Comparative evaluation of mechanical and biological prostheses in patients with aortic stenosis
Juan Andres Montero, Federica Venturino, Santiago Cubas, Sofía Rodríguez, Maximiliano Hernández, Carolina Sosa, Maximiliano Rodríguez, Daniel Brusich, Victor Dayan

TL;DR
This study compares mechanical and biological aortic valve prostheses, finding that biological prostheses may be less effective in younger males and those not on statins.
Contribution
The study identifies age 70 as a threshold for biological prosthesis benefit and highlights the importance of gender and statin use in decision-making.
Findings
Bioprostheses were linked to higher mortality in males and patients not on statins.
Bioprostheses showed higher risk in patients under 60 and lower risk in those aged 70–79.
Age 70 was identified as the threshold where bioprostheses outperformed mechanical ones.
Abstract
The commonly accepted aortic valve prostheses have been either mechanical or biological. Each type has its advantages and disadvantages, with age being the most widely accepted variable to determine the best option. There is, however, a range between 60 and 70 years where an individualized approach is required. This is a retrospective study. The primary outcome was overall survival based on the type of prosthesis used, stratified by effect modifiers. Association between prosthesis type and mortality rate was evaluated using the incidence rate ratio. Secondary outcomes included cardiovascular survival, postoperative mortality and complications, adjusted for age. Cox regression analysis was performed to account for confounders. Variation in the hazard ratio for death by age was explored by fitting a restricted cubic spline to the interaction between age and valve type. We included all…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
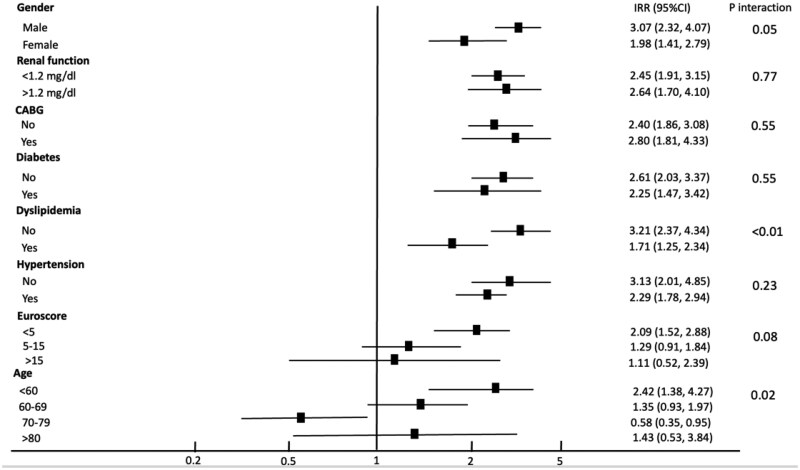 Figure 1
Figure 1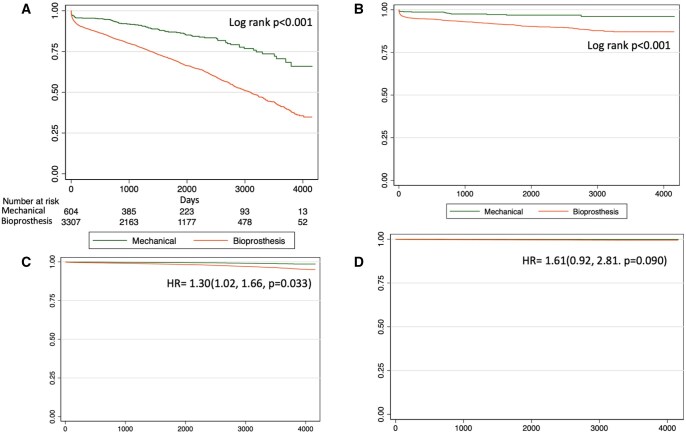 Figure 2
Figure 2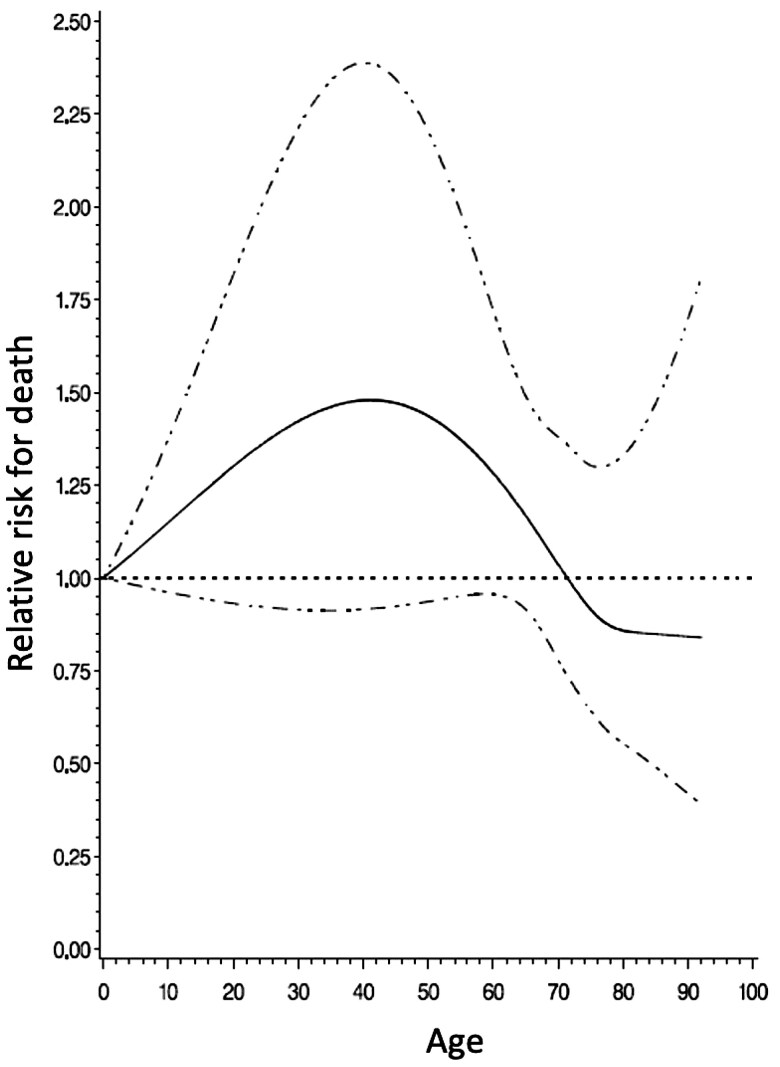 Figure 3
Figure 3| BP ( | MP ( | Total ( |
| |
|---|---|---|---|---|
| Mean age (SD) | 73.5 (6.8) | 57.5 (10.3) | 71.0 (9.4) | <0.001 |
| Age (%) | <0.001 | |||
| <60 | 74 (2.2) | 354 (57.9) | 428 (10.85) | |
| 60–69 | 831 (24.9) | 201 (32.9) | 1032 (26.2) | |
| 70–79 | 1775 (53.3) | 45 (7.4) | 1820 (46.1) | |
| ≥80 | 653 (19.6) | 11 (1.8) | 664 (16.8) | |
| Female (%) | 1486 (44.6) | 222 (36.3) | 1708 (43.3) | <0.001 |
| Hypertension (%) | 2721 (81.6) | 393 (64.3) | 3114 (79.0) | <0.001 |
| Diabetes (%) | 834 (25.0) | 114 (18.7) | 948 (24.0) | <0.001 |
| Smoker (%) | 763 (22.9) | 150 (25.6) | 913 (23.2) | 0.37 |
| Obesity (%) | 628 (18.8) | 70 (11.4) | 698 (17.7) | |
| Creatinine mg/dl (SD) | 1.08 (0.70) | 1.06 (0.86) | 1.08 (0.73) | 0.43 |
| Statins (%) | 1481 (44.4) | 201 (32.9) | 1682 (42.7) | <0.001 |
| Previous infarction (%) | 69 (2.1) | 7 (1.2) | 76 (1.9) | 0.12 |
| Atrial fibrillation (%) | 81 (2.4) | 13 (2.1) | 94 (2.4) | 0.65 |
| NYHA III/IV (%) | 805 (28.6) | 131 (26.3) | 936 (28.3) | 0.62 |
| LVEF (SD) | 57.5 (10.6) | 58.0 (10.4) | 57.6 (10.5) | 0.28 |
| Concomitant CABG (%) | 1201 (36.0) | 122 (20.0) | 1323 (33.5) | <0.001 |
| EuroSCORE I (SD) | 7.47 (4.30) | 4.02 (3.38) | 6.9 (4.4) | <0.001 |
| Variable | Multivariate |
|
|
|---|---|---|---|
| Bioprosthesis | 0.04 | ||
| Male | 1.45 (1.06, 1.98) | 0.02 | |
| Female | 0.90 (0.63, 1.30) | 0.59 | |
| <60 year old | 2.51 (1.42, 4.13) | < 0.001 | 0.01 |
| 60–69 year old | 1.19 (0.82, 0.58) | 0.36 | |
| 70–79 year old | 0.65 (0.39, 1.06) | 0.09 | |
| >80 year old | 1.75 (0.63, 4.71) | 0.27 | |
| Age | 1.02 (1.01, 1.03) | <0.001 | |
| Creatinine | 1.09 (1.04, 1.16) | <0.001 | |
| Statins | 1.16 (1.04, 1.30) | <0.001 | 0.16 |
| Diabetes | 1.29 (1.14, 1.47) | <0.001 | |
| Hypertension | 1.16 (1.00, 1.35) | 0.05 | |
| CABG | 1.11 (0.99, 1.24) | 0.07 |
| Bioprosthesis (3333) | Mechanical (611) | OR (95%CI) |
| |
|---|---|---|---|---|
| Operative mortality | 198 (5.9) | 23 (3.8) | 0.86 (0.51, 1.43) | 0.55 |
| Surgical re-exploration | 181 (5.4) | 22 (3.6) | 1.42 (0.84, 2.39) | 0.19 |
| Postoperative infections | 475 (14.3) | 63 (10.3) | 1.01 (0.72, 1.40) | 0.98 |
| Stroke | 83 (2.49) | 9 (1.47) | 1.55 (0.70, 3.44) | 0.28 |
| Atrial fibrillation | 1238 (37.1) | 122 (20.0) | 1.34 (1.05, 1.71) | 0.02 |
| AV block | 239 (7.2) | 33 (5.4) | 0.98 (0.63, 1.52) | 0.93 |
| PPM | 112 (3.4) | 15 (2.5) | 1.09 (0.58, 2.07) | 0.79 |
| Acute renal failure | 417 (12.5) | 43 (7.0) | 0.94 (0.66, 1.34) | 0.74 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Infective Endocarditis Diagnosis and Management · Aortic Disease and Treatment Approaches
INTRODUCTION
The effective treatment for severe aortic valve disease remains surgical aortic valve replacement (SAVR) or transcatheter aortic valve implantation (TAVI). To date, the commonly accepted aortic valve prosthesis are the mechanical prostheses (MP) or the BP. Each has its advantages and disadvantages, with age currently being the most frequently accepted clinical variable to define the best option. MP is likely to be recommended for younger patients (<50–60 years), while BP is preferred for older patients (>65 years) [1, 2]. There is an age range between 50 and 65 years, according to the guidelines of the American College of Cardiology and the American Heart Association (ACC/AHA), or between 60 and 65 years as per the guidelines of the European Society of Cardiology and the European Association of Cardiothoracic Surgery (ESC/EACTS), where an individualized approach is recommended. In this age group, the only published randomized controlled trial found no differences in survival, with a higher incidence of prosthetic failure and reoperation in the BP group [3]. A recent meta-analysis of primarily retrospective studies found that MP were associated with better survival in this age group [4]. Considering the increasing number of TAVI procedures performed in younger patients (<70 years), it is imperative to confirm the superiority of BP (or not) in comparison to MP in this age group, as well as the predictors that may favour one prosthesis over the other for this group. Our objective was to evaluate survival in a national cohort of patients who required SAVR due to aortic stenosis (AS) using either MP or BP.
METHODS
Ethical statement
The Ethics Review Board of the Hospital de Clínicas (approval number 6220001) approved the study on the 22nd of March 2022, and the requirement for informed consent was waived due to the retrospective nature of the research.
This is a retrospective study using data from Uruguay, sourced from the National Resource Fund (FNR) that is the national entity that fully covers 100% of cardiac surgical procedures in Uruguay. Data submission to the FNR is mandatory to obtain financial approval for each procedure.
Patients
All patients who underwent SAVR for AS in Uruguay between 2011 and 2021 were included (type and model of prostheses used in Supplementary Material, Table S3). Exclusion criteria were urgent or emergency surgery, endocarditis, moderate AS, severe aortic reguritation, previous cardiac surgery, concomitant mitral valve or ascending aorta replacement.
Preoperative, intraoperative and immediate postoperative data were extracted from the FNR. Expected mortality was assessed using EuroSCORE I (logistic model). Calculation of EuroSCORE II was not feasible as the study included patients from before EuroSCORE II was established, and the registry lacks the necessary data for its calculation. Vital status and cause of death were obtained from the Department of Epidemiology of the Ministry of Health.
Objectives
The primary outcome was overall survival based on the type of prostheses used, stratified by effect modifiers. The association between prostheses type and mortality rate was evaluated using the incidence rate ratio (IRR). Secondary objectives included cardiovascular survival defined as time from surgery until death due to cardiovascular causes such as acute myocardial infarction, sudden cardiac death or heart failure and postoperative outcomes (postoperative mortality, surgical re-exploration, infections, stroke, atrial fibrillation, atrioventricular block, patient-prosthesis mismatch and acute renal failure) adjusted by age.
Due to a large percentage of patients with BP who received concurrent coronary artery bypass graft (CABG) (36%), a final model for hazard ratio (HR) for overall survival in patients with BP after multivariate adjustment excluding patients who underwent CABG can be found in Supplementary Material (Table S4).
Statistics
Normality of continuous variables was assessed by the Shapiro test. Continuous data are expressed as mean ± SD, while categorical data are expressed as absolute values and percentages. Continuous variables such as age, creatinine levels, left ventricular ejection fraction (LVEF) and EuroSCORE were categorized as follows: age (<60, 60–69, 70–79, >80 years), creatinine levels (<1.2 and >1.2 mg/dl), LVEF (>50%, 50–30%, <30%) and EuroSCORE (<5%, 5–15%, >15%).
Preoperative variables were compared between the groups to identify potential confounders using the chi-squared test (for categorical variables) and Student’s t-test (for continuous variables). Potential confounders were then evaluated using univariate Cox regression analysis to determine their role as confounding factors. Univariate confounding and effect modification were assessed through Mantel-Haenszel stratification, and multivariate adjustment was performed using Cox regression. Interaction in the multivariate Cox regression model was evaluated using the likelihood ratio test for variables identified as modifiers in the univariate analysis. If interaction was present, the interaction term was included in the final model.
Long-term mortality was assessed as the mortality rate, with the numerator being the number of events (deaths) and the denominator being person-days of follow-up. The association between prosthesis type and mortality rate was evaluated using the IRR (Supplementary Material, Table S1). The IRR and its 95% confidence interval (CI) were calculated using the Mantel-Haenszel method. Considering that the age group of 60–70 years is recommended for either bioprosthesis or mechanical valve, the IRR was also calculated for each age group, and a subgroup analysis was performed for patients aged 60–70 years. Interaction was assessed using the chi-squared test. Cases with missing information were excluded in the multivariate analysis.
Survival was analysed using the Kaplan–Meier method, and comparisons between groups were made using the log-rank test.
Postoperative outcomes were compared between groups and adjusted for age groups using logistic regression.
The variation in the mortality risk index between MP and BP by age was explored by adjusting a restricted cubic spline to the interaction between age and valve type, using five knots.
RESULTS
A total of 3944 patients who underwent SAVR in Uruguay between 2011 and 2021 were included in the study. The mean age of the cohort was 71 (SD: 9.4) years, most of them were women (43.3% vs 56.7%, P < 0.001), and the mean EuroSCORE I was 6.9% (7.47% in BP vs 4.02% in MP, P < 0.001). Patients receiving a BP were older on average (73.5 vs 57.5 years, P < 0.001) and had a higher prevalence of female sex (44.6% vs 36.3%, P < 0.001), diabetes (25% vs 18.7%, P < 0.001), statins (44.4% vs 32.9%, P < 0.001), hypertension (81.6% vs 64.3%, P < 0.001), elevated creatinine levels (>1.2 mg/dl) (24.5% vs 18.7%, P < 0.001) and concomitant coronary surgery (36% vs 20%, P < 0.001) (Table 1). The predicted mortality was higher in patients receiving BP (7.47 (SD: 4.30) vs 4.02 (SD: 3.38), P < 0.001).
Primary objective
The unadjusted IRR showed a higher risk in patients receiving BP (IRR = 2.57; 95% CI: 2.07–3.20, P < 0.001). Univariate adjustment revealed that age (P for interaction = 0.02), sex (P for interaction = 0.05) and statins (P for interaction < 0.01) were effect modifiers of the impact of BP on mortality rate (Fig. 1). When stratifying mortality rates by age group, BP was associated with higher risk in patients under 60 years (IRR = 2.42; 95% CI: 1.38–4.27, P for interaction = 0.02) and lower risk in patients aged 70–79 years (IRR = 0.58; 95% CI: 0.35–0.95, P for interaction = 0.02) (Fig. 1). No significant differences were observed in the 60–69 or >80 age groups. Similarly, the impact of BP on mortality was greater in males (IRR = 3.07; 95% CI: 2.32–4.07) compared to females (IRR = 1.98; 95% CI: 1.41–2.79, P for interaction = 0.05) and was higher in patients without statins (IRR = 3.21; 95% CI: 2.37–4.34) compared to those with statins (IRR = 1.71; 95% CI: 1.25–2.34, P for interaction = 0.02).
Forest plot for mortality incidence rate ratio for bioprostheses with adjustment for confounders and stratum-specific associations (n = 3944)
Adjusted and unadjusted survival was lower in patients receiving BP (Fig. 2).
Kaplan–Meier survival curves. Overall (A) unadjusted and (C) adjusted survival. Cardiovascular (B) unadjusted and (D) adjusted survival
Univariate predictors of survival included age, sex, creatinine levels, concomitant coronary surgery, EuroSCORE, BP, statins, diabetes and hypertension (Supplementary Material, Table S2).
After multivariate regression and interaction analysis, BP use was an independent predictor of overall survival in male patients (HR = 1.45; 95% CI: 1.06–1.98, P = 0.018) but not in females (HR = 0.90; 95% CI: 0.63–1.30). Additionally, its use was significantly associated with worse outcomes in patients under 60 years (HR = 2.51; 95% CI: 1.42–4.13) and better outcomes in the 70–79 age group (HR = 0.65; 95% CI: 0.39–1.06) (Table 2). Although no significant interaction was observed after multivariate adjustment for statins, a strong negative effect on survival was noted in patients without statins.
When analysing the relative risk of survival benefit with BP by increasing age, 70 years emerged as the threshold at which BP demonstrated a survival benefit over MP (Fig. 3).
Hazard ratio of death and 95% confidence intervals (dashed lines) by age
Patients aged 60–69 years
Subgroup analysis of patients aged 60–69 years showed no interaction in any analysed subgroups. However, male sex (IRR = 1.67; 95% CI: 1.04–2.70) and absence of statins (IRR = 1.83; 95% CI: 1.06–3.18) were significantly associated with worse outcomes with BP (Supplementary Material, Fig. S1).
Secondary objectives
Unadjusted cardiovascular survival was lower in patients receiving BP, but no differences were found after adjusting for confounders (Fig. 2).
There were no differences in postoperative outcomes except for an increased risk of postoperative atrial fibrillation with BP (OR = 1.34; 95% CI: 1.05–1.71, P = 0.02) (Table 3).
DISCUSSION
After multivariate analyses, BP were associated with worse survival in male patients and in those under 60 years of age. A trend towards improved survival was observed in the 70–79 age group. The significant association between survival and BP use in patients without statins, as well as the influence of gender, should be considered when deciding on the type of prosthesis for patients aged 60–69 years. This was discussed in depth in a companion article published in 2024 by Dayan et al. about medium-term survival of patients with aortic prosthesis at the sixth decade of life [5]. There is no clear age threshold at which the ACC/AHA or ESC/EACTS guidelines decisively recommend BP over MP, or vice versa. Current guidelines suggest that patients under 50 years of age may benefit from MP, while those over 65 years are generally recommended for BP use [1, 2]. However, studies on intermediate age groups (50–70 years) have shown conflicting results. Chiang et al. [6], in a 10-year retrospective follow-up of patients undergoing SAVR in New York State, reported no differences in long-term mortality in this age group. Similarly, Attia et al. [7], using data from the Cleveland Clinic, found no differences in long-term survival between valve types in this age group. Moreover, they reported no survival differences in patients requiring reintervention. However, Attia et al.’s findings may have limited external validity and should be interpreted with caution when applied to cardiac surgery centres with lower surgical volumes.
In contrast, other studies have reported better survival with MP in this age group. For instance, Brown et al. [8] in the USA and Glaser et al. [9] in Sweden demonstrated superior survival rates with MP in patients aged 50–70 years. These discrepancies highlight the need for individualized decision-making based on patient characteristics, local expertise and institutional factors. Most data comparing BP and MP originate from the USA or Europe. Factors such as anticoagulation management and technical expertise at cardiac surgery centres significantly influence the relative benefits of each valve type. Thus, evidence from centres outside these regions is crucial to gaining a global perspective and improving the external validity of available data.
Our national data, derived from a Latin American country, do not align with the findings of Goldstone et al. [10] in California. Goldstone et al. reported that the survival benefit of MP persisted only up to age 55. In contrast, we identified age 70 as the turning point where the benefit of MP was surpassed by BP.
The primary disadvantage of BP is degeneration and the need for reintervention. However, if severe degeneration is detected early and reoperations are successfully performed, the disadvantages of BP are mitigated, potentially shifting the age threshold for benefit towards younger patients.
Cardiac surgery centres in Uruguay, representing Latin American countries, likely differ from those in the USA in terms of delayed diagnosis and potentially worse outcomes following reinterventions. These factors may explain the observed benefit of MP up to age 70 in our population.
Clearly, the optimal choice of prosthesis for patients aged 50 to 70 is not absolute. Identifying subgroups of patients who may benefit from either valve type is essential. Gender is a particularly important subgroup that has been insufficiently studied in the literature.
Kulik et al. [11] found better outcomes with BP in female patients, possibly due to a reduced need for reinterventions. Similarly, a Finnish nationwide study [12] demonstrated a lower reintervention rate in women. Hammermeister et al. [13] in a randomized trial of male patients, reported higher long-term mortality with BP. Other studies have shown that gender is a significant confounder in the relative benefits of MP [14].
Although high-dose statin therapy has not succeeded in halting the calcification of native aortic valves [15], limited evidence exists regarding their benefit in BP. Antonini-Canterin et al. [16] demonstrated an association between statin use and a reduction in the progression of BP degeneration. Additionally, rosuvastatin has been shown in animal models to decrease BP calcification [17]. In our cohort, patients with dyslipidaemia who received BP exhibited better outcomes. While medication use was not a variable in our database, it is likely that these patients were on statins, and the observed benefit may be attributable to their reported role in slowing BP degeneration. Further randomized controlled trials are necessary to test this association. This difference may be related to the inflammatory response and haemodynamic stress associated with biological valves, also knowing that the age and number of comorbidities that these patients had at the time of surgery was greater, these results were similar to those found by Rikhard Björn et al. [18].
We know that these results may vary today, given the advances in valve-in-valve TAVI (ViV-TAVI), which make it necessary to choose a bioprosthesis for patients at high risk of reintervention, thereby increasing their survival. A recent study by Danial Ahmad et al. [19] retrospectively compared patients who underwent ViV-TAVI and native valve TAVI. Of 3532 patients, 198 (5.6%) underwent ViV-TAVI. The ViV-TAVI group had a higher incidence of major vascular complications (2.5% vs 0.8%, P = 0.008), a lower rate of permanent pacemaker placement (2.5% vs 8.1%, P = 0.004) and a comparable incidence of stroke (2.5% vs 2.4%, P = 0.911). In a multivariate Cox regression analysis, ViV-TAVI was associated with a reduced risk of death (HR 0.68 [0.5 to 0.9], P = 0.02). Therefore, ViV-TAVI appears to be a feasible and safe strategy for high-risk patients with bioprosthetic valve failure, potentially influencing survival rates and prosthesis selection in this patient group. As well as with new generation biological valves that promise greater durability, thanks to an anticalcification coating process on its leaflets, it ensures better haemodynamics and improvements in tissue preservation processes, which could translate into greater durability and better clinical performance. In addition, it incorporates new technology, which facilitates future ViV procedures in patients who may require reinterventions. The COMMENCE trial by Bavaria et al. [20] published in 2023 confirms these hypotheses after following patients with new generation RESILIA tissue valves for 5 years.
CONCLUSION
Our findings confirm that gender strongly influences outcomes after SAVR and should be carefully considered. Our data suggest that male patients in the 60–70 year-old age group likely benefit more from MP, while female patients may achieve favourable outcomes with either strategy.
Limitations
As a retrospective study, selection bias is the primary limitation. To account for measured confounders, we performed Cox regression analyses. However, we acknowledge the potential influence of unmeasured confounders on the results.
We relied on the national database to extract outcome variables. The follow-up of postoperative outcomes and cross-referencing with other national databases is suboptimal. Consequently, we were unable to evaluate critical outcomes such as readmissions, reoperations, strokes or bleeding events.
Supplementary Material
ivaf091_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Otto CM , Nishimura RA, Bonow RO et al 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021;143:e 72–227. doi: 10.1161/CIR.000000000000092333332150 · doi ↗ · pubmed ↗
- 2Vahanian A , Beyersdorf F, Praz F et al; ESC/EACTS Scientific Document Group. 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J 2022;43:561–632.34453165 10.1093/eurheartj/ehab 395 · doi ↗ · pubmed ↗
- 3Stassano P , Di Tommaso L, Monaco M et al Aortic valve replacement: a prospective randomized evaluation of mechanical versus biological valves in patients ages 55 to 70 years. J Am Coll Cardiol 2009;54:1862–8.19892237 10.1016/j.jacc.2009.07.032 · doi ↗ · pubmed ↗
- 4Jiang Y , Wang S, Bian J, Chen S, Shao Y. Mechanical versus bioprosthetic aortic valve replacement in middle-aged adults: a systematic review and meta-analysis. J Cardiovasc Dev Dis 2023;10:90.36826586 10.3390/jcdd 10020090 PMC 9965629 · doi ↗ · pubmed ↗
- 5Dayan V , Montero JA, Freemantle N. Medium-term survival of patients with mechanical and biological aortic prosthesis at the 6th decade of life. P Lo S One 2024;19:e 0312408. doi: 10.1371/journal.pone.031240839556548 PMC 11573135 · doi ↗ · pubmed ↗
- 6Chiang YP , Chikwe J, Moskowitz AJ, Itagaki S, Adams DH, Egorova NN. Survival and long-term outcomes following bioprosthetic vs mechanical aortic valve replacement in patients aged 50 to 69 years. JAMA 2014;312:1323–9.25268439 10.1001/jama.2014.12679 · doi ↗ · pubmed ↗
- 7Attia T , Yang Y, Svensson LG et al; Members of the Cleveland Clinic Aortic Valve Center. Similar long-term survival after isolated bioprosthetic versus mechanical aortic valve replacement: a propensity-matched analysis. J Thorac Cardiovasc Surg 2022;164:1444–55.e 4.33892946 10.1016/j.jtcvs.2020.11.181 · doi ↗ · pubmed ↗
- 8Brown ML , Schaff HV, Lahr BD et al Aortic valve replacement in patients aged 50 to 70 years: improved outcome with mechanical versus biologic prostheses. J Thorac Cardiovasc Surg 2008;135:878–84; discussion 884.18374773 10.1016/j.jtcvs.2007.10.065 · doi ↗ · pubmed ↗