured IIAs and appropriate intervention are crucial [12].
In the present case, after the diagnosis of IE, initial imaging confirmed the absence of an aneurysm. However, within a few days, an aneurysm developed and subsequently ruptured. Previous reports have described similar cases where aneurysms ruptured unexpectedly despite initial imaging showing no aneurysm [3-5]. In these instances, patients presented with ischemic stroke, and initial imaging studies such as MRA or CTA confirmed the absence of aneurysms. However, rupture of the infectious aneurysm occurred within 38 hours to three days after the imaging. Additionally, the presence of an infectious aneurysm in a previously occluded vessel suggests that the aneurysm likely formed as a result of bacterial embolism, where bacteria invade the cerebral artery wall, causing vascular weakening and aneurysm formation [3,4,5,12]. However, while IE is often associated with ischemic stroke, only 20%-30% of these strokes are symptomatic [1,2]. The occurrence of ischemic stroke does not necessarily predict the formation of an infectious aneurysm. Although many guidelines recommend neuroimaging upon the diagnosis of IE [1,2], they also note that "vascular imaging should not be routinely performed, and CTA or MRA may be sufficient for screening in cases where an infectious aneurysm is suspected. For patients diagnosed with an infectious aneurysm on CTA or MRA, those with acute cerebral hemorrhage, those in whom non-invasive techniques are negative but suspicion remains, and those for whom mechanical thrombectomy is considered, catheter angiography should be performed" [1].
The findings from this case and others suggest that a single negative imaging study may not be sufficient, particularly in high-risk patients. While routine follow-up imaging for all IE patients may not be practical, a risk-based approach could prove beneficial in preventing unexpected aneurysm rupture. The risk factors for the formation and rupture of infectious aneurysms in patients with IE remain unclear, and further research is needed to better understand these mechanisms.
A limitation of this report is that a pathological examination of the aneurysm was not performed. Although arterial dissection could also have contributed to aneurysm rupture, given the patient's IE and the absence of findings suggestive of dissection on MRA and CTA, the rupture is most likely due to an infectious aneurysm.
Conclusions
This case illustrates the rare but devastating complication of rapidly forming and rupturing IIAs in the setting of IE. Despite appropriate antimicrobial therapy and negative neurovascular imaging early in the disease course, a fatal SAH occurred within days due to the abrupt development of a ruptured aneurysm. Even when initial neuroimaging is negative, the risk of IIA should not be excluded. Clinicians should remain vigilant for the possibility of sudden neurological deterioration, even in the absence of radiographic evidence of an aneurysm, as timely detection and intervention are crucial for improving outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 12023 ESC Guidelines for the management of endocarditis Eur Heart J Delgado V Ajmone Marsan N de Waha S 394840424420233762265610.1093/eurheartj/ehad 193 · doi ↗ · pubmed ↗
- 2Infective endocarditis Nat Rev Dis Primers Holland TL Baddour LM Bayer AS Hoen B Miro JM Fowler VG Jr 16059220162758241410.1038/nrdp.2016.59PMC 5240923 · doi ↗ · pubmed ↗
- 3Successful coil embolization of a ruptured mycotic aneurysm that developed three days after septic embolic infarction: case report and review of the literature J Clin Neurosci Wang JL Hinduja AP Powers CJ 95983920172820930610.1016/j.jocn.2017.01.021 · doi ↗ · pubmed ↗
- 4Short-term aneurysm formation and rupture due to septic embolism diagnosed with a thrombus retrieved from another occluded artery Surg Neurol Int Nukata R Ikeda H Akaike N 4741320223632495510.25259/SNI_727_2022 PMC 9610041 · doi ↗ · pubmed ↗
- 5A case of infectious intracranial aneurysm that formed and ruptured within a few days after occlusion of the proximal middle cerebral artery by infective endocarditis Surg Neurol Int Yanagawa T Ikeda S Yoshitomi S Shibata A Ikeda T 1931420233740451210.25259/SNI_229_2023 PMC 10316150 · doi ↗ · pubmed ↗
- 6Intracranial infectious aneurysms: a comprehensive review Neurosurg Rev Ducruet AF Hickman ZL Zacharia BE Narula R Grobelny BT Gorski J Connolly ES Jr 37463320101983874510.1007/s 10143-009-0233-1 · doi ↗ · pubmed ↗
- 7Management and long-term outcomes of patients with infectious intracranial aneurysms Neurosurgery Alawieh AM Dimisko L Newman S 5155239220233670069610.1227/neu.0000000000002235 PMC 10158861 · doi ↗ · pubmed ↗
- 8National treatment practices in the management of infectious intracranial aneurysms and infective endocarditis J Neurointerv Surg Singla A Fargen K Blackburn S 741746820162604498610.1136/neurintsurg-2015-011834 · doi ↗ · pubmed ↗