Laparoscopic cholecystectomy plus endoscopic retrograde direct cholangioscopy: an integrated strategy for Mirizzi syndrome
Zhu-Hui Liu, Yu-Tong Yao, Guang-Ming Xiang, Wei-Hui Liu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1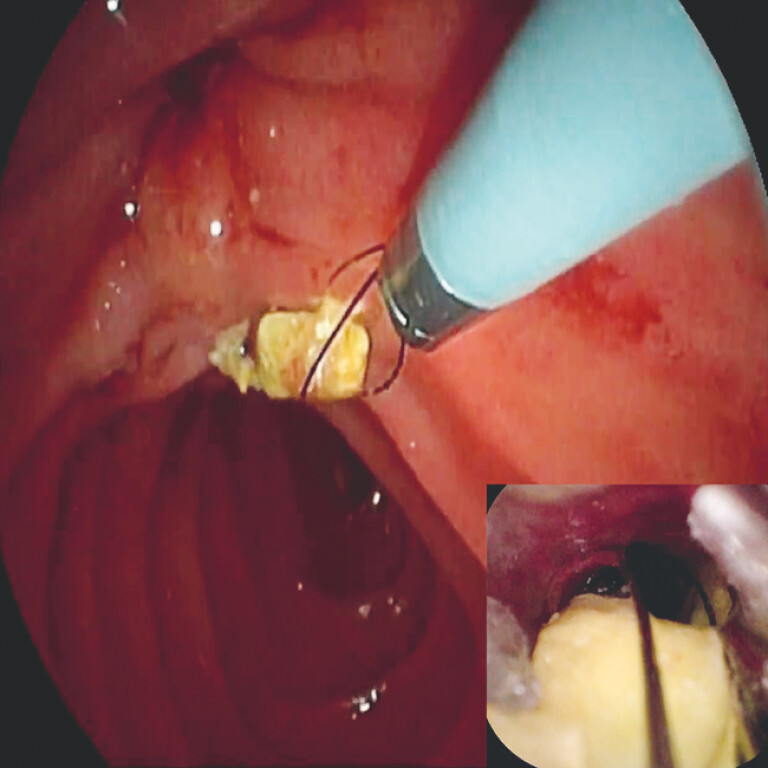 Fig. 2
Fig. 2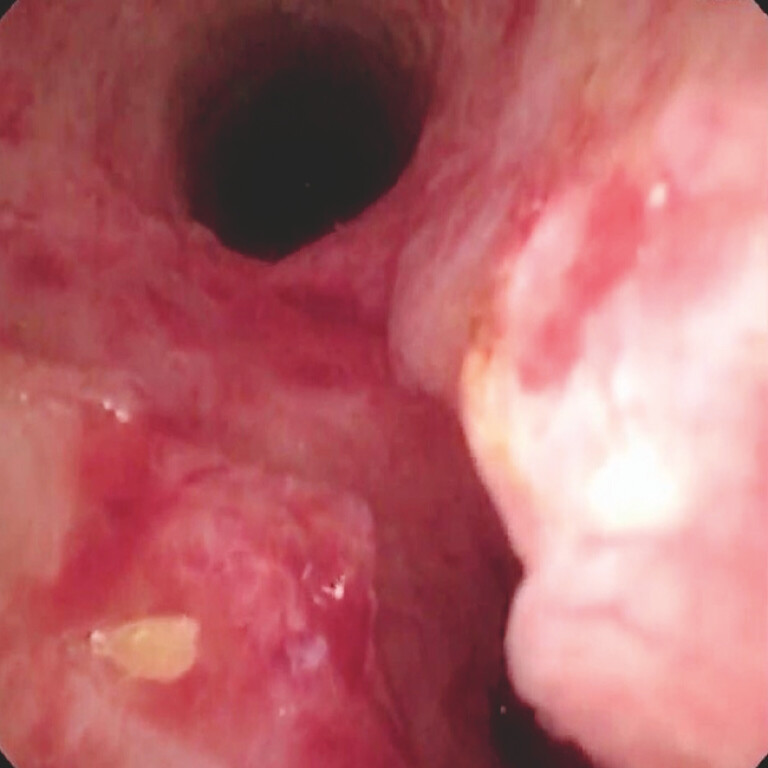 Fig. 3
Fig. 3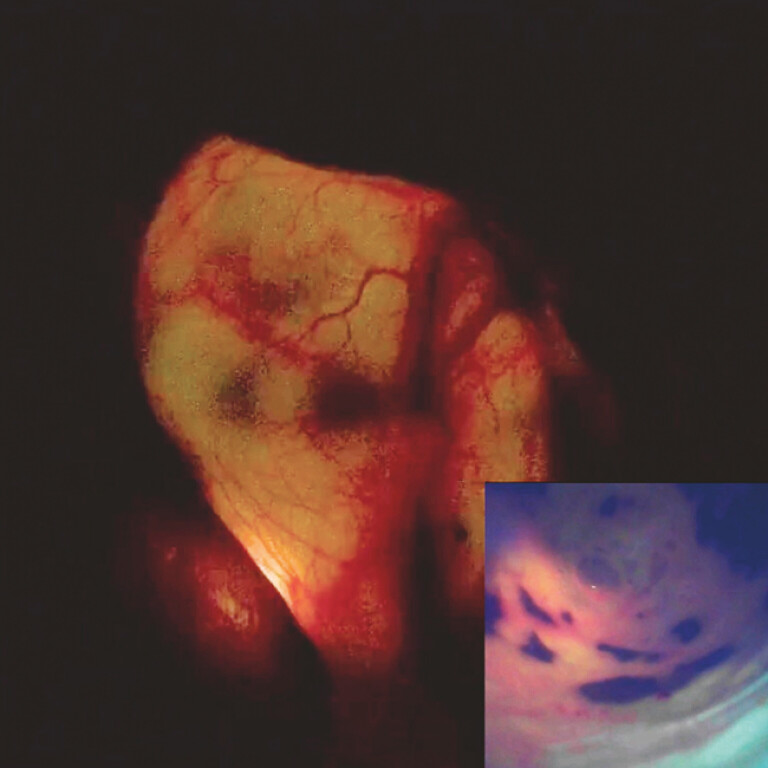 Fig. 4
Fig. 4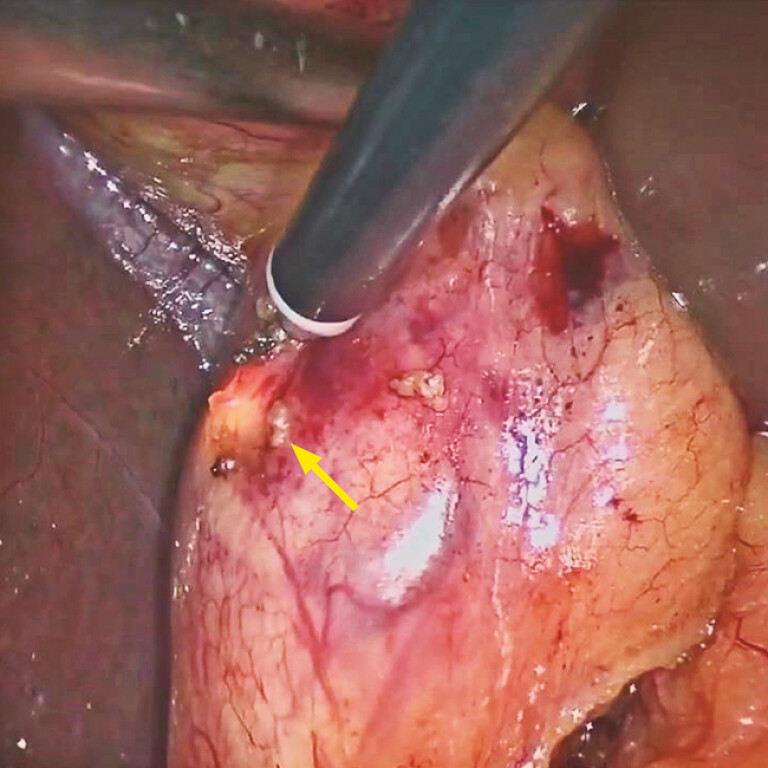 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBiliary and Gastrointestinal Fistulas · Gallbladder and Bile Duct Disorders · Pediatric Hepatobiliary Diseases and Treatments
Mirizzi syndrome, a rare but serious complication of cholelithiasis, is difficult to differentiate from cholangitis and choledocholithiasis. Despite the help of preoperative imaging, more than 50% of cases of Mirizzi syndromes are still diagnosed intraoperatively 1 . Even if the preoperative diagnosis is clear, intraoperative cholangiography, choledochoscopy, or intraductal ultrasonography may still be needed to confirm the diagnosis and determine the presence, size, and location of the fistula 2 . Therefore, we propose an integrated strategy for suspected Mirizzi syndrome, this being to perform endoscopic retrograde direct cholangioscopy (ERDC) 3 4 simultaneously during laparoscopic cholecystectomy, to simplify the diagnosis and treatment process while ensuring safety ( Video 1 ).
Laparoscopic cholecystectomy plus endoscopic retrograde direct cholangioscopy are performed, providing an integrated strategy for Mirizzi syndrome.Video 1
A 41-year-old man in our hospital was suspected of having Mirizzi syndrome. Laparoscopic cholecystectomy and ERDC were performed simultaneously without radiography support. First, direct vision through the cholangioscope revealed the cystic duct stone and the compressed common hepatic duct, which confirmed the diagnosis of Mirizzi syndrome ( Fig. 1 ). The stone was removed using a slim extraction basket and saline irrigation after electrohydraulic lithotripsy ( Fig. 2 ). Under cholangioscopic visualization, we confirmed the common bile duct (CBD) was a sealed cavity without residual stones, which also meant this patient had type I Mirizzi syndrome ( Fig. 3 ). A porcelain gallbladder could be observed through the unobstructed cystic duct, while laparoscopically the gallbladder appeared luminous ( Fig. 4 ). Guided by the light of the cholangioscope, we were able to accurately identify the cystic duct, CBD, and common hepatic duct ( Fig. 5 ). After the gallbladder triangle had been dissected, the gallbladder was successfully excised. The patient made a full recovery, with no complications reported.
Cholangioscopic view showing the obstructing cystic duct stone.
Endoscopic view showing the cystic duct stone being removed with a slim extraction basket and saline irrigation after electrohydraulic lithotripsy had been performed.
Cholangioscopic view showing no evidence of leaks or residual stones in the common bile duct.
Laparoscopic view showing luminosity of the gallbladder (inset: cholangioscopic image of the porcelain gallbladder).
Image during laparoscopic cholecystectomy showing how the cholangioscope provided a direct indication of the location of the bile duct.
In our practice, ERDC clarified the diagnosis and classification of Mirizzi syndrome, removed the obstructing stones, provided direct guidance for laparoscopic gallbladder triangle dissection, and avoided the huge trauma caused by open surgery. Our strategy may be a novel, safe, efficient, and economical solution to Mirizzi syndrome, achieving both diagnostic and therapeutic goals.
Endoscopy_UCTN_Code_TTT_1AR_2AH
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wu J Cai SY Chen XL Mirizzi syndrome: Problems and strategies Hepatobiliary Pancreat Dis Int 20242323424010.1016/j.hbpd.2024.01.00538326157 · doi ↗ · pubmed ↗
- 2Valderrama-Treviño AI Granados-Romero JJ Espejel-Deloiza M Updates in Mirizzi syndrome Hepatobiliary Surg Nutr 2017617017810.21037/hbsn.2016.11.0128653000 PMC 5474450 · doi ↗ · pubmed ↗
- 3Guo Q Zhao J Zhang RY Laparoscopic cholecystectomy with non-X-ray endoscopic retrograde cholangiopancreatography for simultaneous common bile duct stone extraction Br J Surg 2024111 znad 44710.1093/bjs/znad 44738226555 · doi ↗ · pubmed ↗
- 4Liu WH Huang XY Hu X Initial experience of visualized biliary cannulation during ERCP Endoscopy 2023551037104237339664 10.1055/a-2113-8952 · doi ↗ · pubmed ↗